Fatal Accident at Tyseley Depot 14 December 2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tracks the Monthly Magazine of the Inter City Railway Society
Tracks the monthly magazine of the Inter City Railway Society Volume 40 No.7 July 2012 Inter City Railway Society founded 1973 www.icrs.org.uk The content of the magazine is the copyright of the Society No part of this magazine may be reproduced without prior permission of the copyright holder President: Simon Mutten (01603 715701) Coppercoin, 12 Blofield Corner Rd, Blofield, Norwich, Norfolk NR13 4RT Chairman: Carl Watson - [email protected] (07403 040533) 14, Partridge Gardens, Waterlooville, Hampshire PO8 9XG Treasurer: Peter Britcliffe - [email protected] (01429 234180) 9 Voltigeur Drive, Hart, Hartlepool TS27 3BS Membership Secretary: Trevor Roots - [email protected] (01466 760724) (07765 337700) Mill of Botary, Cairnie, Huntly, Aberdeenshire AB54 4UD Secretary: Stuart Moore - [email protected] (01603 714735) 64 Blofield Corner Rd, Blofield, Norwich, Norfolk NR13 4SA Magazine: Editorial Manager: Trevor Roots - [email protected] details as above Editorial Team: Sightings: James Holloway - [email protected] (0121 744 2351) 246 Longmore Road, Shirley, Solihull B90 3ES Traffic News: John Barton - [email protected] (0121 770 2205) 46, Arbor Way, Chelmsley Wood, Birmingham B37 7LD Website: Website Manager: Mark Richards - [email protected] 7 Parkside, Furzton, Milton Keynes, Bucks. MK4 1BX Yahoo Administrator: Steve Revill Books: Publications Manager: Carl Watson - [email protected] details as above Publications Team: Combine & Individual / Irish: Carl Watson - [email protected] Pocket Book: Carl Watson / Trevor Roots - [email protected] Wagons: Scott Yeates - [email protected] Name Directory: Eddie Rathmill / Trevor Roots - [email protected] USF: Scott Yeates / Carl Watson / Trevor Roots - [email protected] Contents: Officials Contact List .....................................2 Traffic and Traction News................ -

Vintage Trains Business Plan November 2017
Vintage Trains Business Plan November 2017 Disclaimer and Explanatory Note This business plan has been prepared from information provided by the Trustees and Managers of Vintage Trains Charitable Trust to assist potential community subscribers to consider buying community shares in Vintage Trains CBS, a Community Benefit Society. This document is not a prospectus nor investment advertisement, financial promotion or offer under the Financial Services and Markets, Act 2000. Consequently, neither the Trustees, Managers nor the advisers can accept responsibility for any losses arising to persons acting or refraining from action on the material contained in this business plan. Persons considering a financial commitment of any kind should conduct such investigations as they consider necessary to satisfy themselves as to the appropriateness of the financial commitment and the risk of loss or some or all of any financial commitment. Page 2 of 36 Contents 1. Introduction and background ............................................................................................................ 4 1.1 Purpose of the business plan ....................................................................................................... 4 1.2 About Vintage Trains ................................................................................................................... 4 2. The need for the share offer .............................................................................................................. 6 2.1 Purpose of the share offer -

Warding Arrangements for Legend Ladywood Ward
