Sexually Transmitted Diseases Act)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Insights Into the Pathogenicity of Burkholderia Pseudomallei
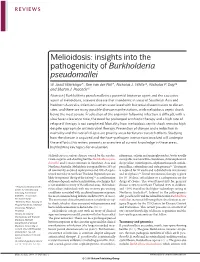
REVIEWS Melioidosis: insights into the pathogenicity of Burkholderia pseudomallei W. Joost Wiersinga*, Tom van der Poll*, Nicholas J. White‡§, Nicholas P. Day‡§ and Sharon J. Peacock‡§ Abstract | Burkholderia pseudomallei is a potential bioterror agent and the causative agent of melioidosis, a severe disease that is endemic in areas of Southeast Asia and Northern Australia. Infection is often associated with bacterial dissemination to distant sites, and there are many possible disease manifestations, with melioidosis septic shock being the most severe. Eradication of the organism following infection is difficult, with a slow fever-clearance time, the need for prolonged antibiotic therapy and a high rate of relapse if therapy is not completed. Mortality from melioidosis septic shock remains high despite appropriate antimicrobial therapy. Prevention of disease and a reduction in mortality and the rate of relapse are priority areas for future research efforts. Studying how the disease is acquired and the host–pathogen interactions involved will underpin these efforts; this review presents an overview of current knowledge in these areas, highlighting key topics for evaluation. Melioidosis is a serious disease caused by the aerobic, rifamycins, colistin and aminoglycosides), but is usually Gram-negative soil-dwelling bacillus Burkholderia pseu- susceptible to amoxicillin-clavulanate, chloramphenicol, domallei and is most common in Southeast Asia and doxycycline, trimethoprim-sulphamethoxazole, ureido- Northern Australia. Melioidosis is responsible for 20% of penicillins, ceftazidime and carbapenems2,4. Treatment all community-acquired septicaemias and 40% of sepsis- is required for 20 weeks and is divided into intravenous related mortality in northeast Thailand. Reported cases are and oral phases2,4. Initial intravenous therapy is given likely to represent ‘the tip of the iceberg’1,2, as confirmation for 10–14 days; ceftazidime or a carbapenem are the of disease depends on bacterial isolation, a technique that drugs of choice. -

Characterization of the Burkholderia Cenocepacia J2315 Surface-Exposed Immunoproteome
Article Characterization of the Burkholderia cenocepacia J2315 Surface-Exposed Immunoproteome 1, 1, 1, Sílvia A. Sousa * , António M.M. Seixas y , Manoj Mandal y, Manuel J. Rodríguez-Ortega 2 and Jorge H. Leitão 1,* 1 iBB–Institute for Bioengineering and Biosciences, 1049-001 Lisbon, Portugal; [email protected] (A.M.M.S.); [email protected] (M.M.) 2 Departament of Biochemistry and Molecular Biology, Córdoba University, 14071 Córdoba, Spain; [email protected] * Correspondence: [email protected] (S.A.S.); [email protected] (J.H.L.); Tel.: +351-2184-19986 (S.A.S.); +351-2184-17688 (J.H.L.) Both authors contributed equally to the work. y Received: 31 July 2020; Accepted: 3 September 2020; Published: 6 September 2020 Abstract: Infections by the Burkholderia cepacia complex (Bcc) remain seriously life threatening to cystic fibrosis (CF) patients, and no effective eradication is available. A vaccine to protect patients against Bcc infections is a highly attractive therapeutic option, but none is available. A strategy combining the bioinformatics identification of putative surface-exposed proteins with an experimental approach encompassing the “shaving” of surface-exposed proteins with trypsin followed by peptide identification by liquid chromatography and mass spectrometry is here reported. The methodology allowed the bioinformatics identification of 263 potentially surface-exposed proteins, 16 of them also experimentally identified by the “shaving” approach. Of the proteins identified, 143 have a high probability of containing B-cell epitopes that are surface-exposed. The immunogenicity of three of these proteins was demonstrated using serum samples from Bcc-infected CF patients and Western blotting, validating the usefulness of this methodology in identifying potentially immunogenic surface-exposed proteins that might be used for the development of Bcc-protective vaccines. -
Analysis of Shigella Flexneri Cell Surface Virulence Factors
Analysis of Shigella flexneri Cell Surface Virulence Factors Min Yan Teh B. Sc. (Honours) Submitted for the degree of Doctor of Philosophy Discipline of Microbiology and Immunology The School of Molecular and Biomedical Science The University of Adelaide September 2012 Declaration This work contains no material which has been accepted for the award of any other degree or diploma in any university or other tertiary institution to Min Yan Teh and, to the best of my knowledge and belief, contains no material previously published or written by another person, except where due reference has been made in the text. I give consent to this copy of my thesis, when deposited in the University Library, being made available for loan and photocopying, subject to the provisions of the Copyright Act 1968. The author acknowledges that copyright of published works contained within this thesis resides with the copyright holder(s) of those works. I also give permission for the digital version of my thesis to be made available on the web, via the University’s digital research repository, the Library catalogue, the Australasian Digital Theses Program (ADTP) and also through web search engines, unless permission has been granted by the University to restrict access for a period of time. Adelaide, Australia, September 2012 ___________________ Min Yan Teh i ii Abstract The IcsA autotransporter (AT) is a key virulence protein of Shigella flexneri, a human pathogen that causes bacillary dysentery through invasion of colonic epithelium. IcsA is a polarly distributed, outer membrane protein that confers motility to intracellular bacteria by engaging the host actin regulatory protein, neural Wiskott-Aldrich syndrome protein (N- WASP). -

