Research Associate Applicant
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Match Day 2009
Medical School News Match Day 2009 This year’s Match Day festivities took place on March 19 at the Pearl Street Grill and Brewery in Photos David Feiner, pictured with his father, By Marc, and mother, Elise, is staying in downtown Buffalo, where students, their families and friends and faculty gathered to celebrate. Nancy Parisi Buffalo to train in orthopaedic surgery. He wore his father’s scrubs for the special occasion. Ajay Prakash Abad Mimi Z. Amberger Jee Bang (continued) Andrew Michael Baschnagel William Frederick Bevilacqua Margherita Bruni Jason C. Choi Urmi A. Desai Neurology Surgery Neurology Radiation–Oncology Surgery Otolaryngology Internal Medicine Family Medicine University of Rochester/Strong San Diego Naval Medical Center Johns Hopkins Hospital, William Beaumont Hospital University at Buffalo University of South Florida College Beth Israel Deaconess Medical Center New York Presbyterian Hospital Memorial Hospital San Diego, CA Baltimore, MD Royal Oak, MI Buffalo, NY of Medicine Boston, MA (Columbia) Rochester, NY 9 Tampa, FL New York, NY Stephanie Lyn Andrus Pamela Dorothy Bannon Torsten Behrens Sandeep Rao Bhashyam Baishakhi Choudhury Sameer Madhav Deshmukh Katie Roseann Agnello Pediatrics Emergency Medicine Emergency Medicine Internal Medicine Andrew J. Bukowinski Otolaryngology Surgery–Preliminary Internal Medicine North Shore, Long Island Jewish Hospital of the University of University at Buffalo Stony Brook Teaching Hospitals Pediatrics University of North Carolina Massachusetts General Hospital University of Rochester/Strong Health System Pennsylvania Buffalo, NY Stony Brook, NY University of Pittsburgh Medical Hospitals Boston, MA Memorial Hospital Manhasset, NY Philadelphia, PA Center Chapel Hill, NC 2009Rochester, NY Pittsburgh, PA Urology Colleen Elizabeth Bell Drew T. -
Buffalo Building Project
BUFFALO BUILDING reuse PROJECT Developed at the request of Mayor Byron Brown TABLE OF CONTENTS Executive Summary............................................................... pg 2 Project Recommendations - Overview..................................... pg 3-4 Project Background............................................................... pg 5 Project Participants............................................................... pg 6 Project Scope and Focus........................................................ pg 7-11 Downtown Challenges and Opportunities............................... pg 12-16 Project Recommendations in Detail........................................ pg 17-25 Anticipated Outcomes........................................................... pg 26-28 Resources and References .................................................... pg 29-30 Resources and References................................................... Thank you to National Fuel for their generous support on this project 1 Buffalo Building Reuse | Report 2012 EXECUTIVE SUMMARY visible part. However, redeveloping To stimulate near-term investments Mayor Brown calls for downtown’s class B and C buildings in this type of redevelopment, recommendations to entails a difficult and complicated it is recommended programs revitalize downtown and process, which requires a multi-year and incentives be targeted to dedicated investment of resources strategic mixed use and residential encourage investment. (staff, tools and funding), which should opportunities. These programs come -

50 Thruway Plaza Drive Cheektowaga (Buffalo), NY 14225 2 2 SANDS INVESTMENT GROUP EXCLUSIVELY MARKETED BY
1 IHOP 50 Thruway Plaza Drive Cheektowaga (Buffalo), NY 14225 2 2 SANDS INVESTMENT GROUP EXCLUSIVELY MARKETED BY: ADAM SCHERR Lic. # 01925644 310.853.1266 | DIRECT [email protected] 11900 Olympic Blvd, Suite 490 Los Angeles, CA 90064 844.4.SIG.NNN www.SIGnnn.com In Cooperation With SIG RE Services NY LLC Lic. # 10991233211 BoR: Andrew AcKerman - Lic. # 10491210161 3 SANDS INVESTMENT GROUP 3 TABLE OF CONTENTS 04 06 07 13 15 INVESTMENT OVERVIEW LEASE ABSTRACT PROPERTY OVERVIEW AREA OVERVIEW TENANT OVERVIEW Investment Summary Lease Summary Property Images City Overview Tenant Profile Investment Highlights Rent Roll Location, Aerials & Retail Maps Demographics © 2021 Sands Investment Group (SIG). The information contained in this ‘Offering Memorandum’, has been obtained from sources believed to be reliable. Sands Investment Group does not doubt its accuracy; however, Sands Investment Group makes no guarantee, representation or warranty about the accuracy contained herein. It is the responsibility of each individual to conduct thorough due diligence on any and all information that is passed on about the property to determine its accuracy and completeness. Any and all proJections, market assumptions and cash flow analysis are used to help determine a potential overview on the property, however there is no guarantee or assurance these proJections, market assumptions and cash flow analysis are subJect to change with property and market conditions. Sands Investment Group encourages all potential interested buyers to seek advice from your tax, financial and legal advisors before making any real estate purchase and transaction. SANDS INVESTMENT GROUP 4 4 INVESTMENT SUMMARY Sands Investment Group is Pleased to Present Exclusively For Sale the 4 , 022 SF IHOP Located at 50 Thruway Plaza Drive in Cheektowaga (Buffalo), NY. -

