Pt 311 Neuroscience
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fetal Brain Anomalies Associated with Ventriculomegaly Or Asymmetry: an MRI-Based Study
ORIGINAL RESEARCH PEDIATRICS Fetal Brain Anomalies Associated with Ventriculomegaly or Asymmetry: An MRI-Based Study X E. Barzilay, X O. Bar-Yosef, X S. Dorembus, X R. Achiron, and X E. Katorza ABSTRACT BACKGROUND AND PURPOSE: Fetal lateral ventriculomegaly is a relatively common finding with much debate over its clinical signifi- cance. The purpose of this study was to examine the association between ventriculomegaly and asymmetry and concomitant CNS findings as seen in fetal brain MR imaging. MATERIALS AND METHODS: Fetal brain MR imaging performed for various indications, including ventriculomegaly, with or without additional ultrasound findings, was assessed for possible inclusion. Two hundred seventy-eight cases found to have at least 1 lateral ventricle with a width of Ն10 mm were included in the study. Ventriculomegaly was considered mild if the measurement was 10–11.9 mm; moderate if, 12–14.9 mm; and severe if, Ն15 mm. Asymmetry was defined as a difference of Ն2 mm between the 2 lateral ventricles. Fetal brain MR imaging findings were classified according to severity by predefined categories. RESULTS: The risk of CNS findings appears to be strongly related to the width of the ventricle (OR, 1.38; 95% CI, 1.08–1.76; P ϭ .009). The prevalence of associated CNS abnormalities was significantly higher (P ϭ .005) in symmetric ventriculomegaly compared with asymmetric ventriculomegaly (38.8% versus 24.2%, respectively, for all CNS abnormalities and 20% versus 7.1%, respectively, for major CNS abnormalities). CONCLUSIONS: In this study, we demonstrate that the rate of minor and major findings increased with each millimeter increase in ventricle width and that the presence of symmetric ventricles in mild and moderate ventriculomegaly was a prognostic indicator for CNS abnormalities. -

Telovelar Approach to the Fourth Ventricle: Microsurgical Anatomy
J Neurosurg 92:812–823, 2000 Telovelar approach to the fourth ventricle: microsurgical anatomy ANTONIO C. M. MUSSI, M.D., AND ALBERT L. RHOTON, JR., M.D. Department of Neurological Surgery, University of Florida, Gainesville, Florida Object. In the past, access to the fourth ventricle was obtained by splitting the vermis or removing part of the cere- bellum. The purpose of this study was to examine the access to the fourth ventricle achieved by opening the tela cho- roidea and inferior medullary velum, the two thin sheets of tissue that form the lower half of the roof of the fourth ven- tricle, without incising or removing part of the cerebellum. Methods. Fifty formalin-fixed specimens, in which the arteries were perfused with red silicone and the veins with blue silicone, provided the material for this study. The dissections were performed in a stepwise manner to simulate the exposure that can be obtained by retracting the cerebellar tonsils and opening the tela choroidea and inferior medullary velum. Conclusions. Gently displacing the tonsils laterally exposes both the tela choroidea and the inferior medullary velum. Opening the tela provides access to the floor and body of the ventricle from the aqueduct to the obex. The additional opening of the velum provides access to the superior half of the roof of the ventricle, the fastigium, and the superolater- al recess. Elevating the tonsillar surface away from the posterolateral medulla exposes the tela, which covers the later- al recess, and opening this tela exposes the structure forming -