Newtown Warding Arrangements for Soho & Jewellery Quarter Ladywood Ward Legend Nechells Authority boundary Final recommendation North Edgbaston Ladywood Bordesley & Highgate Edgbaston 0 0.1 0.2 0.4 Balsall Heath West Kilometers Contains OS data © Crown copyright and database right 2016. $ Bournville & Cotteridge Allens Cross Warding Arrangements for Longbridge & West Heath Ward Legend Frankley Great Park Northfield Authority boundary King's Norton North Final recommendation Longbridge & West Heath King's Norton South Rubery & Rednal 0 0.15 0.3 0.6 Kilometers Contains OS data © Crown copyright and database right 2016. $ Warding Arrangements for Lozells Ward Birchfield Legend Authority boundary Final recommendation Aston Handsworth Lozells Soho & Jewellery Quarter Newtown 0 0.05 0.1 0.2 Kilometers Contains OS data © Crown copyright and database right 2016. $ Small Heath Sparkbrook & Balsall Heath East Tyseley & Hay Mills Warding Balsall Heath West Arrangements for Moseley Ward Edgbaston Legend Authority boundary Final recommendation Sparkhill Moseley Bournbrook & Selly Park Hall Green North Brandwood & King's Heath Stirchley Billesley 0 0.15 0.3 0.6 Kilometers Hall Green South Contains OS data © Crown copyright and database right 2016. $ Perry Barr Stockland Green Warding Pype Hayes Arrangements for Gravelly Hill Nechells Ward Aston Legend Authority boundary Final recommendation Bromford & Hodge Hill Lozells Ward End Nechells Newtown Alum Rock Glebe Farm & Tile Cross Soho & Jewellery Quarter Ladywood Heartlands Bordesley & Highgate 0 0.15 0.3 0.6 Kilometers Bordesley Green Contains OS data © Crown copyright and database right 2016. $ Small Heath Handsworth Aston Warding Lozells Arrangements for Newtown Ward Legend Authority boundary Final recommendation Newtown Nechells Soho & Jewellery Quarter 0 0.075 0.15 0.3 Ladywood Kilometers Contains OS data © Crown copyright and database Ladywood right 2016. -

HRA-News-160-April-2020.Pdf
April 2020 The official journal of THE HERITAGE RAILWAY ASSOCIATION Issue 160 UNTIL FURTHER NOTICE Three general managers talk about coping with lockdown New faces at the HRA! COVID-19 Advice and guidance Coal OFFERS 2020 Awards & winners update WANTS Chairman’s Briefing Dates for your Diary Dear Member, November 2020 Right now, you’re trying to see the future for your railway, or your museum, your tramway, your cliff railway. When can you reopen? 10th Autumn Seminar How will finances look? How long will it take things to get back to 11th Autumn Management Forum normal? You’re not alone. Thank goodness for the friendship and solidarity of the heritage railways movement. We’ve always been good at collaboration Inside this edition and sharing, from locomotives and rolling stock, through staff and equipment, to knowledge and ideas. I’m proud to say that the Chairman’s Briefing 2 Chief Exec’s Briefing 3 HRA has contributed to that solidarity and sharing. Today, we’re Covid -19 4 working even harder at our role of supporting all our members, Covid -19 HRA support 6 and helping you all to speak with one voice for the aid and Coal - latest news 10 consideration we’ll be needing over the weeks and months to Coal - key facts 13 come. New Faces at the HRA 14 Members News 15 We can’t help looking ahead. Many of you will be planning for a Friends Tour 16 long, dry season. And that’s wise work. But there’s also plenty of In Memoriam 17 important work to do today. -

Boiler Almost Finished
BOILER ALMOST FINISHED The new smokebox in position on the smokebox saddle on Betton Grange at Tyseley on September 29th. BARRY HAYMAN uilding steam locomotives in the 21st predict when the work will be completed. century is a precarious and expensive A year ago, the best guess was that we business, let no-one persuade you would have the boiler back from Tyseley in Botherwise! late spring of this year, then a number of Just as it is impossible to predict exactly months would be required to put everything how much it costs to build a main line together and perhaps get a fire in the grate tender locomotive, so it is impossible to by November or December. That was until it Autumn Newsletter 2018 WELCOME... was discovered we needed a new front taper the spring, there will be comparatively little section for the boiler and immediately this outstanding work before the locomotive can put us back three months. be steamed. In the event, instead of Tyseley sending However, and this is a big HOWEVER, we the completed boiler to Llangollen, we still have a funding shortage. Our Final Push decided to take the chassis to Tyseley, at fundraising initiative, launched almost a year the end of June, so that once the boiler was ago, is still open. As estimates for the cost of finished it could be trial fitted into the frames outstanding work have changed, the overall so that any snags could be sorted out at cost has gone up and we are still searching Tyseley. The smokebox was placed onto the for around £40k to finish the loco. -

