E960 Public Disclosure Authorized
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Academic Calendar 19-20
Academic Calendar 2019-20 TBAK COLLEGE FOR WOMEN THASSIM BEEVI ABDUL KADER COLLEGE FOR WOMEN Kilakarai - 623 517, Ramanathapuram District Sponsored by Seethakathi Trust, Chennai - 600 006 [A Minority Autonomous Institution & Re-accredited by NAAC with B++ Grade ISO 9001:2015 Certified Institution] Affiliated to Alagappa University, Karaikudi 2 0 1 9 - 2 0 1 TBAK COLLEGE FOR WOMEN Academic Calendar 2019-20 In the name of the Almighty, The Most Gracious, The Most Merciful! All praise be to the Almighty only! Towards the end of the meeting recite this together with the audience Glory be to the Almighty and praise be to Him! Glory be to YOU and all praise be to You! I bear witness that there is no true GOD except YOU alone. I ask your pardon and turn to YOU in repentance. [Dua from the Hadith of Prophet Muhammad (PBUH) Narrated by Abu Hurairah (Rali) Source: Abu Dawud: 4859] 2 Academic Calendar 2019-20 TBAK COLLEGE FOR WOMEN In the Name of Allah, the Most Gracious, the Most Merciful Proclaim (Or Read :) In the name of thy Lord and Cherisher, Who Created man, out of a mere clot of congealed blood. Proclaim! And thy Lord is Most Bountiful He who taught the use of the pen Taught man that which he knew not Nay, but man doth transgress all bounds In that he looketh upon himself as self-sufficient. Verily, to thy Lord is the return of all. Alquran Sura 96: (verses 1 to 8) 3 TBAK COLLEGE FOR WOMEN Academic Calendar 2019-20 Founded in 1988 G O No 1448 dated 12 September 1988 THASSIM BEEVI ABDUL KADER COLLEGE FOR WOMEN (Sponsored by Seethakathi Trust, Chennai) (Affiliated to Alagappa University, Karaikudi) No. -
CTRI Trial Data
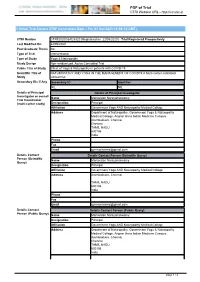
PDF of Trial CTRI Website URL - http://ctri.nic.in Clinical Trial Details (PDF Generation Date :- Fri, 01 Oct 2021 15:08:12 GMT) CTRI Number CTRI/2020/05/025320 [Registered on: 22/05/2020] - Trial Registered Prospectively Last Modified On 22/05/2020 Post Graduate Thesis No Type of Trial Interventional Type of Study Yoga & Naturopathy Study Design Non-randomized, Active Controlled Trial Public Title of Study Effect of Yoga & Naturopathy in patients with COVID-19 Scientific Title of NATUROPATHY AND YOGA IN THE MANAGEMENT OF COVID19 A Multi-center controlled Study clinical trial Secondary IDs if Any Secondary ID Identifier NIL NIL Details of Principal Details of Principal Investigator Investigator or overall Name Manavalan Narayanaswamy Trial Coordinator (multi-center study) Designation Principal Affiliation Government Yoga AND Naturopathy Medical College Address Department of Naturopathy, Government Yoga & Naturopathy Medical College, Arignar Anna Indian Medicine Campus Arumbakkam, Chennai Chennai TAMIL NADU 600106 India Phone Fax Email [email protected] Details Contact Details Contact Person (Scientific Query) Person (Scientific Name Manavalan Narayanaswamy Query) Designation Principal Affiliation Government Yoga AND Naturopathy Medical College Address Arumbakkam, Chennai TAMIL NADU 600106 India Phone Fax Email [email protected] Details Contact Details Contact Person (Public Query) Person (Public Query) Name Manavalan Narayanaswamy Designation Principal Affiliation Government Yoga AND Naturopathy Medical College Address Department -