Sylvian Aqueduct Syndrome and Global Rostral Midbrain Dysfunction Associated with Shunt Malfunction
Sylvian aqueduct syndrome and global rostral midbrain dysfunction associated with shunt malfunction Giuseppe Cinalli, M.D., Christian Sainte-Rose, M.D., Isabelle Simon, M.D., Guillaume Lot, M.D., and Spiros Sgouros, M.D. Department of Pediatric Neurosurgery and Pediatric Radiology, Hôpital Necker•Enfants Malades, Université René Decartes; and Department of Neurosurgery, Hôpital Lariboisiere, Paris, France Object. This study is a retrospective analysis of clinical data obtained in 28 patients affected by obstructive hydrocephalus who presented with signs of midbrain dysfunction during episodes of shunt malfunction. Methods. All patients presented with an upward gaze palsy, sometimes associated with other signs of oculomotor dysfunction. In seven cases the ocular signs remained isolated and resolved rapidly after shunt revision. In 21 cases the ocular signs were variably associated with other clinical manifestations such as pyramidal and extrapyramidal deficits, memory disturbances, mutism, or alterations in consciousness. Resolution of these symptoms after shunt revision was usually slow. In four cases a transient paradoxical aggravation was observed at the time of shunt revision. In 11 cases ventriculocisternostomy allowed resolution of the symptoms and withdrawal of the shunt. Simultaneous supratentorial and infratentorial intracranial pressure recordings performed in seven of the patients showed a pressure gradient between the supratentorial and infratentorial compartments with a higher supratentorial pressure before shunt revision. Inversion of this pressure gradient was observed after shunt revision and resolution of the gradient was observed in one case after third ventriculostomy. In six recent cases, a focal midbrain hyperintensity was evidenced on T2-weighted magnetic resonance imaging sequences at the time of shunt malfunction. This rapidly resolved after the patient underwent third ventriculostomy. -

Meninges Ventricles And
Meninges ,ventricles & CSF Dr.Sanaa Al-Shaarawy Dr. Essam Eldin Salama OBJECTIVES • By the end of the lecture the student should be able to: • Describe the cerebral meninges & list the main dural folds. • Describe the spinal meninges & locate the level of the termination of each of them. • Describe the importance of the subarachnoid space. • List the Ventricular system of the CNS and locate the site of each of them. • Describe the formation, circulation, drainage, and functions of the CSF. • Know some clinical point about the CSF MENINGES • The brain and spinal cord are invested by three concentric membranes ; • The outermost layer is the dura matter. • The middle layer is the arachnoid matter. • The innermost layer is the pia matter. DURA MATER ▪The cranial dura is a two layered tough, fibrous thick membrane that surrounds the brain. ▪It is formed of two layers; periosteal and meningeal. ▪The periosteal layer is attached to the skull. ▪The meningeal layer is folded forming the dural folds : falx cerebri, and tentorium cerebelli. ▪Sensory innervation of the dura is mostly from : meningeal branches of the trigeminal and vagus nerves & C1 to C3(upper cervical Ns.). DURA MATER Folds Two large reflection of dura extend into the cranial cavity : 1.The falx cerebri, In the midline, ▪It is a vertical sickle-shaped sheet of dura, extends from the cranial roof into the great longitudinal fissure between the two cerebral hemispheres. ▪It has an attached border adherent to the skull. ▪And a free border lies above the corpus callosum. DURA MATER Folds 2. A horizontal shelf of dura, The tentorium cerebelli, ▪ It lies between the posterior part of the cerebral hemispheres and the cerebellum. -