Railway Enthusiasts 2018
RAILWAY ENTHUSIASTS 2018 February 2018: A RAILWAY LIFE Andrew gave us a talk about his sometimes-colourful career on the railway, mainly spent at Toton. Starting in November 1970, Andrew was looking for the legendary “Job for Life”, something that was still available back in those days, so applied for a clerical job with British Rail. This was as an ATI (Advanced Traffic Information) clerk, a new system that was being tried out to make sure that traffic could be individually identified. This was a little hit and miss, due to the vagaries of what passed for technology then. Training in touch-typing was seen as a necessity, so off he went with 3 other colleagues to Euston. Mistaken identity nearly got him into trouble but resulted in fortunately gaining a more advantageous post. With yet another system being brought into play, Andrew made a move to Gloucester to steal a march on this new process. A couple of fun years, watching nuclear flasks being derailed, mysterious contents eating a wagon and flying wagons burying themselves in the ground followed, before he was propelled back to Toton. The decline in traffic ended up with the demise of Hump Shunting before a couple of moves found him in Nottingham, on the site where Dunelm now sits. After some fortuitous moves and promotions, Andrew found himself, as privatisation took the freight railway into American hands, in an extremely busy and exacting role. He was trying to win freight back to rail from road, an uphill battle at the best of times. As Development Manager (Central) Andrew was responsible for projects in the South-East, East Anglia and the East Midlands, before changes that for a brief time had him covering projects across most of the country! Things steadied down, very slightly as new territorial lines were drawn and eventually “Central” came to mean the East Midlands, West Midlands, all of Wales and the South West from Southampton westwards. -

Springfield Medical Rajput 25 1 19
OUR PRACTICE AREA SERVICES AVALIABLE Moseley, Tyseley, Sparkhill, Springfield, Anticoagulation clinic Hall Green, Acocks Green, Shirley, Solihull and SPRINGFIELD Baby Clinic (8 week check) Olton and other areas at the discretion of Dr. ECG Recording and Interpretation LOCAL My Healthcare Federation HUB is generally Immunisations MEDICAL open 8am-8pm 7 days a week. Appointments can be Quit Smoking Clinic booked via the surgery for consultations. Phlebotomy (blood taking) The nearest HUB is at Travel Advice & Vaccinations Fernley Medical Centre HUB, 560 Stratford Road, Joint Injections PRACTICE Sparkhill, Birmingham B11 4AN Minor Operations HUB Services include: face to face GP appointments, Virtual GP, Virtual Cryotherapy (Freezing Treatment) Pharmacist, District Nurses, HCA Appointments & Physiotherapy . Sexual Health including Coil fitting 739- 741 STRATFORD ROAD Unlike your GP at the practice however, doctors at the local Spirometry SPRINGFIELD, BIRMINGHAM B11 4DG HUB do not have the benefit of seeing you on a regular Long term conditions clinics/management - basis despite having access to your medical records. You CONTACT NUMBER are more likely to be assured of continuity of care, effective Diabetes, Asthma/COPD, Heart treatment of on-going or long term conditions, and Disease, Epilepsy, Hypertension, Thyroid, personal doctoring at your own GP surgery. Depression, Cancer, Dementia, Mental 0121 778 4321 It is wise therefore to always contact your GP surgery, at all Health Conditions, Medically Unexplained FAX : 0121 702 2662 times, with your health needs before going to local HUB or Symptoms etc. A&E. Doctors at the surgery will be able to advise you if you do need to attend the A&E department. -

NRT Index Stations