Downloaded from the NCBI Genomes Gene-Specific Primers (Additional File 22: Table S13) and Porcelli Et Al
Porcelli et al. BMC Genomics 2013, 14:616 http://www.biomedcentral.com/1471-2164/14/616 RESEARCH ARTICLE Open Access Parallel evolution of genome structure and transcriptional landscape in the Epsilonproteobacteria Ida Porcelli, Mark Reuter, Bruce M Pearson, Thomas Wilhelm and Arnoud HM van Vliet* Abstract Background: Gene reshuffling, point mutations and horizontal gene transfer contribute to bacterial genome variation, but require the genome to rewire its transcriptional circuitry to ensure that inserted, mutated or reshuffled genes are transcribed at appropriate levels. The genomes of Epsilonproteobacteria display very low synteny, due to high levels of reshuffling and reorganisation of gene order, but still share a significant number of gene orthologs allowing comparison. Here we present the primary transcriptome of the pathogenic Epsilonproteobacterium Campylobacter jejuni, and have used this for comparative and predictive transcriptomics in the Epsilonproteobacteria. Results: Differential RNA-sequencing using 454 sequencing technology was used to determine the primary transcriptome of C. jejuni NCTC 11168, which consists of 992 transcription start sites (TSS), which included 29 putative non-coding and stable RNAs, 266 intragenic (internal) TSS, and 206 antisense TSS. Several previously unknown features were identified in the C. jejuni transcriptional landscape, like leaderless mRNAs and potential leader peptides upstream of amino acid biosynthesis genes. A cross-species comparison of the primary transcriptomes of C. jejuni and the related Epsilonproteobacterium Helicobacter pylori highlighted a lack of conservation of operon organisation, position of intragenic and antisense promoters or leaderless mRNAs. Predictive comparisons using 40 other Epsilonproteobacterial genomes suggests that this lack of conservation of transcriptional features is common to all Epsilonproteobacterial genomes, and is associated with the absence of genome synteny in this subdivision of the Proteobacteria. -

