Radiographic Studies on the Carpal Joints in Some Small Animals
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4Th SESSION 1
2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4th SESSION 1: Carpal Ligament 1 Stable Central Column Theory of Carpal Mechanics Michael Sandow FRACS Wakefield Orthopaedic Clinic Adelaide, Australia Background: The carpus is a complicated and functionally challenged mechanical system and advancements in the understanding have been compromised by the recognition that there is no standard carpal mechanical system and no typical wrist. This paper cover component of a larger project that seeks to develop a kinetic model of wrist mechanics to allow reverse analysis of the specific biomechanical controls or rule of a specific patient's carpus, and then use those to create a forward mathematical model to reproduce the unique individual's anatomical motion based on the extracted rules. Objectives and Methods: Based on previous observations, the carpus essentially moves with only 2 degrees of freedom - pitch (flexion / extension) and yaw (radial deviation / ulnar deviation), while largely preventing roll (pronation / supination). The object of this paper is therefore to present the background and justification to support the rules based motion (RBM) concept states that the motion of a mechanical system, such as the wrist, is the net interplay of 4 rules - morphology, constraint, interaction and load. The Stable Central Column Theory (SCCT) of wrist mechanics applies the concept of RBM to the carpus, and by using a reverse engineering computational analysis model, identified a consistent pattern of isometric constraints, creating a "Two-Gear Four-Bar" linkage. This study assessed the motion of the carpus using a 3D dynamic visualization model, and the hypothesis was that the pattern and direction of motion of the proximal row, and the distal row with respect the immediately cephalad carpal bones or radius would be very similar in all directions of wrist motion. -

Defining the Morphometrics of the First Metacarpal for the Development of an Osseointegrated Prosthesis
Defining the Morphometrics of the First Metacarpal for the Development of an Osseointegrated Prosthesis Authors: JJ Vaux OMS-IV1, RR Hugate, M.D.2, JW Hills3, RF Grzybowski, D.O.4, CK Funk. Ph.D.1 Affiliations: 1Rocky Vista University College of Osteopathic Medicine, 2Colorado Limb Consultants, 3Dept of Materials and Mechanical Engineering, Denver University, 4Diversified Radiology Objective: Amputation of the thumb presents a serious insult to the hand and can result in up to a 22% loss of functionality in that limb (2,3). To date, several different techniques have been explored for reconstruction of the thumb, however none seem to be incredibly successful (1,4). We believe the answer lies in an osseointegrated prosthesis within the first metacarpal. In order to successfully create an osseointegrated prosthesis, the morphometrics of the first metacarpal are needed. The aim of this study was to define the geometry of the first metacarpal in order to help create a standardized set of stems and prostheses to treat patients who have suffered amputation of the thumb at the level of the first metacarpal phalangeal joint (MCPJ). Methods: A total of eighty first metacarpals from forty-one cadavers were studied. All soft tissues were removed and the first metacarpals were imaged by computed tomography (CT). Three-dimensional models were constructed using cuts from the coronal, sagittal, and axial planes. Using a HyperMesh software, the individual first metacarpals were analyzed and measurements were taken for overall length, radius of curvature, medullary canal diameter, cortical thickness, and distance from the distal end to the center of the isthmus. -

Original Article Pictorial Atlas of Symptomatic Accessory Ossicles by 18F-Sodium Fluoride (Naf) PET-CT
Am J Nucl Med Mol Imaging 2017;7(6):275-282 www.ajnmmi.us /ISSN:2160-8407/ajnmmi0069278 Original Article Pictorial atlas of symptomatic accessory ossicles by 18F-Sodium Fluoride (NaF) PET-CT Sharjeel Usmani1, Cherry Sit2, Gopinath Gnanasegaran2, Tim Van den Wyngaert3, Fahad Marafi4 1Department of Nuclear Medicine & PET/CT Imaging, Kuwait Cancer Control Center, Khaitan, Kuwait; 2Royal Free Hospital NHS Trust, London, UK; 3Antwerp University Hospital, Belgium; 4Jaber Al-Ahmad Molecular Imaging Center, Kuwait Received August 7, 2017; Accepted December 15, 2017; Epub December 20, 2017; Published December 30, 2017 Abstract: Accessory ossicles are developmental variants which are often asymptomatic. When incidentally picked up on imaging, they are often inconsequential and rarely a cause for concern. However, they may cause pain or discomfort due to trauma, altered stress, and over-activity. Nuclear scintigraphy may play a role in the diagnosis and localizing pain generators. 18F-Sodium Fluoride (NaF) is a PET imaging agent used in bone imaging. Although commonly used in imaging patients with cancer imaging malignancy, 18F-NaF may be useful in the evaluation of benign bone and joint conditions. In this article, we would like to present a spectrum of clinical cases and review the potential diagnostic utility of 18F-NaF in the assessment of symptomatic accessory ossicles in patients referred for staging cancers. Keywords: 18F-NaF PET/CT, accessory ossicles, hybrid imaging Introduction Accessory ossicles are developmental variants which are often asymptomatic. When inciden- Bone and joint pain is a common presentation tally picked up on imaging, they are often incon- in both primary and secondary practice. -