ANSWERED ON:11.05.2005 AUTOMATIC and MODERN TELEPHONE EXCHANGES in TAMIL NADU Kharventhan Shri Salarapatty Kuppusamy
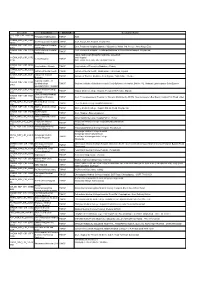
GOVERNMENT OF INDIA COMMUNICATIONS AND INFORMATION TECHNOLOGY LOK SABHA UNSTARRED QUESTION NO:6879 ANSWERED ON:11.05.2005 AUTOMATIC AND MODERN TELEPHONE EXCHANGES IN TAMIL NADU Kharventhan Shri Salarapatty Kuppusamy Will the Minister of COMMUNICATIONS AND INFORMATION TECHNOLOGY be pleased to state: (a) the details of automatic and modern telephone exchanges set up in Tamil Nadu during the last three years, location- wise; (b) the details of such exchanges proposed to be set up in Tamil Nadu during the current year; (c) the details of the telephone exchanges whose capacities were expanded in the current financial year; and (d) the details of telephone exchanges where waiting list for telephone connection still exists? Answer THE MINISTER OF STATE IN THE MINISTRY OF COMMUNICATIONS ANDINFORMATION TECHNOLOGY (DR. SHAKEEL AHMAD) (a) The details of automatic and modern telephone exchanges set up in Tamilnadu during the last three years are given in the Annexures- I(a), I(b) & I(c). (b) The details of such exchanges proposed to be set up in Tamilnadu during the current year are given in Annexure-II. (c) The details of the telephone exchanges whose capacities were expanded in the current financial year are given at Annexure-III. (d) The details of telephone exchanges where waiting list for telephone connection still exists are given in Annexure- IV. ANNEXURE-I(a) DETAILS OF TELEPHONE EXCHANGES SET UP DURING 2002-03 IN TAMILNADU Sl Name of Exchange Capacity Type/Technology District No.(Location) 1 Avinashi-II 4000 CDOTMBMXL Coimbatore 2 K.P.Pudur -
Research Methodology and Biostatistics” for Affiliated Institutions of the Tamil Nadu Dr.M.G.R Medical University As Per the Given Schedule
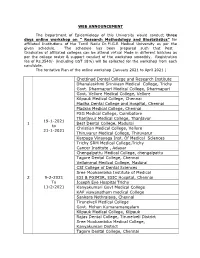
WEB ANNOUNCEMENT The Department of Epidemiology of this University would conduct three days online workshop on “ Research Methodology and Biostatistics” for affiliated Institutions of the Tamil Nadu Dr.M.G.R Medical University as per the given schedule. The schedule has been prepared such that Post Graduates of affiliated colleges can be attend virtual Mode in different batches as per the college roster & support conduct of the workshop smoothly. Registration fee of Rs.3540/- (including GST 18%) will be collected for the workshop from each candidate. The tentative Plan of the online workshop (January 2021 to April 2021 ) Chettinad Dental College and Research Institute