Neuromelanin Marks the Spot: Identifying a Locus Coeruleus Biomarker of Cognitive Reserve in Healthy Aging
Neurobiology of Aging xxx (2015) 1e10 Contents lists available at ScienceDirect Neurobiology of Aging journal homepage: www.elsevier.com/locate/neuaging Neuromelanin marks the spot: identifying a locus coeruleus biomarker of cognitive reserve in healthy aging David V. Clewett a,*, Tae-Ho Lee b, Steven Greening b,c,d, Allison Ponzio c, Eshed Margalit e, Mara Mather a,b,c a Neuroscience Graduate Program, University of Southern California, Los Angeles, CA, USA b Department of Psychology, University of Southern California, Los Angeles, CA, USA c Davis School of Gerontology, University of Southern California, Los Angeles, CA, USA d Department of Psychology, Louisiana State University, Baton Rouge, LA, USA e Dornsife College of Letters and Sciences, University of Southern California, Los Angeles, CA, USA article info abstract Article history: Leading a mentally stimulating life may build up a reserve of neural and mental resources that preserve Received 28 May 2015 cognitive abilities in late life. Recent autopsy evidence links neuronal density in the locus coeruleus (LC), Received in revised form 18 September 2015 the brain’s main source of norepinephrine, to slower cognitive decline before death, inspiring the idea Accepted 23 September 2015 that the noradrenergic system is a key component of reserve (Robertson, I. H. 2013. A noradrenergic theory of cognitive reserve: implications for Alzheimer’s disease. Neurobiol. Aging. 34, 298e308). Here, we tested this hypothesis using neuromelanin-sensitive magnetic resonance imaging to visualize and Keywords: measure LC signal intensity in healthy younger and older adults. Established proxies of reserve, including Locus coeruleus Aging education, occupational attainment, and verbal intelligence, were linearly correlated with LC signal in- fi Norepinephrine tensity in both age groups. -
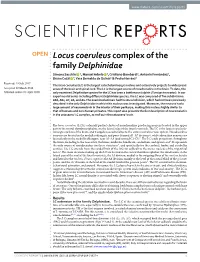
Locus Coeruleus Complex of the Family Delphinidae
www.nature.com/scientificreports OPEN Locus coeruleus complex of the family Delphinidae Simona Sacchini 1, Manuel Arbelo 1, Cristiano Bombardi2, Antonio Fernández1, Bruno Cozzi 3, Yara Bernaldo de Quirós1 & Pedro Herráez1 Received: 19 July 2017 The locus coeruleus (LC) is the largest catecholaminergic nucleus and extensively projects to widespread Accepted: 22 March 2018 areas of the brain and spinal cord. The LC is the largest source of noradrenaline in the brain. To date, the Published: xx xx xxxx only examined Delphinidae species for the LC has been a bottlenose dolphin (Tursiops truncatus). In our experimental series including diferent Delphinidae species, the LC was composed of fve subdivisions: A6d, A6v, A7, A5, and A4. The examined animals had the A4 subdivision, which had not been previously described in the only Delphinidae in which this nucleus was investigated. Moreover, the neurons had a large amount of neuromelanin in the interior of their perikarya, making this nucleus highly similar to that of humans and non-human primates. This report also presents the frst description of neuromelanin in the cetaceans’ LC complex, as well as in the cetaceans’ brain. Te locus coeruleus (LC) is a densely packed cluster of noradrenaline-producing neurons located in the upper part of the rostral rhombencephalon, on the lateral edge of the fourth ventricle. Te LC is the largest catechola- minergic nucleus of the brain, and it supplies noradrenaline to the entire central nervous system. Noradrenaline neurons are located in the medulla oblongata and pons (termed A1-A7 divisions), while adrenaline neurons are located only in the medulla oblongata, near A1-A3 (and termed C1-C3)1. -