The Carpometacarpal Joint of the Thumb: MR Appearance in Asymptomatic Volunteers
Skeletal Radiol (2013) 42:1105–1112 DOI 10.1007/s00256-013-1633-4 SCIENTIFIC ARTICLE The carpometacarpal joint of the thumb: MR appearance in asymptomatic volunteers Anna Hirschmann & Reto Sutter & Andreas Schweizer & Christian W. A. Pfirrmann Received: 23 January 2013 /Revised: 1 April 2013 /Accepted: 21 April 2013 /Published online: 15 May 2013 # ISS 2013 Abstract subjects. The AOL showed a variable SI (36 %/42 % low, Purpose To prospectively characterize the MR appearance 27 %/27 % increased, 36 %/30 % striated). The IML was the of the carpometacarpal (CMC) joint of the thumb in asymp- thickest ligament with a mean of 2.9 mm/3.1 mm and the tomatic volunteers. DRL the thinnest (1.2 mm/1.4 mm). There was a mean Materials and methods Thirty-four asymptomatic volun- dorsal subluxation of 1.8 mm/2.0 mm and radial subluxation teers (17 women, 17 men, mean age, 33.9±9.2 years) of 2.8 mm/3.4 mm of the metacarpal base. The AOL was underwent MR imaging of the thumb after approval by the significantly thicker in men (1.7 mm) than in women local ethical committee. Two musculoskeletal radiologists (1.2 mm; p=0.02). Radial subluxation was significantly independently classified visibility and signal intensity (SI) larger in men (3.4 mm) than in women (2.2 mm; p=0.02). characteristics of the anterior oblique (AOL/beak ligament), No subluxation in palmar or ulnar direction was seen. the posterior oblique (POL), the intermetacarpal (IML), and Conclusions Radial and dorsal subluxation of the CMC the dorsoradial ligaments (DRL) on a three-point Likert joint can be a normal finding in a resting position at MR scale. -