Dhanalaskhmi Srinivasn Medical College, Trichy Govt. Dharmapuri Medical College, Dharmapuri Govt. Vellore Medical College, Vellore Kilpauk Medical College, Chennai Madha Dental College and Hospital, Chennai Madras Medical College, Chennai PSG Medical College, Coimbatore Thanjavur Medical College, Thanjavur 19-1-2021 1 Best Dental College, Madurai to Christian Medical College, Vellore 21-1-2021 Thiruvarur Medical College, Thiruvarur Karpaga Vinayaga Inst. Of Medical Sciences Trichy SRM Medical College,Trichy Cancer Institute , Adayar Chengalpattu Medical College, chengalpattu Tagore Dental College, Chennai Vellammal Medical College, Madurai CSI College of Dental Sciences Sree Mookambika Institute of Medical 29-2-2021 ESI & PGIMSR, ESIC Hospital, Chennai To Joseph Eye Hospital Trichy 11-2-2021 Kanyakumari Govt Medical College KAP viswanatham medical College Sankara Nethralaya, Chennai Tirunelveli Medical College Govt. Mohan Kumaramangalam Kilpauk Medical College, Kilpauk Rajas Dental College, Tirunelveli District Sree Mookambika Medical College, Kanyakumari District Tagore Dental College, Chennai Trichy SRM Medical College,Trichy Vivekanandha Dental College for Women, Namakkal Christian medical College, Vellore Govt. -

Community-Supported Management and Conservation Strategies for Seagrass Beds in Palk Bay
1 Community-supported management and conservation strategies for seagrass beds in Palk Bay Clown fish amongst the seagrass of Palk bay © SDMRI Final Project Report December 2014 – January 2016 IUCN, International Union for Conservation of Nature India Country Office Project Details Community-supported management and conservation strategies Project Name for seagrass beds in Palk Bay IUCN, International Union for Conservation of Nature Grantee Name & Address India Country Office C4/25 Safdarjung Development Area, New Delhi, 110016, India Principle Investigator: Ms. Nisha D’Souza, IUCN India Country Office Project Associate: Ms. Jagriti Kumari, IUCN India Country Office Implementing partner: Suganti Devadason Marine Research Institute (SDMRI) Advisors: Dr. NM Ishwar (Programme Coordinator, IUCN India Project team Country Office); Dr. Saudamini Das (Associate Professor, Institute of Economic Growth); Dr. RC Bhatta (Professor of Fisheries Economics, College of Fisheries); Dr. Ruchi Badola (Scientist- G/Senior Professor, Wildlife Institute of India); Dr. E. Vivekananda (Scientist Emeritus, Central Marine Fisheries Research Institute); Dr. JD Sophia (Principal Scientist, M.S. Swaminathan Research Foundation); Dr. Y. Yadava (Director, Bay of Bengal Programme, Inter-Governmental Organization) Project Start Date 12 December 2014 Project End Date 11 January 2016 Reporting Period Final report Submitted to GIZ on: 12 February 2016 Produced with the financial support of GIZ. 2 Contents page Contents Page No. 1. Background to the Project 4 2. Summary of Project Activities 5 3. Literature Review 3.1 Palk Bay Marine Ecosystem 6 3.2 Linkages Between Seagrass and Fisheries 8 3.3 Economic Valuation of Seagrass 9 3.4 Management & Conservation of Palk Bay seagrass 11 3.5 Participatory Management 12 4. -