Polarity and Secretion of Shigella Flexneri Icsa: a Classical Autotransporter
Polarity and Secretion of Shigella flexneri IcsA: A Classical Autotransporter MATTHEW THOMAS DOYLE, B. SC. (BIOTECHNOLOGY) Submitted for the degree of Doctor of Philosophy Department of Molecular and Cellular Biology School of Biological Sciences The University of Adelaide Adelaide, South Australia, Australia July 2015 Declaration I certify that this Thesis contains no material which has been accepted for the award of any other degree or diploma in my name, in any university or other tertiary institution and, to the best of my knowledge and belief, contains no material previously published or written by another person, except where due reference has been made in the text. I certify that no part of this work will, in the future, be used in a submission in my name for any other degree or diploma in any university or other tertiary institution without the prior approval of the University of Adelaide and where applicable, any partner institution responsible for the joint- award of this degree. I give consent to this copy of my thesis when deposited in the University Library, being made available for loan and photocopying, subject to the provisions of the Copyright Act 1968. I acknowledge that copyright of published works contained within this thesis resides with the copyright holders of those works. I give permission for the digital version of my thesis to be made available on the web, via the University’s digital research repository, the Library Search and also through web search engines, unless permission has been granted by the University to restrict access for a period of time. -
Identification of Shigella Species
UK Standards for Microbiology Investigations 2013 Identification of Shigella species DECEMBER 13 - NOVEMBER 15 BETWEEN ON CONSULTED WAS DOCUMENT THIS - DRAFT Issued by the Standards Unit, Microbiology Services, PHE Bacteriology – Identification | ID 20 | Issue no: di+ | Issue date: dd.mm.yy <tab+enter> | Page: 1 of 20 © Crown copyright 2013 Identification of Shigella species Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website http://www.hpa.org.uk/SMI/Partnerships. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see http://www.hpa.org.uk/SMI/WorkingGroups). The contributions of many individuals in clinical, specialist and reference laboratories2013 who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editing the medical content. For further information please contact us at: DECEMBER 13 Standards Unit - Microbiology Services Public Health England 61 Colindale Avenue London NW9 5EQ NOVEMBER E-mail: [email protected] 15 Website: http://www.hpa.org.uk/SMI UK Standards for Microbiology Investigations are produced in association with: BETWEEN ON CONSULTED WAS DOCUMENT THIS - DRAFT Bacteriology – Identification | ID 20 | Issue no: di+ | Issue date: dd.mm.yy <tab+enter> | Page: 2 of 20 UK Standards for Microbiology Investigations | Issued by the Standards Unit, Public Health England Identification of Shigella species Contents ACKNOWLEDGMENTS .......................................................................................................... 2 AMENDMENT TABLE ............................................................................................................ -

Product Sheet Info
Product Information Sheet for NR-517 Shigella flexneri, Strain 24570 Citation: Acknowledgment for publications should read “The following reagent was obtained through the NIH Biodefense and Catalog No. NR-517 Emerging Infections Research Resources Repository, NIAID, ® (Derived from ATCC 29903™) NIH: Shigella flexneri, Strain 24570, NR-517.” For research only. Not for human use. Biosafety Level: 2 Appropriate safety procedures should always be used with this material. Laboratory safety is discussed in the following Contributor: publication: U.S. Department of Health and Human Services, ATCC® Public Health Service, Centers for Disease Control and Prevention, and National Institutes of Health. Biosafety in Product Description: Microbiological and Biomedical Laboratories. 5th ed. Bacteria Classification: Enterobacteriaceae, Shigella Washington, DC: U.S. Government Printing Office, 2007; see Species: Shigella flexneri (S. flexneri) www.cdc.gov/od/ohs/biosfty/bmbl5/bmbl5toc.htm. Type Strain: 24570 Serotype: 2a Disclaimers: You are authorized to use this product for research use only. Shigellae are Gram-negative, nonsporulating, facultative, It is not intended for human use. anaerobic bacilli that are the causative agent of shigellosis. Four species of Shigella (S. dysenteriae, S. flexneri, S. Use of this product is subject to the terms and conditions of sonnei and S. boydii) are able to cause the disease. the BEI Resources Material Transfer Agreement (MTA). The Shigellosis is most commonly associated with children of MTA is available on our Web site at www.beiresources.org. developing countries where it causes more than one million deaths every year. Transmission generally occurs through While BEI Resources uses reasonable efforts to include contaminated food and water or by person-to-person 1,2 accurate and up-to-date information on this product sheet, contact. -