REVIEW ARTICLE Osteoarthritis of the Wrist
REVIEW ARTICLE Osteoarthritis of the Wrist Krista E. Weiss, Craig M. Rodner, MD From Harvard College, Cambridge, MA and Department of Orthopaedic Surgery, University of Connecticut Health Center, Farmington, CT. Osteoarthritis of the wrist is one of the most common conditions encountered by hand surgeons. It may result from a nonunited or malunited fracture of the scaphoid or distal radius; disruption of the intercarpal, radiocarpal, radioulnar, or ulnocarpal ligaments; avascular necrosis of the carpus; or a developmental abnormality. Whatever the cause, subsequent abnormal joint loading produces a spectrum of symptoms, from mild swelling to considerable pain and limitations of motion as the involved joints degenerate. A meticulous clinical and radiographic evaluation is required so that the pain-generating articulation(s) can be identi- fied and eliminated. This article reviews common causes of wrist osteoarthritis and their surgical treatment alternatives. (J Hand Surg 2007;32A:725–746. Copyright © 2007 by the American Society for Surgery of the Hand.) Key words: Wrist, osteoarthritis, arthrodesis, carpectomy, SLAC. here are several different causes, both idio- of events is analogous to SLAC wrist and has pathic and traumatic, of wrist osteoarthritis. been termed scaphoid nonunion advanced collapse Untreated cases of idiopathic carpal avascular (SNAC). Wrist osteoarthritis can also occur second- T 1 2 necrosis, as in Kienböck’s or Preiser’s disease, may ary to an intra-articular fracture of the distal radius or result in radiocarpal arthritis. Congenital wrist abnor- ulna or from an extra-articular fracture resulting in malities, such as Madelung’s deformity,3,4 can lead malunion and abnormal joint loading. -
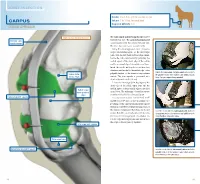
Carpus Volume: 7 to 10 Ml for Each Joint Degree of Difficulty: 1/3 Dorsal Approach
JOINT INJECTION needle: 1 to 1.5 in. (2.5 to 3.8 cm), 20 ga Carpus volume: 7 to 10 ml for each joint Degree of difficulty: 1/3 Dorsal approach right carpus, dorsomedial view The radiocarpal and intercarpal joints can be extensor carpi entered with ease. The carpometacarpal joint radialis tendon communicates with the intercarpal joint and, therefore, does not require separate entry. Using the dorsal approach, enter the radio- carpal (antebrachiocarpal) or the intercarpal joints with the limb held and the carpus flexed. Locate the radiocarpal joint by palpating the medial aspect of the distal edge of the radius and the proximal edge of the radial carpal bone. Insert the needle midway between these two structures and medial to the medial edge of the palpate the radiocarpal and intercarpal joints medial to palpable tendon of the extensor carpi radialis radius (distal the palpable tendon of the extensor carpi radialis muscle. medial edge) muscle. The joint capsule is penetrated at a Note: The right carpus is being palpated. depth of about 0.5 inch (1.3 cm). Locate the intercarpal joint by palpating the distal edge of the radial carpal bone and the medial aspect of the proximal edge of the third radial carpal bone (proximal carpal bone. The technique of needle insertion edge) is similar to that for the radiocarpal joint. radiocarpal joint capsule It is important to point out that Ford et al47 and Moyer et al48 showed that the palmar out- pouchings of the carpometacarpal joint capsule extend into the fibers of the proximal portion of the suspensory ligament. -

Readingsample
Color Atlas of Human Anatomy Vol. 1: Locomotor System Bearbeitet von Werner Platzer 6. durchges. Auflage 2008. Buch. ca. 480 S. ISBN 978 3 13 533306 9 Zu Inhaltsverzeichnis schnell und portofrei erhältlich bei Die Online-Fachbuchhandlung beck-shop.de ist spezialisiert auf Fachbücher, insbesondere Recht, Steuern und Wirtschaft. Im Sortiment finden Sie alle Medien (Bücher, Zeitschriften, CDs, eBooks, etc.) aller Verlage. Ergänzt wird das Programm durch Services wie Neuerscheinungsdienst oder Zusammenstellungen von Büchern zu Sonderpreisen. Der Shop führt mehr als 8 Millionen Produkte. 130 Upper Limb: Bones, Ligaments, Joints Radiocarpal and Midcarpal Joints Ligaments in the Region of the Wrist (A–E) (A–E) Four groups of ligaments can be distin- The radiocarpal or wrist joint is an ellip- guished: soid joint formed on one side by the radius (1) and the articular disk (2) and on the Ligaments which unite the forearm bones with other by the proximal row of carpal bones.Not the carpal bones (violet). These include the all the carpal bones of the proximal row are ulnar collateral ligament (8), the radial col- in continual contact with the socket- lateral ligament (9), the palmar radiocarpal shaped articular facet of the radius and the ligament (10), the dorsal radiocarpal liga- disk. The triquetrum (3), only makes close ment (11), and the palmar ulnocarpal liga- contact with the disk during ulnar abduc- ment (12). tion and loses contact on radial abduction. Ligaments which unite the carpal bones with The capsule of the wrist joint is lax, dorsally one another,orintercarpal ligaments (red). These comprise the radiate carpal ligament Upper Limb relatively thin, and is reinforced by numer- ous ligaments. -

