Clover Handbook 05.11.18
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Local Business Database Local Business Database: Alphabetical Listing
Local Business Database Local Business Database: Alphabetical Listing Business Name City State Category 111 Chop House Worcester MA Restaurants 122 Diner Holden MA Restaurants 1369 Coffee House Cambridge MA Coffee 180FitGym Springfield MA Sports and Recreation 202 Liquors Holyoke MA Beer, Wine and Spirits 21st Amendment Boston MA Restaurants 25 Central Northampton MA Retail 2nd Street Baking Co Turners Falls MA Food and Beverage 3A Cafe Plymouth MA Restaurants 4 Bros Bistro West Yarmouth MA Restaurants 4 Family Charlemont MA Travel & Transportation 5 and 10 Antique Gallery Deerfield MA Retail 5 Star Supermarket Springfield MA Supermarkets and Groceries 7 B's Bar and Grill Westfield MA Restaurants 7 Nana Japanese Steakhouse Worcester MA Restaurants 76 Discount Liquors Westfield MA Beer, Wine and Spirits 7a Foods West Tisbury MA Restaurants 7B's Bar and Grill Westfield MA Restaurants 7th Wave Restaurant Rockport MA Restaurants 9 Tastes Cambridge MA Restaurants 90 Main Eatery Charlemont MA Restaurants 90 Meat Outlet Springfield MA Food and Beverage 906 Homwin Chinese Restaurant Springfield MA Restaurants 99 Nail Salon Milford MA Beauty and Spa A Child's Garden Northampton MA Retail A Cut Above Florist Chicopee MA Florists A Heart for Art Shelburne Falls MA Retail A J Tomaiolo Italian Restaurant Northborough MA Restaurants A J's Apollos Market Mattapan MA Convenience Stores A New Face Skin Care & Body Work Montague MA Beauty and Spa A Notch Above Northampton MA Services and Supplies A Street Liquors Hull MA Beer, Wine and Spirits A Taste of Vietnam Leominster MA Pizza A Turning Point Turners Falls MA Beauty and Spa A Valley Antiques Northampton MA Retail A. -

Clover Handbook 11.30.16
CLOVER EMPLOYEE HANDBOOK v. 11.30.16 PROPERTY OF CLOVER FAST FOOD INC. WELCOME Welcome to Clover. We’re building the future, and we need you to get it right. What does that mean? It means we make a lot of mistakes. Tons and tons of mistakes. We expect you’re going to screw some things up too. Maybe not as much as us, but you’re going to make mistakes, and we’re going to love you for them. That’s what doing new things is all about. But let’s make these failures work for us. To make that happen always follow these simple rules: (a) Let’s work together to make sure your mistakes don’t cost anyone. That means don’t get hurt, don’t create dangerous situations for others, and don’t bust my fryer, seriously. (b) We’re going to ask you to learn (and help us learn) from EVERY SINGLE mistake you make. We love NEW MISTAKES (as long as they don’t cost anyone, see above), but we hate seeing the same mistakes again and again. Over the coming weeks we want you to learn as much as you can as quickly as possible. You’re going to learn what clean looks like, how to keep up with lines that grow larger everyday, and you may even learn what a “Gordon” is. Above all you’re going to get to know our food. And we’re going to be there with you along the way to provide the support you need. You’re going to help us make Clover better than it is today. -

Menu Forecast: 2020 and Beyond Nancy Kruse, the Kruse Company Lizzy Freier, Technomic, Inc