Madras Village Survey Monographs, 12, Athangarai, Part VI, Vol-IX
CENSUS OF INDIA 1961 VOLUME IX MADRAS PART VI VILLAGE SURVEY MONOGRAPHS 12. ATHANGARAI P. K. NAMBIAR OF THE INDIAN ADMINISTRATIVE SERVICE SUPERINTENDENT OF CENSUS OPERATIONS, MADRAS 1964 CENSUS OF INDIA 1961 (Cen!'us Report-Vol. No. IX will relate to Madras only. Under this series will be issued the following publications) Part I-A General Report (2 Volumes) I-B Demography and Vital Statistics * T-C Subsidiary Tables * Part lI-A General Population Tables * II-B (I) General Economic Tables B-1 to B-IV * IT-B (II) B-V to B-IX * ll-C (I) Cultural Tables * IT-C-IT (i) MIgration Tables IJ-C-U (ii) * Part III Household Economic Tables * Part IV-A Report on Honsing and Establishments * IV-B Housing and Establishment Tables" * Part V-A (i) Scheduled Castes and Tribes (ReporL&-Tabb!s SCT I and SCT II) V-A (ii) " (Tables SCT HI to SCT IX and Special Tables) * V-B (I) Ethnographic Notes on Scheduled Tribes V-R (II) V-C Todas V-D Ethnographic Notes on Scheduled Castes V-E Ethnographic Notes on Denotified and Nomadic Tribes * Part VI Village Survey Monographs (40 Nos.) * Part VII-A Crafts and Artisans (9 Nos.) VII-B Fairs and Festivals * Part VIII-A Administration Report - Enumeration } For Official use only * VIlI-B Administration Report - Tabulation Part IX Atlas of the Madras State Part X Madras City (2 Volumes) District Census Handbooks on twelve districts Part XI Reports on Special Studies * A Handlooms in Madras State "' B Food Habits in Madras State C Slums of Madras City D Temples of Madras State (5 Volumes) * E Physically Handicapped of Madras State F Family Planning Attitudes: A Survey Part Xl[ Languages of Madras State * ALREADY PUBLISHED FOREWORD Apart from laying the foundations of demography in this sub-continent, a hundred years of the Indian Census has also produced "elaborate and scholarly accounts of the variegated phenomena of Indian life-sometimes with no statistics attached, but usually with just enough statistics to give empirical underpinning to their conclusions". -

ALLOTTED LIST (1).Xlsx
PG DEGREE/DIPLOMA COURSES 2020-2021 SESSION RESULT- ROUND II - GOVERNMENT QUOTA SNO GRANK ARNO NAME COMMUNITY SERVICE MARKSFROM TO M.D. D.V.L M.D. D.V.L 1 1 5709 BHUVANANDHINI K BC Service 1035.05 MADRAS MEDICAL COLLEGE, CHENNAI MADRAS MEDICAL COLLEGE, CHENNAI M.D. Radio Diagnosis M.D. Radio Diagnosis 2 2 5272 SHIVA A MBC/DNC Service 1002.3 MADRAS MEDICAL COLLEGE, CHENNAI MADRAS MEDICAL COLLEGE, CHENNAI M.D. Radio Diagnosis M.D. Radio Diagnosis 3 3 4624 B KIRUBAKARAN BC Service 991.2 MADRAS MEDICAL COLLEGE, CHENNAI MADRAS MEDICAL COLLEGE, CHENNAI M.D. Radio Diagnosis M.D. Radio Diagnosis 4 5 3713 SIDDHARTH P BC Service 940 COIMBATORE MEDICAL COLLEGE, COIMBATORE COIMBATORE MEDICAL