PHILANTHROPY at Work
Annual Report 2013 PHILANTHROPY at Work Kaleida Health Foundation | Women & Children’s Hospital of Buffalo Foundation The John R. Oishei Children’s Hospital Message from the President and CEO Philanthropy and volunteerism are embedded in the Western New York community and Kaleida Health. Through the generous contributions of individuals, physicians, “Many of our hospitals were founded through corporations, foundations and our employees, we are able philanthropic efforts and like our past, so many to support state-of-the-art equipment, research, education, community health/wellness programs, and charity care. Many of our successes today are a direct result of donor of our hospitals were founded through philanthropic efforts and like our past, so many of our successes today are a direct engagement and support.” result of donor engagement and support. With more than 155 years of experience and a remarkable history of medical advances and breakthroughs, we are constantly seeking new ways to care for our patients with skill and compassion. Our expert medical team is leading the way with groundbreaking research, technology, and partnerships with the Buffalo Niagara Medical Campus, the State University of New York at Buffalo School of Medicine, ECMC and Roswell Park. Every day we are finding new ways to ensure that our patients have access to the most modern, safe and effective medical care possible. Kaleida Health is experiencing exciting momentum. On the horizon is construction of The John R. Oishei Children’s Hospital, Western New York’s first new children’s hospital in over 120 years. Our physician-led steering committee is spearheading the planning process for this hospital on the Buffalo Niagara Medical Campus. -

Curriculum Vitae
Curriculum Vitae Brian J. Page, MD FACC July, 2015 ______________________________________________________________________ Current Academic Position: Associate Professor of Medicine Office Address: Clinical & Translational Research Center 875 Ellicott Street, Room 7030 Buffalo, New York 14203 Phone: 716-829-2663 Fax: 716-854-1840 Email: [email protected] Licensure: New York State, January 2006 – present ______________________________________________________________________ Education BA Biochemistry (Summa cum Laude), Canisius College, Buffalo, NY, May, 1999. MD State University of New York at Buffalo School of Medicine (cum Laude), Buffalo, NY, June 2003. Post-Doctoral Training 2003 – 2006 Medical Intern/Resident, State University of New York at Buffalo, Internal Medicine Residency Program, Buffalo, NY. 2006 – 2009 Fellow in Cardiovascular Disease and Instructor of Medicine, State University of New York at Buffalo, Buffalo, NY. Brian J. Page, MD December, 2014 Board Certifications 2006 – 2016 American Board of Internal Medicine 2009 – 2019 American Board of Internal Medicine – Cardiovascular Disease 2009 – 2019 Certification Board of Nuclear Cardiology Academic Appointments 7/2009 – present Research Assistant Professor of Medicine, State University of New York at Buffalo, Buffalo, NY. Administrative Positions 7/2008 – 6/2009 Chief Cardiology Fellow 7/2013 – 2/2014 Associate Program Director, Fellowship in Cardiovascular Disease 3/2014 – present Program Director, Fellowship in Cardiovascular Disease Honors and Awards 1. Lawrence H. Golden, MD Intern Award for Humanistic and Scientific Excellence in Patient Care, State University of New York at Buffalo Internal Medicine Residency Program, June 2004. 2. SUNY at Buffalo 9th Annual Resident Scholarly Exchange day. “Myocardial proteomic profiling demonstrates that overexpressing fibroblast growth factor (AdvFGF-5) normalizes metabolic and stress protein expression in swine with hibernating myocardium”, Poster, 1st Place, May 2006. -