The Surgical Treatment of Tumors of the Fourth Ventricle: a Single-Institution Experience
CLINICAL ARTICLE J Neurosurg 128:339–351, 2018 The surgical treatment of tumors of the fourth ventricle: a single-institution experience Sherise D. Ferguson, MD, Nicholas B. Levine, MD, Dima Suki, PhD, Andrew J. Tsung, MD, Fredrick F. Lang, MD, Raymond Sawaya, MD, Jeffrey S. Weinberg, MD, and Ian E. McCutcheon, MD, FRCS(C) Department of Neurosurgery, The University of Texas MD Anderson Cancer Center, Houston, Texas OBJECTIVE Fourth ventricle tumors are rare, and surgical series are typically small, comprising a single pathology, or focused exclusively on pediatric populations. This study investigated surgical outcome and complications following fourth ventricle tumor resection in a diverse patient population. This is the largest cohort of fourth ventricle tumors described in the literature to date. METHODS This is an 18-year (1993–2010) retrospective review of 55 cases involving patients undergoing surgery for tumors of the fourth ventricle. Data included patient demographic characteristics, pathological and radiographic tumor characteristics, and surgical factors (approach, surgical adjuncts, extent of resection, etc.). The neurological and medical complications following resection were collected and outcomes at 30 days, 90 days, 6 months, and 1 year were reviewed to determine patient recovery. Patient, tumor, and surgical factors were analyzed to determine factors associated with the frequently encountered postoperative neurological complications. RESULTS There were no postoperative deaths. Gross-total resection was achieved in 75% of cases. Forty-five percent of patients experienced at least 1 major neurological complication, while 31% had minor complications only. New or worsening gait/focal motor disturbance (56%), speech/swallowing deficits (38%), and cranial nerve deficits (31%) were the most common neurological deficits in the immediate postoperative period. -
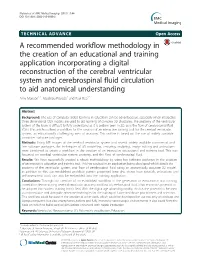
A Recommended Workflow Methodology in the Creation of An
Manson et al. BMC Medical Imaging (2015) 15:44 DOI 10.1186/s12880-015-0088-6 TECHNICAL ADVANCE Open Access A recommended workflow methodology in the creation of an educational and training application incorporating a digital reconstruction of the cerebral ventricular system and cerebrospinal fluid circulation to aid anatomical understanding Amy Manson1,2, Matthieu Poyade2 and Paul Rea1* Abstract Background: The use of computer-aided learning in education can be advantageous, especially when interactive three-dimensional (3D) models are used to aid learning of complex 3D structures. The anatomy of the ventricular system of the brain is difficult to fully understand as it is seldom seen in 3D, as is the flow of cerebrospinal fluid (CSF). This article outlines a workflow for the creation of an interactive training tool for the cerebral ventricular system, an educationally challenging area of anatomy. This outline is based on the use of widely available computer software packages. Methods: Using MR images of the cerebral ventricular system and several widely available commercial and free software packages, the techniques of 3D modelling, texturing, sculpting, image editing and animations were combined to create a workflow in the creation of an interactive educational and training tool. This was focussed on cerebral ventricular system anatomy, and the flow of cerebrospinal fluid. Results: We have successfully created a robust methodology by using key software packages in the creation of an interactive education and training tool. This has resulted in an application being developed which details the anatomy of the ventricular system, and flow of cerebrospinal fluid using an anatomically accurate 3D model. -

Craniopharyngioma in the Third Ventricle: Necropsy Findings and Histogenesis
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.50.8.1053 on 1 August 1987. Downloaded from Journal ofNeurology, Neurosurgery, and Psychiatry 1987;50:1053-1056 Short report Craniopharyngioma in the third ventricle: necropsy findings and histogenesis KATSUZO KUNISHIO, YUJI YAMAMOTO, NORIO SUNAMI, SHOJI ASARI, TADAATSU AKAGI,* YUJI OHTSUKI* From the Department ofNeurological Surgery, Matsuyama Shimin Hospital, Ehime and Department Of Pathology,* Kochi Medical School, Kochi, Japan SUMMARY A case of craniopharyngioma confined within the third ventricle with necropsy is re- ported. A stalk-like structure in this tumour was present in the wall of the third ventricle at its base. It is suggested that this tumour might have arisen from the remnants of Rathke's pouch persisting in the tuber cinereum. Craniopharyngiomas have been considered to be de- or slightly low-density mass (mean Hounsfield units (HU): rived from remnants of Rathke's pouch, which is 30) occupying the third ventricle, and the lateral ventricles Protected by copyright. thought to lie in the superior aspect of the pituitary were dilated. With contrast medium there was homogeneous enhancement (mean HU: 68) of the entire mass situated in stalk and infundibulum. They commonly occupy the the third ventricle. Coronal CT scans showed that an en- suprasellar cistern and may occasionally spread into hanced mass seemed to be separated from the sella turcica the anterior, middle, or posterior cranial fossae, as and confined to the third ventricle. Conray ventriculography well as into the sella turcica. Craniopharyngioma showed a large mass almost completely filling the anterior confined to the third ventricle, however, is rare. -