Network Rail Timetable OFFICIAL# May 2021 Station Index Station Table(s) A Abbey Wood T052, T200, T201 Aber T130 Abercynon T130 Aberdare T130 Aberdeen T026, T051, T065, T229, T240 Aberdour T242 Aberdovey T076 Abererch T076 Abergavenny T131 Abergele & Pensarn T081 Aberystwyth T076 Accrington T041, T097 Achanalt T239 Achnasheen T239 Achnashellach T239 Acklington T048 Acle T015 Acocks Green T071 Acton Bridge T091 Acton Central T059 Acton Main Line T117 Adderley Park T068 Addiewell T224 Addlestone T149 Adisham T212 Adlington (cheshire) T084 Adlington (lancashire) T082 Adwick T029, T031 Aigburth T103 Ainsdale T103 Aintree T105 Airbles T225 Airdrie T226 Albany Park T200 Albrighton T074 Alderley Edge T082, T084 Aldermaston T116 Aldershot T149, T155 Aldrington T188 Alexandra Palace T024 Alexandra Parade T226 Alexandria T226 Alfreton T034, T049, T053 Allens West T044 Alloa T230 Alness T239 Alnmouth For Alnwick T026, T048, T051 Alresford (essex) T011 Alsager T050, T067 Althorne T006 Page 1 of 53 Network Rail Timetable OFFICIAL# May 2021 Station Index Station Table(s) Althorpe T029 A Altnabreac T239 Alton T155 Altrincham T088 Alvechurch T069 Ambergate T056 Amberley T186 Amersham T114 Ammanford T129 Ancaster T019 Anderston T225, T226 Andover T160 Anerley T177, T178 Angmering T186, T188 Annan T216 Anniesland T226, T232 Ansdell & Fairhaven T097 Apperley Bridge T036, T037 Appleby T042 Appledore (kent) T192 Appleford T116 Appley Bridge T082 Apsley T066 Arbroath T026, T051, T229 Ardgay T239 Ardlui T227 Ardrossan Harbour T221 Ardrossan South Beach T221 -

Delivering a Rail Revolution for Communities
Delivering a Rail Revolution for Communities Malcolm Holmes, Executive Director West Midlands Rail Executive is a movement for change, driving a revolution in rail services for West Midlanders • Increasing local influence over our rail network through: • A strong role in the specification and procurement of the 2017 West Midlands franchise • Leading the local management of the franchise • A role in specification of other franchises that operate in the region • A fully devolved West Midlands rail franchise WMRE Strategic Focus Single Network Vision West Midlands Rail Investment Strategy West Midlands West Midlands Rail Franchising Rail Programme Stations Alliance & Partnerships WMRE Strategic Focus Single Network Vision West Midlands Rail Investment Strategy West Midlands West Midlands Rail Franchising Rail Programme Stations Alliance & Partnerships Franchises in WMRE Area Crewe Stoke-on-Trent West Midlands Franchise - WMSBU West Midlands Franchise - WCSBU Derby Cross Country Nottingham Stafford Chiltern Railways Rugeley Trent Valley Wales & Borders (Arriva Trains Wales) Burton-on- Rugeley Town Trent Inter City West Coast (Virgin Trains) Cannock Lichfield Trent Lichfield City Valley Great Western (First Great Western) East Midlands Walsall Tamworth Shrewsbury Sutton Coldfield Tame Bridge Pky Wolverhampton Nuneaton Birmingham Aston Snow Hill Hinckley Leicester Telford Telford Central Smethwick Galton Bridge New St Rowley Regis Birmingham International Cradley Heath Birmingham Moor St University Coventry Rugby Stourbridge Solihull Long Buckby -
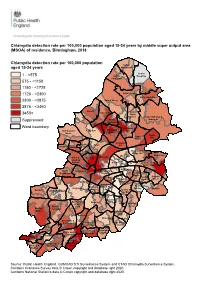
MSOA) of Residence, Birmingham, 2018
Chlamydia detection rate per 100,000 population aged 15-24 years by middle super output area (MSOA) of residence, Birmingham, 2018 Chlamydia detection rate per 100,000 population Sutton aged 15-24 years Mere Green Sutton 1 - <575 Sutton Roughley Four Oaks 575 - <1150 1150 - <1725 1725 - <2300 Sutton Trinity Sutton Reddicap 2300 - <2875 Sutton Vesey 2875 - <3450 Oscott Kingstanding Sutton 3450+ Wylde Green Sutton Walmley & Perry Minworth Suppressed Common Ward boundary Erdington Handsworth Perry Barr Stockland Wood Green Castle Pype Vale Hayes Gravelly Birchfield Aston Hill Holyhead Handsworth Lozells Bromford & Hodge Hill Ward End Shard End Soho & Newtown Nechells Jewellery Quarter Alum Rock Glebe Farm & Tile Cross Heartlands North Ladywood Bordesley & Edgbaston Highgate Yardley East Garretts Bordesley Yardley Green Green Small West & Heath Stechford Sparkbrook & South Balsall Balsall Heath Edgbaston Yardley Sheldon Heath East Tyseley & Quinton Harborne West Hay Mills Sparkhill Bournbrook Moseley & Selly Acocks Weoley & Park Green Bartley Selly Oak Green Hall Green North Stirchley Billesley Bournville & Cotteridge Brandwood & Hall Green King's Heath South Allens Cross Druids Heath Highter's King's Norton & Monyhull Heath North Frankley Northfield Great Park King's Longbridge & Norton Rubery & West Heath South Rednal Source: Public Health England, GUMCAD STI Surveillance System and CTAD Chlamydia Surveillance System. Contains Ordnance Survey data © Crown copyright and database right 2020. Contains National Statistics data © Crown copyright -