News Release
NEWS RELEASE FOR IMMEDIATE RELEASE Contact: Michael P. Hughes (716) 983-3731 [email protected] KALEIDA HEALTH NAMES NEW SYSTEM CHIEF OPERATING OFFICER BUFFALO, N.Y. (October 16, 2014) – Jamal A. Ghani, MBA, MHA today was named executive vice president and system chief operating officer for Kaleida Health. Ghani comes to Buffalo from the Cleveland Clinic Florida, where he served as the chief executive administrative officer. Cleveland Clinic Florida, located in Weston, West Palm Beach, Palm Beach Gardens and Parkland, Florida is part of the world renowned Cleveland Clinic. “We are very proud to have Jamal join our team,” said Jody Lomeo, president & CEO of Kaleida Health. “He will bring a national perspective to the organization, helping align our operations, improve quality of care, as well as patient satisfaction. Having a Cleveland Clinic alumnus like Jamal will be great for Kaleida Health and the patients we serve.” As system chief operating officer, Ghani will be responsible for the growth, development and leadership over Kaleida Health’s operating divisions, including its four hospitals, the Visiting Nursing Association of Western New York, long term care, as well as its ambulatory network. Prior to his appointment at the Cleveland Clinic, Ghani was the president of Metro Health Systems in Wyoming, Michigan. Metro Health includes Metro Health Hospital, a major teaching osteopathic hospital affiliated with Michigan State University as well as 17 neighborhood physician offices, certified medical homes, located throughout West Michigan, a Cancer Center developed in partnership with the University of Michigan’s Department of Radiation Oncology, plus joint ventures with other healthcare providers. -
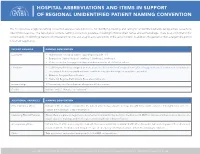
Hospital Abbreviations and Items in Support of Regional Unidentified Patient Naming Convention
HOSPITAL ABBREVIATIONS AND ITEMS IN SUPPORT OF REGIONAL UNIDENTIFIED PATIENT NAMING CONVENTION This tool provides a regional naming convention and associated protocols for identifying, tracking, and caring for unidentified patients during a mass casualty in- cident (MCI) response. The table below contains naming convention guidance, including for first and last names and estimated age. There is also information for incorporation of identifying features into the patient record, and a tag to associate victims of the same incident. In addition, the guidance offers a target time period for patient registration. PATIENT VARIABLE NAMING CONVENTION Last Name • Abbreviation of hospital name + digit (beginning with “1”) • Example for General Hospital: GenHosp1, GenHosp2, GenHosp3 • Please see below for suggested hospital abbreviations for all GNYHA members First Name • Each hospital has been assigned an item; please see below for list of assigned items, plus 50 suggested names for that item. Hospitals are encouraged to develop additional names within their assigned item type beyond those provided. • Example: Assigned Item = Flowers • Name list: Begonia, Daffodil, Lily, Rose, Lilac, Dahlia, etc. Estimated Age 1/1/estimated year of birth (based on hospital staff observation) Gender Indicate “male,” “female,” or “unknown” ADDITIONAL VARIABLES NAMING CONVENTION If the Patient is a Minor Indicate in the medical record whether the patient arrived unaccompanied or was brought in by or with someone. If brought in by someone, capture the individual’s contact information. Identifying Physical Features Ensure there is a place on registration documentation and within the electronic medical record (EMR) to capture information about tattoos, un- usual features or markings, and their location, which could help with identification. -

CHANGES in GOVERNANCE: Interviews with New York State Healthcare Leaders
CHANGES IN GOVERNANCE: Interviews with New York State Healthcare Leaders September 2018 CHANGES IN GOVERNANCEa 1 CHANGES IN GOVERNANCE INTRODUCTION Since our first Changes in Governance report, published in 2017, we continue to see significant transformation in the healthcare environment, with a growing number of affiliations occurring and major care delivery reform. These changes are impacting the way governance is structured both at the system and local stand-alone hospital board levels. This report highlights 11 interviews conducted with thought leaders from across the state about their experiences and views on the changing role of governance. These interviews were conducted by Sue Ellen Wagner, Executive Director, HTNYS, between fall 2017 and spring 2018. HTNYS extends special thanks to these leaders for taking the time to share their valuable insight for this report. GOVERNANCE TRENDS Governance trends identified during the interviews include: Governance structures are changing at both the health system and stand-alone hospital board level. Health systems are continuing to get larger. Many local stand-alone hospital board roles and responsibilities are changing as these facilities become part of health systems. Diversifying boards and recruiting younger board members remains challenging. Many board members are working full-time jobs and have little time for education, even though they feel board education is extremely important. Many boards are allowing videoconferencing for those trustees who travel out of town for the winter months or who live in another state. It is important to maintain a personal “feel” to meetings. Some system boards have begun to examine the number of committee meetings and board meetings they have. -