Orthopaedics Instructions: to Best Navigate the List, First Download This PDF File to Your Computer
Orthopaedics Instructions: To best navigate the list, first download this PDF file to your computer. Then navigate the document using the bookmarks feature in the left column. The bookmarks expand and collapse. Finally, ensure that you look at the top of each category and work down to review notes or specific instructions. Bookmarks: Bookmarks: notes or specific with expandable instructions and collapsible topics As you start using the codes, it is recommended that you also check in Index and Tabular lists to ensure there is not a code with more specificity or a different code that may be more appropriate for your patient. Copyright APTA 2016, ALL RIGHTS RESERVED. Last Updated: 09/14/16 Contact: [email protected] Orthopaedics Disorder by site: Ankle Achilles tendinopathy ** Achilles tendinopathy is not listed in ICD10 M76.6 Achilles tendinitis Achilles bursitis M76.61 Achilles tendinitis, right leg M76.62 Achilles tendinitis, left leg ** Tendinosis is not listed in ICD10 M76.89 Other specified enthesopathies of lower limb, excluding foot M76.891 Other specified enthesopathies of right lower limb, excluding foot M76.892 Other specified enthesopathies of left lower limb, excluding foot Posterior tibialis dysfunction **Posterior Tibial Tendon Dysfunction (PTTD) is not listed in ICD10 M76.82 Posterior tibial tendinitis M76.821 Posterior tibial tendinitis, right leg M76.822 Posterior tibial tendinitis, left leg M76.89 Other specified enthesopathies of lower limb, excluding foot M76.891 Other specified enthesopathies of right lower limb, -

The Skeletal System
Essentials of Human Anatomy & Physiology Seventh Edition Foundation • Physical Foundation of the Body The Skeletal System – 206 Bones • Osteology – science of the anatomy, structure, and function of bones – “Os” means Bone • With the exception of teeth, bone IS the hardest substance in the body Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings The Skeletal System • Parts of the skeletal system • Bones (skeleton) • Joints • Cartilages • Ligaments (bone to bone)(tendon=bone to muscle) • Divided into two divisions • Axial skeleton • Copyright © 2003Appendicular Pearson Education, Inc. publishing as Benjaminskeleton Cummings – limbs and girdle 1 Functions of Bones Bones of the Human Body • The skeleton has 206 bones • Support of the body • Two basic types of bone tissue • Protection of soft organs • Compact bone • Movement due to attached skeletal • Homogeneous muscles • Spongy bone • Storage of minerals and fats (K, Mg, • Small needle-like pieces of bone Na) Figure 5.2b • Many open spaces • Blood cell formation (White and Red) Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings Classification of Bones Classification of Bones • Long bones • Short bones • Typically longer than wide • Generally cube-shape • Have a shaft with heads at both ends • Contain mostly spongy bone • Contain mostly compact bone •Examples: Carpals, tarsals • Examples: Femur, humerus Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings 2 Classification of Bones on the Classification of Bones Basis of Shape • Flat bones • Thin and flattened • Usually curved • Thin layers of compact bone around a layer of spongy bone •Examples: Skull, ribs, sternum Figure 5.1 Copyright © 2003 Pearson Education, Inc. -

(Bucked Shins) in the Flat Racing Horse: Prevalence, Diagnosis, Pathogenesis, and Associated Factors
Journal of Dairy, Veterinary & Animal Research Mini Review Open Access A review of dorsal metacarpal disease (bucked shins) in the flat racing horse: prevalence, diagnosis, pathogenesis, and associated factors Abstract Volume 5 Issue 6 - 2017 Dorsal metacarpal disease (DMD) is the most common cause of lostdays to training S Couch,1 BD Nielsen2 and racing in Thoroughbred racehorses. Colloquially termed ‘bucked’ or ‘sore’ shins, 1Royal (Dick) School of Veterinary Studies, University of this initially painful condition commonly occurs in the first season of training and can Edinburgh, United Kingdom raise welfare concerns. Clinical signs include pain with digital palpation and swelling 2Department of Animal Science, Michigan State University, USA on the dorsal, and sometimes dorso-medial, aspect of the third metacarpal (McIII). Periostitis and excessive growth of periosteal bone can be present as a response to Correspondence: Brian D Nielsen, Michigan State University, high strain cyclic fatigue. Whilst DMD can resolve with rest or reduced exercise, it Department of Animal Science, 474 S. Shaw Lane, East Lansing, can leave bone susceptible to future catastrophic fracture at the same site, particularly MI 48824 1225, USA, Tel 517 432 1378, Fax 517 353 1699, saucer fractures of the lamellar bone of the diaphysis. Some trainers continue to work Email [email protected] an animal through DMD, with the view that it will only happen once, but it can re- occur. Additionally, the animal is in discomfort and has a weakened skeletal system. Received: September 13, 2017 | Published: September 25, In vivo studies of the effects of cyclic strain on the skeletal system of Thoroughbreds 2017 are notoriously difficult, due to the many variables involved and in vitro studies cannot mimic true training and racing conditions. -