COLLEGE, COIMBATORE M.D. Radio Diagnosis M.D. Radio Diagnosis 5 6 3634 LENINPRABHU P MBC/DNC Service 934.72 STANLEY MEDICAL COLLEGE , CHENNAI STANLEY MEDICAL COLLEGE , CHENNAI M.D. D.V.L M.D. D.V.L 6 7 4294 ELANGO M MBC/DNC Service 931.5 STANLEY MEDICAL COLLEGE , CHENNAI STANLEY MEDICAL COLLEGE , CHENNAI M.D. Radio Diagnosis M.D. Radio Diagnosis 7 9 6403 RAGAVI MBC/DNC Service 930.91 STANLEY MEDICAL COLLEGE , CHENNAI STANLEY MEDICAL COLLEGE , CHENNAI M.D. Radio Diagnosis M.D. Radio Diagnosis 8 10 5180 SHYAMALA M BC Service 930.35 STANLEY MEDICAL COLLEGE , CHENNAI STANLEY MEDICAL COLLEGE , CHENNAI ANTONY SHERLY M.D. General Medicine M.D. General Medicine 9 16 5772 BC Service 918.21 ROSE M MADURAI MEDICAL COLLEGE, MADURAI MADURAI MEDICAL COLLEGE, MADURAI M.D. General Medicine M.D. General Medicine 10 17 5323 C ADITHYAN BC Service 914.4 MADRAS MEDICAL COLLEGE, CHENNAI MADRAS MEDICAL COLLEGE, CHENNAI M.D. -

Directorate of Medical Education
1 Directorate of Medical Education Hand Book on Right to Information Act - 2005 2 CHAPT ER DETAILS PAGE NO NO. 1. INTRODUCTION 3 2 PARTICULARS OF ORGANISATION, FUNCTIONS AND DUTIES 5 3 POWERS AND DUTIES OF OFFICERS AND EMPLOYEES 80 4 RULES, REGULATIONS,INSTRUCTIONS, MANUAL AND RECORDS 91 FOR DISCHARGING FUNCTIONS 5 PARTICULARS OF ANY ARRANGEMENT THAT EXISTS FOR 93 CONSULTATION WITH OR REPRESENTATION BY THE MEMBERS OF THE PUBLIC IN RELATION TO THE FORMULATION OF ITS POLICY OR IMPLEMENTATION THEREOF 6 A STATEMENT OF THE CATEGORIES OF DOCUMENTS THAT ARE 94 HELD BY IT OR UNDER ITS CONTROL 7 A STATEMENT OF BOARDS, COUNCIL, COMMITTEES AND OTHER 95 BODIES CONSTITUTED AS ITS PART 8 THE NAMES, DESIGNATION AND OTHER PARTICULARS OF THE 96 PUBLIC INFORMATION OFFICER 9 PROCEDURE FOLLOWED IN DECISION MAKING PROCESS 107 10 DIRECTORY OF OFFICERS AND EMPLOYEES 108 11 THE MONTHLY REMUNERATION RECEIVED BY EACH OF ITS 110 OFFICERS AND EMPLOYEES INCLUDING THE SYSTEM OF COMPENSATION AS PROVIDED IN REGULATIONS. 12 THE BUDGET ALLOCATED TO EACH AGENCY/OFFICERS 111 (PARTICULARS OF ALL PLANS, PROPOSED EXPENDITURES AND REPORTS ON DISBURSEMENT MADE 116 13 THE MANNER OF EXECUTION OR SUBSIDY PROGRAMME 14 PARTICULARS OF RECEIPIENTS OF CONCESSIONS, PERMITS OR 117 AUTHORISATION GRANTED BY IT 15 NORMS SET BY IT FOR THE DISCHARGE OF ITS FUNCTIONS 118 16 INFORMATION AVAILABLE IN AN ELECTRONIC FORM 119 17 PARTICULARS OF THE FACILITIES AVAILABLE TO CITIZENS FOR 120 OBTAINING THE INFORMATION 18 OTHER USEFUL INFORMATION 121 3 CHAPTER-1 - INTRODUCTION 1.1This handbook is brought out by the Directorate of Medical Education (Government of Tamil Nadu) , Chennai as required by the Right to Information Act, 2005. -
Circuit ID Location District Customer Name SDC NSP CIR 240B1AB Perungudi HUB Location TNHSP HUB D CHENN NSP CIR 33EF Govt.Royepettah Hospital TNHSP Govt