Menu Forecast: 2020 and Beyond Nancy Kruse, The Kruse Company Lizzy Freier, Technomic, Inc. Menus 2020: Introduction Restaurateurs are bombarded by info, inputs Challenge: Sort through hype and hoopla Opportunity: Identify foods and flavors with appeal Objective: Put trends to work in your operation for your customers and your bottom line 2 Menu Size Relatively Stable; Deeper Dive Reveals Volatility Five-year item count change Add-On Kids Menu Adult Beverage Nonalcohol Side +32.5% +15.4% 4.3% Beverage +3.2% +3.3% Overall -1.2% Dessert Entree Appetizer Senior Menu -0.6% -3.4% -3.7% -12.2% Source: Technomic Ignite menu data 3 Action Shifts to LTOs, Specials and Add-Ons 23 Entree 18 Appetizer Categories Categories Five-Year LTO Change +63.9% 3 6 YOY YOY Source: Technomic Ignite menu data 4 Menus 2020 Agenda Health Asian Middle Eastern The Next Big Thing 5 Healthful: 9% 14% 2020 and Beyond 7% “I’m eating more food because of its 20% specific nutritional 20% benefits than I did two years ago.” Agree completely Agree Somewhat agree Somewhat disagree 30% Disagree Disagree completely Source: Technomic 2018 Healthy Eating Consumer Trend Report 6 Trendy Diet Plans Fuel New Dishes Options: • Paleo 38% of • Keto consumers would try • Whole 30 • Vegetarian • Gluten-Free Source: Technomic 2018 Healthy Eating Consumer Trend Report 7 Gluten-Free Still Trending? Yes, But So Are Good Grains Panera reveals whole-grain content of breads • Clarify exact whole-grain content • Avoid misleading labeling BBQ Chicken on Whole Grain Flatbread 8 Dining Law of Physics: -

Clover Handbook 4.3.15
CLOVER EMPLOYEE HANDBOOK v. 4.3.15 PROPERTY OF CLOVER FAST FOOD INC. WELCOME Welcome to Clover. We’re building the future, and we need you to get it right. What does that mean? It means we make a lot of mistakes. Tons and tons of mistakes. We expect you’re going to screw some things up too. Maybe not as much as us, but you’re going to make mistakes, and we’re going to love you for them. That’s what doing new things is all about. But let’s make these failures work for us. To make that happen always follow these simple rules: (a) Let’s work together to make sure your mistakes don’t cost anyone. That means don’t get hurt, don’t create dangerous situations for others, and don’t bust my fryer, seriously. (b) We’re going to ask you to learn (and help us learn) from EVERY SINGLE mistake you make. We love NEW MISTAKES (as long as they don’t cost anyone, see above), but we hate seeing the same mistakes again and again. Over the coming weeks we want you to learn as much as you can as quickly as possible. You’re going to learn what clean looks like, how to keep up with lines that grow larger everyday, and you may even learn what a “Gordon” is. Above all you’re going to get to know our food. And we’re going to be there with you along the way to provide the support you need. You’re going to help us make Clover better than it is today. -
Typecon 2017 Walking Guide to Boston
Cover art features an illustration of the iconic statue dedicated to Make Way for Ducklings, a classic children’s book set in Beantown. Designed TypeCon 2017 by Nancy Schön and located in the Public Garden, the ducks are local celebrities, and are typically dressed up for holidays and the playoffs. There’s Walking Guide even a parade in their honor on Duckling Day. to Boston Food. Booze. Museums. Events. Touristy Things. We’ve got you covered. Welcome to Boston! Since 1630, Boston has been one of the country’s most rebellious cities. Here you’ll fnd a spirit of independence that transcends generations, and a culture of innovation that has inspired the best and brightest minds for centuries. Boston is one of the most walkable cities in America, so be sure to wander the countless parks, visit landmarks such as the Old North Church and Fenway Park, and get lost amidst the cobblestone alleys and brownstone row houses of Boston’s neighborhoods. Boston has some of the best restaurants in the country, not to mention world-class cultural institutions like the MFA and New England Aquarium. And throw Cambridge some love too! From Harvard to MIT to artsy Central Square, the People’s Republic is a unique city unto itself. —Written by Carl Unger, Monotype Zakim Bridge North What’s in here? End 1 Workshops & Food Nearby West 3 Coffee & Breakfast End 5 Cheap Eats 7 10 Minute Walk 9 15 Minute Walk Govt. Waterfront 11 Worth the Walk Center 13 Food Trucks Beacon 15 Seafood Spots Hill 17 Dollar Oysters Financial 19 Good for Groups Downtown Crossing 21 Money to Burn 23 Breweries & Booze Back 25 City Happenings Bay TC 27 Museums Theatre Chinatown Leather District Bay Village Fenway Seaport South End 1 Workshops TC Hotel: ve es A am Boston Park Plaza St. -