Clinical Medical Policy
CLINICAL MEDICAL POLICY Noninvasive Electrical Bone Growth Stimulators Policy Name: (osteogenesis stimulators) Policy Number: MP-070-MD-PA Responsible Department(s): Medical Management Provider Notice Date: 12/15/2018 Issue Date: 01/15/2019 Effective Date: 01/15/2019 Annual Approval Date: 10/17/2019 Revision Date: N/A Products: Gateway Health℠ Medicaid Application: All participating hospitals and providers Page Number(s): 1 of 78 DISCLAIMER Gateway Health℠ (Gateway) medical policy is intended to serve only as a general reference resource regarding coverage for the services described. This policy does not constitute medical advice and is not intended to govern or otherwise influence medical decisions. POLICY STATEMENT Gateway Health℠ may provide coverage under the medical-surgical and DME benefits of the Company’s Medicaid products for medically necessary noninvasive electrical bone growth stimulators as treatment of nonunion long bone fractures or congenital pseudarthrosis. This policy is designed to address medical necessity guidelines that are appropriate for the majority of individuals with a particular disease, illness or condition. Each person’s unique clinical circumstances warrant individual consideration, based upon review of applicable medical records. (Current applicable Pennsylvania HealthChoices Agreement Section V. Program Requirements, B. Prior Authorization of Services, 1. General Prior Authorization Requirements.) Policy No. MP-070-MD-PA Page 1 of 78 DEFINITIONS Prior Authorization Review Panel - A panel of representatives from within the PA Department of Human Services who have been assigned organizational responsibility for the review, approval and denial of all PH-MCO Prior Authorization policies and procedures. Non-invasive (Osteogenic) Electrical Bone Growth Stimulator – A device that uses pulsed- electromagnetic fields, capacitative coupling or combined magnetic fields to generate a weak electric current through the target site. -

Four Unusual Cases of Congenital Forelimb Malformations in Dogs
animals Article Four Unusual Cases of Congenital Forelimb Malformations in Dogs Simona Di Pietro 1 , Giuseppe Santi Rapisarda 2, Luca Cicero 3,* , Vito Angileri 4, Simona Morabito 5, Giovanni Cassata 3 and Francesco Macrì 1 1 Department of Veterinary Sciences, University of Messina, Viale Palatucci, 98168 Messina, Italy; [email protected] (S.D.P.); [email protected] (F.M.) 2 Department of Veterinary Prevention, Provincial Health Authority of Catania, 95030 Gravina di Catania, Italy; [email protected] 3 Institute Zooprofilattico Sperimentale of Sicily, Via G. Marinuzzi, 3, 90129 Palermo, Italy; [email protected] 4 Veterinary Practitioner, 91025 Marsala, Italy; [email protected] 5 Ospedale Veterinario I Portoni Rossi, Via Roma, 57/a, 40069 Zola Predosa (BO), Italy; [email protected] * Correspondence: [email protected] Simple Summary: Congenital limb defects are sporadically encountered in dogs during normal clinical practice. Literature concerning their diagnosis and management in canine species is poor. Sometimes, the diagnosis and description of congenital limb abnormalities are complicated by the concurrent presence of different malformations in the same limb and the lack of widely accepted classification schemes. In order to improve the knowledge about congenital limb anomalies in dogs, this report describes the clinical and radiographic findings in four dogs affected by unusual congenital forelimb defects, underlying also the importance of reviewing current terminology. Citation: Di Pietro, S.; Rapisarda, G.S.; Cicero, L.; Angileri, V.; Morabito, Abstract: Four dogs were presented with thoracic limb deformity. After clinical and radiographic S.; Cassata, G.; Macrì, F. Four Unusual examinations, a diagnosis of congenital malformations was performed for each of them.