Split Cerebral Aqueduct: a Neuroendoscopic Illustration
Split cerebral aqueduct: a neuroendoscopic illustration Alberto Feletti, Alessandro Fiorindi & Pierluigi Longatti Child's Nervous System ISSN 0256-7040 Volume 32 Number 1 Childs Nerv Syst (2016) 32:199-203 DOI 10.1007/s00381-015-2827-y 1 23 Your article is protected by copyright and all rights are held exclusively by Springer- Verlag Berlin Heidelberg. This e-offprint is for personal use only and shall not be self- archived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. The link must be accompanied by the following text: "The final publication is available at link.springer.com”. 1 23 Author's personal copy Childs Nerv Syst (2016) 32:199–203 DOI 10.1007/s00381-015-2827-y CASE REPORT Split cerebral aqueduct: a neuroendoscopic illustration Alberto Feletti1 & Alessandro Fiorindi2 & Pierluigi Longatti2 Received: 30 June 2015 /Accepted: 9 July 2015 /Published online: 1 August 2015 # Springer-Verlag Berlin Heidelberg 2015 Abstract Introduction Purpose Forking of the cerebral aqueduct is a developmental malformation that is infrequently encountered by neurosur- Although some authors have described the forking of the ce- geons as a rare cause of hydrocephalus, sometimes with a rebral aqueduct (CA) as a common cause of hydrocephalus, a delayed onset. -

Neuroanatomy Dr
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Prof Yousry 10/15/17 A F B K G C H D I M E N J L Ventricular System, The Cerebrospinal Fluid, and the Blood Brain Barrier The lateral ventricle Interventricular foramen It is Y-shaped cavity in the cerebral hemisphere with the following parts: trigone 1) A central part (body): Extends from the interventricular foramen to the splenium of corpus callosum. 2) 3 horns: - Anterior horn: Lies in the frontal lobe in front of the interventricular foramen. - Posterior horn : Lies in the occipital lobe. - Inferior horn : Lies in the temporal lobe. rd It is connected to the 3 ventricle by body interventricular foramen (of Monro). Anterior Trigone (atrium): the part of the body at the horn junction of inferior and posterior horns Contains the glomus (choroid plexus tuft) calcified in adult (x-ray&CT). Interventricular foramen Relations of Body of the lateral ventricle Roof : body of the Corpus callosum Floor: body of Caudate Nucleus and body of the thalamus. Stria terminalis between thalamus and caudate. (connects between amygdala and venteral nucleus of the hypothalmus) Medial wall: Septum Pellucidum Body of the fornix (choroid fissure between fornix and thalamus (choroid plexus) Relations of lateral ventricle body Anterior horn Choroid fissure Relations of Anterior horn of the lateral ventricle Roof : genu of the Corpus callosum Floor: Head of Caudate Nucleus Medial wall: Rostrum of corpus callosum Septum Pellucidum Anterior column of the fornix Relations of Posterior horn of the lateral ventricle •Roof and lateral wall Tapetum of the corpus callosum Optic radiation lying against the tapetum in the lateral wall. -

Ventriculomegaly
Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Ventriculomegaly This information sheet from Great Ormond Street Hospital (GOSH) explains the causes, symptoms and treatment of ventriculomegaly and hydrocephalus and where to get help. Ventricles are cavities within the brain filled Without signs of increased pressure in the with cerebro-spinal fluid (CSF) acting as a brain (hydrocephalus), ventriculomegaly most ‘cushion’. CSF also supplies nutrients to the likely will not cause any problems. However, brain. The brain has four ventricles: two it can be linked with hydrocephalus and other lateral ventricles, the third ventricle and the problems. Ventriculomegaly can be diagnosed fourth ventricle. during pregnancy and occurs in around two CSF is created within the brain and flows from per cent of all pregnancies. the lateral ventricles into the third ventricle. It then flows through a narrow tube (the What causes cerebral aqueduct) into the fourth ventricle which lies towards the base of the brain. From ventriculomegaly? the fourth ventricle, it flows around the spinal In many cases, we do not know what causes cord and over the surface of the brain before ventriculomegaly (in the absence of any raised being re-absorbed. CSF pressure) but it can occur if there has been Ventriculomegaly is the medical term used to brain damage for any reason leading to loss describe enlargement of the ventricles of the of brain tissue. Often however it is a “chance” brain. Hydrocephalus is the term used when finding and when the ventricles are only a enlargement of the ventricles has been caused little enlarged of little significance.