A Public Consultation on Revised Proposals for the Transposition of Directive 2008/57/EC on the Interoperability of the Rail System
A public consultation on revised proposals for the transposition of Directive 2008/57/EC on the interoperability of the rail system 1 October 2011 Contents Executive Summary 2 How to respond 2 Freedom of Information 3 The Consultation Criteria 4 What will happen next 4 The proposals 5 Longer term strategic issues 22 List of consultation questions 25 Annexes: A – List of those consulted B - The Consultation Criteria C – Draft Railways (Interoperability) Regulations 2012 D - Transposition Note E – Draft List of Exclusions from Scope (GB) F – Draft Impact Assessment G – Directive 2008/57 (and updates) H – Commission Recommendation 2011/217 2 October 2011 Executive Summary i.) This consultation seeks views on draft regulations concerning the interoperability of the railways. These regulations are necessary to meet the requirements of the Interoperability Directive 2008/57/EC which recast earlier versions and the deadline for implementation was 19 July 2010. The recast Directive contained new provisions for type authorisation of vehicles. It also has provisions for the reauthorisation process for vehicles authorised in another Member State which have been moved from the 2004 Safety Directive into the Interoperability Directive. ii.) The draft regulations will implement the Directive for England, Scotland, Wales and Northern Ireland. The reauthorisation of vehicles for the UK half of the Channel Tunnel are dealt with in bi-national safety regulations. All other requirements in the Directive in relation to the Tunnel will be implemented through these draft interoperability regulations. iii.) This consultation builds on two earlier rounds of consultation which were published by the Department in 2009 and 2010. -
Tyseley Energy Park and the Creation of the Smart Manufacturing Approach ‘Factory in a Box’ (See Annex 2)
ERA Phase 1 – Summary of Outputs 1 Energy Research Accelerator (ERA) Phase 1 – Summary of Outputs ERA Phase 1 – Summary of Outputs 2 Energy Research Accelerator (ERA) Phase 1 – Summary of Outputs Established in 2016 as the UK’s first cross-disciplinary energy research acceleration hub, the pioneering Energy Research Accelerator (ERA) brings together 1400 researchers in eight internationally-recognised research universities from the Midlands region (Aston, Birmingham, Cranfield, Keele, Leicester, Loughborough, Nottingham and Warwick) and the British Geological Survey. It was funded as a large-scale pilot to establish whether wide scale collaborative working could deliver significant regional impact. The five-year programme was created in discussion with BEIS and was financially supported by Innovate UK. The core objectives were to integrate research, develop advanced energy systems, reduce dependence on importing energy, enhance energy security and resilience, deliver regional economic benefit, develop future energy leaders and help to achieve the region and UK’s carbon reduction targets. After only four years, already there has been significant success and economic impact, the latter amounting to a 9:1 return on the original £60m government investment. Benchmarking suggests the level of funding catalysed would result, over a longer term, in a net GVA of £3bn and 10,000 new jobs. Whilst not all of this activity has been led by ERA, ERA funding has been a key contributor in unlocking opportunities. The Midlands is a region which has historically underperformed in terms of employment, skilled jobs and has been significantly impacted by Covid-19, and hence ERA aligns strongly to the levelling-up agenda.