Newly Emerged Serotype 1C of Shigella Flexneri
G C A T T A C G G C A T genes Article Newly Emerged Serotype 1c of Shigella flexneri: Multiple Origins and Changing Drug Resistance Landscape Pawan Parajuli 1, Bui Quang Minh 2 and Naresh K. Verma 1,* 1 Division of Biomedical Science and Biochemistry, Research School of Biology, The Australian National University, Canberra, ACT 2601, Australia; [email protected] 2 Research School of Computer Science & Research School of Biology, The Australian National University, Canberra, ACT 2601, Australia; [email protected] * Correspondence: [email protected] Received: 28 July 2020; Accepted: 1 September 2020; Published: 3 September 2020 Abstract: Bacillary dysentery caused by Shigella flexneri is a major cause of under-five mortality in developing countries, where a novel S. flexneri serotype 1c has become very common since the 1980s. However, the origin and diversification of serotype 1c remain poorly understood. To understand the evolution of serotype 1c and their antimicrobial resistance, we sequenced and analyzed the whole-genome of 85 clinical isolates from the United Kingdom, Egypt, Bangladesh, Vietnam, and Japan belonging to serotype 1c and related serotypes of 1a, 1b and Y/Yv. We identified up to three distinct O-antigen modifying genes in S. flexneri 1c strains, which were acquired from three different bacteriophages. Our analysis shows that S. flexneri 1c strains have originated from serotype 1a and serotype 1b strains after the acquisition of bacteriophage-encoding gtrIc operon. The maximum-likelihood phylogenetic analysis using core genes suggests two distinct S. flexneri 1c lineages, one specific to Bangladesh, which originated from ancestral serotype 1a strains and the other from the United Kingdom, Egypt, and Vietnam originated from ancestral serotype 1b strains. -

Biomolecules
biomolecules Review Phylogenetic Distribution, Ultrastructure, and Function of Bacterial Flagellar Sheaths Joshua Chu 1, Jun Liu 2 and Timothy R. Hoover 3,* 1 Department of Microbiology, Cornell University, Ithaca, NY 14853, USA; [email protected] 2 Microbial Sciences Institute, Department of Microbial Pathogenesis, Yale University, West Haven, CT 06516, USA; [email protected] 3 Department of Microbiology, University of Georgia, Athens, GA 30602, USA * Correspondence: [email protected]; Tel.: +1-706-542-2675 Received: 30 January 2020; Accepted: 26 February 2020; Published: 27 February 2020 Abstract: A number of Gram-negative bacteria have a membrane surrounding their flagella, referred to as the flagellar sheath, which is continuous with the outer membrane. The flagellar sheath was initially described in Vibrio metschnikovii in the early 1950s as an extension of the outer cell wall layer that completely surrounded the flagellar filament. Subsequent studies identified other bacteria that possess flagellar sheaths, most of which are restricted to a few genera of the phylum Proteobacteria. Biochemical analysis of the flagellar sheaths from a few bacterial species revealed the presence of lipopolysaccharide, phospholipids, and outer membrane proteins in the sheath. Some proteins localize preferentially to the flagellar sheath, indicating mechanisms exist for protein partitioning to the sheath. Recent cryo-electron tomography studies have yielded high resolution images of the flagellar sheath and other structures closely associated with the sheath, which has generated insights and new hypotheses for how the flagellar sheath is synthesized. Various functions have been proposed for the flagellar sheath, including preventing disassociation of the flagellin subunits in the presence of gastric acid, avoiding activation of the host innate immune response by flagellin, activating the host immune response, adherence to host cells, and protecting the bacterium from bacteriophages. -

The Role of Cellular Autophagy and Type Iv Secretion System in Anaplasma Phagocytophilum Infection
THE ROLE OF CELLULAR AUTOPHAGY AND TYPE IV SECRETION SYSTEM IN ANAPLASMA PHAGOCYTOPHILUM INFECTION DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Hua Niu, M.S. * * * * * The Ohio State University 2008 Dissertation Committee: Dr. Yasuko Rikihisa, Adviser Approved by Dr. William P. Lafuse Dr. Mamoru Yamaguchi __________________________ Dr. Michael J. Oglesbee Adviser Graduate Program in Veterinary Biosciences ABSTRACT Human granulocytic anaplasmosis (HGA), an emerging tick-borne zoonosis is caused by a gram-negative, obligatory intracellular bacterium, Anaplasma phagocytophilum. A. phagocytophilum has the remarkable ability to inhibit the spontaneous apoptosis of neutrophils, block the production of reactive oxygen intermediates, and replicate in membrane-bound inclusions in the cytoplasm of neutrophils. However, the A. phagocytophilum inclusions have not been fully characterized, and bacterial factors contributing to these phenomena remain unknown. In this study, we studied several molecular aspects of A. phagocytophilum pathogenesis. (1) Characterization of A. phagocytophilum replicative inclusions. We demonstrated that A. phagocytophilum replicative inclusions had the characteristic of early autophagosomes, as shown by the presence of autophagosome markers, LC3 and double lipid bilayer membrane in the A. phagocytophilum inclusions. Furthermore our data suggested that autophagy enhanced A. phagocytophilum replication instead of inhibiting its growth. (2) Investigation of the expression of genes encoding type IV secretion system apparatus in A. phagocytophilum. We found the expression of virB6 and virB9 was up- regulated during the bacterial growth in human neutrophils. Furthermore, differential ii VirB9 expression was shown to associate with the binding of A. phagocytophilum to neutrophils, and prevention of internalized bacteria from being delivered to lysosomes. -