Circuit ID Location District Customer Name SDC_NSP_CIR_240B1AB Perungudi HUB location TNHSP HUB D CHENN_NSP_CIR_33EF Govt.Royepettah Hospital TNHSP Govt. Royepettah Hospital Royapettah DFDF CHENN_NSP_CIR_127F Govt.Peripheral Hospital TNHSP Govt. Peripheral Hospital,Opposite Vijayashree Mahal 3rd Avenue Anna Nagar East 4959 AnnaNagar CHENN_NSP_CIR_33195 Govt.Peripheral Hospital Govt. Peripheral Hospital - TondiarpetKailasam St New Washermanpet Royapuram TNHSP 01 Tondiarpet TAMIL NADU GOVERNMENT DENTAL COLLEGE CHENN_NSP_CIR_337D and Hospital Dental Hospital TNHSP 019B OPP. PARK STATION MUTHUSAMY SALAI CHENN_NSP_CIR_1B1D King Institute - Guindy TNHSP King Institute of Preventive Medicine - Guindy 3A6C CHENN_NSP_CIR_1ADA Institute of Mental health TNHSP Institute of Mental health ,Medavakkam Tank Road, Kilpauk C559 CHENN_NSP_CIR_102F Institute of Thoracic TNHSP Institute of Thoracic Medicine, Near Egmore Taluk Office, Chetpet 6663 Medicine Regional Institute of CHENN_NSP_CIR_283A Ophthalmology _ TNHSP Regional Institute of Ophthalmology & Govt. Ophthalmic Hospital ,Old No.132, Rukmani Lakshmipathy Salai Egmore 61F2 Govt.Ophthalmic Hospital CHENN_NSP_CIR_17427 Kilpauk Medical College- TNHSP Kilpauk Medical College Hospital, Periyavar EVR Salai, Kilpauk F0D Chennai Govt.Thiruvatteeswarar CHENN_NSP_CIR_3ABF Hospital for Thoracic TNHSP Govt. Thiruvatteeswarar Hospital for Thoracic Medicine,No 60/372 Near Aynavaram Bus Depot Konnur High Road Otteri 2EDA Medicine THENI_NSP_CIR_3540E Theni Medical College TNHSP Theni Medical College Hospital,kanavillaku -

KMC Chennai Alumni Association -Annual Report 2017-18
Annual Report 2017-18 KMC Chennai Alumni Association Govt Kilpauk Medical college Poonamalle High road,Kilpauk,Chennai India 600010 KMC Chennai Alumni Association -Annual report 2017-18 KMC Chennai Alumni Association Govt Kilpauk Medical College, Ponnamalle High Road, Kilpauk, Chennai-600 010 Reg No 70/2016 ( Central Chennai ) u/s 10 of the Tamilnadu Societies Registration Act 1975 Write to us at [email protected] Web site: www.kilpaukmedicalcollege.com KMC Chennai Alumni Association -Annual report 2017-18 Objects of the Association 1] To foster a continuing educational and philanthropic rela- tionship between Kilpauk Medical College alumni and the Col- lege, Hospital, its students, and faculty 2] To facilitate the meeting of Kilpauk Medical College alumni with one another 3] To encourage Kilpauk Medical College Alumni to make contributions to Society 4] To interact with foreign institutions and arrange exchange programs 5] To publish and help in publication and / or distributing peri- odicals, monthly magazines ,newspapers ,pamphlets, books for spread and advancements of recent medical improvements and in- novations 6] Scholarship aid to undergraduate and graduate students 7] Sponsorship of community service projects 8] Sponsorship of fund raising events which will benefit the College and Hospital directly or which will benefit the Alumni in the establishment of scholarships or to provide for the expenses of operating the Alumni KMC Chennai Alumni Association -Annual report 2017-18 Kilpauk Medical College Infrastructure development -