Property of Clover Fast Food Inc. Clover
CLOVER EMPLOYEE HANDBOOK v. 5.5.17 PROPERTY OF CLOVER FAST FOOD INC. WELCOME Welcome to Clover. We’re building the future, and we need you to get it right. What does that mean? It means we make a lot of mistakes. Tons and tons of mistakes. We expect you’re going to screw some things up too. Maybe not as much as us, but you’re going to make mistakes, and we’re going to love you for them. That’s what doing new things is all about. But let’s make these failures work for us. To make that happen always follow these simple rules: (a) Let’s work together to make sure your mistakes don’t cost anyone. That means don’t get hurt, don’t create dangerous situations for others, and don’t bust my fryer, seriously. (b) We’re going to ask you to learn (and help us learn) from EVERY SINGLE mistake you make. We love NEW MISTAKES (as long as they don’t cost anyone, see above), but we hate seeing the same mistakes again and again. Over the coming weeks we want you to learn as much as you can as quickly as possible. You’re going to learn what clean looks like, how to keep up with lines that grow larger everyday, and you may even learn what a “Gordon” is. Above all you’re going to get to know our food. And we’re going to be there with you along the way to provide the support you need. You’re going to help us make Clover better than it is today. -

Property of Clover Fast Food Inc. Clover
CLOVER EMPLOYEE HANDBOOK v. 7.26.17 PROPERTY OF CLOVER FAST FOOD INC. WELCOME Welcome to Clover. We’re building the future, and we need you to get it right. What does that mean? It means we make a lot of mistakes. Tons and tons of mistakes. We expect you’re going to screw some things up too. Maybe not as much as us, but you’re going to make mistakes, and we’re going to love you for them. That’s what doing new things is all about. But let’s make these failures work for us. To make that happen always follow these simple rules: (a) Let’s work together to make sure your mistakes don’t cost anyone. That means don’t get hurt, don’t create dangerous situations for others, and don’t bust my fryer, seriously. (b) We’re going to ask you to learn (and help us learn) from EVERY SINGLE mistake you make. We love NEW MISTAKES (as long as they don’t cost anyone, see above), but we hate seeing the same mistakes again and again. Over the coming weeks we want you to learn as much as you can as quickly as possible. You’re going to learn what clean looks like, how to keep up with lines that grow larger everyday, and you may even learn what a “Gordon” is. Above all you’re going to get to know our food. And we’re going to be there with you along the way to provide the support you need. You’re going to help us make Clover better than it is today. -

Teacher's Guide
TEACHER’S GUIDE V. 12.5.14 Introduction to the Clover Teacher’s Guide Welcome. You’re either about to train somebody, or curious about how we train. Here are the most up-to-date methods we use at Clover. Training is the backbone of our company. It’s how we bring new people into our family, share with them all that we’ve worked so hard to build and prepare them to work with us to achieve great things. As you use this guide please try to think back to what it feels like to learn something new. Stop for a second and remember that feeling. It can be scary, frustrating, exciting, confusing. We’re working hard with these