Shigella Spp. Potential Food Safety Hazard Control Measures FDA
Shigella spp. Updated: Potential Food Safety Hazard Control Measures FDA Guidelines Growth Analytical Procedures o Food Sampling and Preparation of Sample Homogenate o Definition of Terms; Collection of Samples; Supplement to all Methods in the HC Compendium (HC) o Shigella o Determination of Enterobacteriaceae (HC) References Potential Food Safety Hazard Top Shigellosis, although commonly regarded as waterborne, is also a food-borne disease restricted primarily to higher primates, including humans. It is usually spread among humans by food handlers with poor personal hygiene. Foods most often incriminated in the transmission have been potato salad, shellfish, raw vegetables, and Mexican dishes. The genus Shigella consists of four species: S. dysenteriae (subgroup A), S. flexneri (subgroup B), S. boydii (subgroup C), and S. sonnei (subgroup D). Shigella organisms may be very difficult to distinguish biochemically from Escherichia coli. Brenner (1984) considers Shigella organisms and E. coli to be a single species, based on DNA homology. Nonetheless, Shigella species are Gram-negative, facultatively anaerobic, nonsporulating, nonmotile rods in the family Enterobacteriaceae. They do not decarboxylate lysine or ferment lactose within 2 d. They utilize glucose and other carbohydrates, producing acid but not gas. However, because of their affinity with E. coli, frequent exceptions may be encountered, e.g., some biotypes produce gas from glucose and mannitol. Neither citrate nor malonate is used as the sole carbon source for growth, and the organisms are inhibited by potassium cyanide (Andrews, 1998). Control Measures Top Hazards from Shigella can be prevented by preventing human waste contamination of water supplies and by improved personal hygiene for people who are ill or are carriers of Shigella and work in food operations (Ward et al., 1997). -

Identification of Intestinal Microbes in Children With
IDENTIFICATION OF INTESTINAL MICROBES IN CHILDREN WITH DIARRHEA ANDNON-DIARRHEA USING POLYMERASE CHAIN REACTION / ELECTROSPRAY IONIZATION-MASS SPECTROMETRY (PCR / ESI-MS) Teguh Sarry Hartono1, Dewi Murniati2, Andi Yasmon3, Lucky H Moehario3 1 Infectious Disease HospitalProf Dr Sulianti Saroso, Microbiology Resident–Departement of Microbiology, Faculty of Medicine, University of Indonesia. 2Infectious Disease Hospital Prof Dr Sulianti Saroso, 3Department of Microbiology, Faculty of Medicine, University of Indonesia. Abstract :Microbiota present in human intestinal are diverse, and imbalance in composition of intestinal flora may cause diarrhea.This study aimed to obtain a profile of intestinal bacteria in children with and without diarrhea and assess their presence with incidence of diarrhea. An analitical descriptive with cross sectional design study was carried out. A stool specimen was collected from each children of 2-12 years old with and without diarrhea who lived in North Jakarta. DNA extraction was performed prior to detection of microbes using Polymerase Chain Ceaction/Electrospray Ionization-Mass Spectrometry. Eighty stool specimens consisted of 33 and 47 specimens from children with and without diarrhea were included in the study. Thirty single and 6 multiple matches were detected in 30 specimens of the diarrhea group; 28 single and 8 multiple matches were found in 34 specimens of the non-diarrhea.Escherechiacoli and Klebsiella pneumonia were predominant in both groups. Firmicutes, Proteobacteria and Bacteroidetes were deteced in the diarrhea group, while Actinobacteria, Proteobacteria and Verrucomicrobia were in the non-diarrhea. The relationship of incidence of diarrhea and the present of enteropathogens in the stool was not significant, however, there was a strong correlation of the risk of suffering diarrhea due to the presence of enteropathogens (OR = 0.724 with 95%, CI: 0.237-2.215).