District Census Handbook, Madras, Part XIII a and B, Series-20
CENSUS OF INDIA 1981 SERIES 20 TAMIL NADU PART xm A and B DISTRICT CENSUS HANDBOOK TOWN DIRECTORY AND DIVISIONWISE PRIMARY CENSUS ABSTRACT MADRAS A. P. MUTHUSWAMI of the Indian Administrative Service Director of Census Operations Tamil Nadu 12-2,,_ A MADRAS DISTRICT KILOMETERS 012 ._.__.; ,. I NOTE: THE BOUNDARY OF MADRAS DISTRICT IS COTERMINOUS WITH THAT OF THE 26261 MADRAS CORPORATION --- ----- 27.. 32 40 616 \ I \ / ,.-j • I 34 , _/~--'i 26625 '. _- - - I \ ,~- " . " .1 33 \, J 35637 : \.. ...., i 75 } 28245 / " ~ I ( ~ 7 .lN~~~ I . " () 21_709 I 77 "'-- ~ ____ _ I I 38901 I 79 /. Bay Division Division I I 19698,' No. popLllation I '--80 -, ) ,---- J." ______ -r _~2lB__6~I~ 1O 20548 of " 6 ' \ I 109 , . 13 19617 I 39 ~40 I (, 110 5) 25661 __ ;' t e 21278 I.... __ -- I Bengal 15 14892 f'" \ I _- - 116 J \ , _-I 23 16 18319 , I 112 Ir- - -'II ,_ 9{'5 , 17 18090 /"33777>21537)' t-f-,r'lj -' J ' .... _ ( ,_ ..... -- I 115 :,7 169' 18 20930 '\ ..... _- \ 20 20114 / 47 18991 , 1--/ 48 19211 \ \ 113 , I 30422 49 22453 \ - - 411--/ 52 17427 ~~~ 56 18917 59 25388 61 16931 137 64 13871 -_ 25907 I 65 14935 _-_ I I 66 17385 (--- ,I 67 18620 147 I I 68 23619 22 771 _L..,, ____ -- 69 14531 , I 82 20480 r- ..... _""', J-_J • I 1 150 90 14118 \' 26230 & 1 ' ...... __ I __ /1 92 18780 .~ ~ \ ,.'. 94 19421 \ , 148 \ ,/ ::: 95 21592 • 24998 1/ .-._,.~. 96 13072 \. ./' 99 18665 \. / 102 2'2148 /" 129 19906 '. -
Mbbs - 2020 - 2021 - Session List of Candidates Allotted - on 23.11.2020
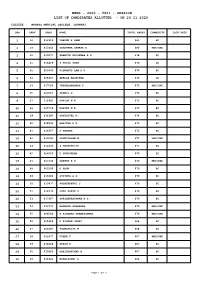
MBBS - 2020 - 2021 - SESSION LIST OF CANDIDATES ALLOTTED - ON 23.11.2020 COLLEGE : MADRAS MEDICAL COLLEGE, CHENNAI. SNO RANK ARNO NAME TOTAL MARKS COMMUNITY JOIN DATE 1 16 612916 VARUNN K SAMY 681 BC 2 19 617442 SARAVANA SANKAR B 680 MBC/DNC 3 26 610077 PRANITH KRISHNAA A G 678 BC 4 31 616829 S SELVA SREE 676 OC 5 32 620045 VISWANTH RAM K U 676 BC 6 33 615867 ADELLA AASRITHA 676 OC 7 34 617504 VENGADANADHAN P 675 MBC/DNC 8 35 603567 PRANIL G 675 BC 9 37 615981 KANIGA N N 675 BC 10 38 615558 ROHITH N D 675 BC 11 39 616397 SAKTHIVEL M 674 BC 12 40 618593 HARITHA R R 673 BC 13 41 616957 S VARSHA 672 BC 14 42 619192 SRINIVASAN M 671 MBC/DNC 15 43 613436 S MADHUPRIYA 671 BC 16 45 624055 D GURUSARAN 670 BC 17 47 617133 SAKTHI K V 670 MBC/DNC 18 48 600196 D ARUN 670 BC 19 49 613404 ATITHYA G S 670 BC 20 50 619977 PUGAZHENTHI S 670 BC 21 51 616572 JAYA SURYA C 670 BC 22 53 617667 SURYANARAYANAN M S 670 BC 23 54 613771 RAANESH PRABAKAR 670 MBC/DNC 24 55 604549 R KISHORE GNANESSHWAR 670 MBC/DNC 25 56 625854 R KISHAN JOGHI 668 BC 26 57 624497 PADMAPRIYA M 668 BC 27 58 613477 UTHRA T 667 MBC/DNC 28 59 616868 AKASH K 667 BC 29 60 619463 HARIESHKUMAR N 667 BC 30 63 618602 MAHALASHMI R 666 BC Page 1 of 5 MBBS - 2020 - 2021 - SESSION LIST OF CANDIDATES ALLOTTED - ON 23.11.2020 COLLEGE : MADRAS MEDICAL COLLEGE, CHENNAI.