materials to give you the tools you need to connect with your employees. We’ve deliberately used a bunch of different media formats with the hope that there will be something for every learning style. Make the training fun. How hard did you work to learn the rules of your favorite sport? Learning through play can not only feel painless but it can be extremely effective. Think about how to make this fun for your employees. Use this to better understand the training tools, use it as a reference, use it for inspiration. If you have ideas/improvements share them. You can help us make this guide better. You will find aspects of the training are deliberately open-ended. Just as in many other places in our company, you’ll notice consistent directions for how to train whether someone is learning to make a sandwich or open up a restaurant in the morning. -

Restaurants United
*FOR URGENT CONSIDERATION AND IMMEDIATE DISSEMINATION* MASSACHUSETTS RESTAURANTS UNITED March 21, 2020 Hon. Charlie Baker, Governor Hon. Karen Polito, Lt. Governor Hon. Robert De Leo, Speaker of the House of Representative Hon. Karen Spilka, President of the Senate Dear Gov. Baker, Lt. Gov. Polito, Speaker De Leo, President Spilka, We are independent restaurant owners and operators from every corner of the Commonwealth. We are deeply invested in our neighborhoods and communities. We host the gathering places, the hang outs, the places where everyone knows your name, the go-to celebration space, the go-to mourning place in times of tragedy – we’re always there for whomever needs us, whenever they need us. Now we need you. Earlier this week, we circulated a draft of this letter. We hope that this letter made its way to all of you, and we thank you for taking the time to read it – we understand how overwhelming and fluid this situation is. We understand that you, and your teams are working diligently and bravely to steer us through this public health crisis. Thank you for your leadership, and for the steps you have taken thus far. This updated letter is meant to serve as a concise, actionable, and focused list of requests from an industry that may never recover. We believe that with action now, the restaurant industry will lead the Commonwealth’s economic recovery from Covid-19. As an industry, there is no denying the collective economic impact of 350,000 hospitality workers, 16,000 businesses, and $18.7 billion in sales. More than just numbers, restaurants participate in almost every facet of the Commonwealth’s economic food chain. -
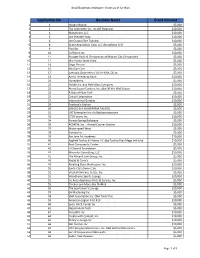
Application No. Business Name Grant Amount
Small Businesss Assistance Grants as of 12/18/20 Application No. Business Name Grant Amount 1 1 Hungry Hound $5,000 2 2 The Crittenden Co., Inc (JB Trophies) $10,000 3 4 Makaboom, LLC $10,000 4 5 Just Breathe Yoga $10,000 5 6 Joe Grasso Elite Training $10,000 6 8 Grace Acquisition Corp. LLC dba Athena Grill $5,000 7 9 Fiorillos $5,000 8 10 Cal Micro Inc. $10,000 9 11 Bourget Body & Chiropractic at Mission City Chiropractic $5,000 10 12 Mio Vicino Santa Clara $5,000 11 14 Gogo Pho Inc $5,000 12 15 Alta Eye Care $5,000 13 17 Eyetopia Optometry / LILY H KIM, OD pc $5,000 14 18 Aarna Threading Salon $10,000 15 20 HoneyBerry $5,000 16 21 Holder Inc. dba Able Glass Company $10,000 17 22 Arena Soccer Centers, Inc. dba Off the Wall Soccer $10,000 18 23 A Slice of New York $5,000 19 25 Calculi Corporation $10,000 20 27 International Gurukul $10,000 21 29 Poorboy's Kitchen $5,000 22 30 SHAQ D.B.A SHAWARMA FALAFEL $5,000 23 31 LNT Enterprise Inc c/o Beijing restaurant $5,000 24 33 CTO Forum, Inc. $10,000 25 34 Korean Spring Barbeque $5,000 26 36 ACSATM, Inc. - Armed Courier Service $10,000 27 37 Motorspeed West $5,000 28 38 Sumiya Inc. $5,000 29 39 San Jose Art Academy $10,000 30 40 Applied Tactics & Fitness LLC dba Tactica Krav Maga Institute $10,000 31 41 Best Chiropractic Center $5,000 32 42 U Channel Foundation $5,000 33 44 Mirandus Consulting, LLC $10,000 34 45 The Mlnarik Law Group, Inc. -

25 Years in Harvard Square What’S Changed, What Hasn’T, and Why • by Nell Porter Brown
EXPLOrATIOns 25 Years in Harvard Square What’s changed, what hasn’t, and why • by Nell Porter Brown The Square has always attracted those who want to shop, eat, gawk, and play. ciation, which celebrated its centennial last year. “But the young people who are just discovering the Square now will have their own favorite places and memories, and come back in 60 years and will still say, ‘It’s not the way it used to be.’ The Square is, and I hope always will be, a unique place.” A dynamic microcosm, the Square has keenly reflected its times throughout its his- tory. During the last 25 years it has changed dramatically, due in part to a real-estate boom and demand for more offices, housing, and parking spaces. “There are the obvi- ous changes of new develop- ment, which is larger in scale visitor from Kansas City films at the Janus. And, of course, burgers than the older buildings,” says Kathy Spie- who had never been to Har- and banter at the Tasty, whose controver- gelman, a former long-time University vard Square recently strolled sial loss in 1997 and later transformation planning administrator. Upscale retailers A through it and then enjoyed a into an Abercrombie & Fitch—and now a and service-oriented establishments that grilled salmon dinner at The Harvest res- Citizens Bank—is still a source of outrage catered to visitors followed—“more chain taurant. “The Square is wild,” the man among many. stores, more banks and phone stores,” said, his eyes gleaming with appreciation. For every generation, it seems, the she notes, “and fewer bookstores, no mu- “There’s so much going on. -
Harvard Square Storefront Survey
(Academic) Cambridge Artists Cooperative Harvard Square Christian Science Reading Room Dunkin Donuts Cambridge, 1. Raven Used Books Storefront Businesses Fjällräven Lizzy's First Parish in Cambridge Market in the Square Starbucks and Other Uses The Just Crust (Vacant) Swiss Watchmaker Mint Julep Hillside Cleaners Esmerelda Cambridge, Massachusetts Custom Barber Shop (Vacant) Liquiterie Dado Tea LF Aesop T-Mobile Club Passim C'est Bon Market & Liquors Anthropologie Border Cafe OTTO Harvard Global Health Institute Ann Taylor College House Harvest Change is Constant Harvard Coop Origins CVS Pharmacy Concepts Clover Food Lab Beat Brasserie Cardullo's Santander Goorin Bros. Hat Shop Crimson Corner (Academic) Cambridge Center for Black Ink Bank of America Moleskine Motto Adult Education (Office) Harvard Shirt Shop Flat Patties Rebekah (Vacant) CVS Pharmacy United States Postal Service Alden & Harlow Brooks (Vacant) (Vacant) Starbucks Leavitt & Perice Brattle Theatre Gap Algiers Pressed Juicery FedEx Office Brattle Square Florist The Curious JP Licks Sweet George Cambridge Savings Bank Monella Gnomon Copy Webster Bank Dickson Tess Tealuxe Store !!T (Residential) Crema Cafe Chipotle Bros. (Residential) Felix Shoe Repair Visionworks Felipe's Taqueria Vision House Russel House Tavern Cabot's Candy Bob Slate Stationer Concepts Smith Campus Center Papyrus Mike's Pastry Zinnia (Residential) Urban Outfitters Q'doba Harvard University Employees The Million Year Picnic (Vacant) Credit Union Plan B Cut & Color Boutique Capital One (cafe) Tatte Flour Bakery & Cafe Hair Cuttery Hunt's Photo & Video Sweetgreen Cambridge Trust See Eyewear Verizon David's Tea b.good Lush Cosmetics Company TD Bank Harvard Square Hotel AT&T (Vacant) The Hourly Oyster House Harvard Book Store MedCap Advisors Whitney's (Vacant) The Cooper Gallery (Vacant) The Garage Harvard Square Eye Care Mr.