Atbuffalo Spring 15.Pdf
UB Boxing’s unlikely champs p28 Toxic algae in Lake Erie p34 How smart is your suitcase? p11 The magazine for alumni and friends of the State University of New York at Buffalo Spring 2015 UB alum Tzippy Salamon on life and the art of dressing p22 Absolutely Fabulous A D B F FIRST LOOK Photograph by Douglas Levere From the Ground Up As night falls over downtown Buffalo, halogen lights shine on the construction site for the future UB medical school on the Buffalo Niagara Medical Campus. Foundations are being set for the 628,000-square-foot building, which is currently the largest medical education facility under construction in the U.S. When complete, it will provide the equivalent of 11 football fields of floor space, while its location will put more than 2,000 students, faculty and staff within walking distance of some of Buffalo’s C top landmarks, including the Anchor Bar E and Shea’s Performing Arts Center. Birds-eye View A The Roosevelt Apartments are approximately half the height of the future medical school. B The existing Niagara Frontier Transportation Authority (NFTA) station will be integrated into the new medical school building. C The Conventus Medical Office Building will include UBMD and Kaleida Health as anchor tenants. D A future passageway will link Allen Street to the medical campus. E Large support beams, or “rakers,” prevent the NFTA Metro subway tunnel from moving. F “Soldier piles”—stacks of many pieces of lumber— form the retaining walls. At Buffalo SPRING 2015 1 2 SPRING 2015 At Buffalo Table of Contents Spring28 -
ANNUAL REPORT 2014-2015 a New Era in Workforce Development
B U O I o BUFFALOB UFFALO ANDAND ERIE CCOUNTYOUNTY WorkforceWWorkfororkforororkforce Investment BoardBoard ANNUAL REPORT 2014-2015 A new era in workforce development Canalside Larkinville SolarCity Buffalo Niagara Medical Campus Photos by © Joe Cascio Contents Board Chairman’s Message..........2 Executive Director’s Message.....3 Career Center Services..................4 Career Center Locations ...............9 Business Services ...........................10 Youth Services .................................12 Alternate Funding Sources ........14 Financial Summary.........................16 Board of Directors.......Back Cover WIB ANNUAL REPORT 2014-2015 BUFFALOB UFFUFFALO ANDAND ERIE COUNTYC OUNTY WorkforceWWorkforor ceorkfor Investment BoardBoard Established under the provisions of the Workforce Investment Act (WIA) of 1998, the Workforce Investment Board (WIB) is a private sector-driven board appointed by Erie County Executive Mark C. Poloncarz and City of Buffalo Mayor Byron W. Brown. The WIB is charged with developing, coordinating and overseeing publicly funded workforce development/training initiatives. Developing and maintaining a high-quality workforce is critical to attracting and retaining business in Erie County. W I o The WIB maintains a workforce development system that is user friendly and responsive to the needs of both the individual trainee/job applicant and the business organization seeking our assistance. 1 The heart of our system is our One Stop Career Centers. These Centers offer a multitude of resources for job seekers and businesses, all under one roof. The typical One Stop Career Center serves thousands of individuals who are seeking employment, changing jobs, reentering the workforce or learning new skills. On July 1, 2015, a new era in Workforce Development began for Buffalo and Erie County as new legislation under the Workforce Innovation and Opportunity Act (WIOA) of 2014 went into effect, replacing the WIA. -

The Upstate New York Stakeholder Proceedings
Brief Report Establishing Recommendations for Stroke Systems in the Thrombectomy Era The Upstate New York Stakeholder Proceedings Zainab Magdon-Ismail, DrPH; Curtis Benesch, MD; Jeremy T. Cushman, MD, MS; Ian Brissette, PhD; Andrew M. Southerland, MD, MSc; Ethan S. Brandler, MD, MPH; Cemal B. Sozener, MD, MEng; Sue Flor, BS; Roseanne Hemmitt, BA; Kathleen Wales, BS; Krystal Parrigan, MS, HSA; Steven R. Levine, MD; on behalf of the Upstate New York Stroke Work Groups Background and Purpose—The American Heart Association/American Stroke Association and Department of Health Stroke Coverdell Program convened a stakeholder meeting in upstate NY to develop recommendations to enhance stroke systems for acute large vessel occlusion. Downloaded from Methods—Prehospital, hospital, and Department of Health leadership were invited (n=157). Participants provided goals/ concerns and developed recommendations for prehospital triage and interfacility transport, rating each using a 3-level impact (A [high], B, and C [low]) and implementation feasibility (1 [high], 2, and 3 [low]) scale. Six weeks later, participants finalized recommendations. Results—Seventy-one stakeholders (45% of invitees) attended. Six themes around goals/concerns emerged: (1) emergency http://stroke.ahajournals.org/ medical services capacity, (2) validated prehospital screening tools, (3) facility capability, (4) triage/transport guidelines, (5) data capture/feedback tools, and (6) facility competition. In response, high-impact (level A) prehospital recommendations, stratified by implementation feasibility, were (1) use of online medical control for triage (6%); (2) regional transportation strategy (31%), standardized emergency medical services checklists (18%), quality metrics (14%), standardized prehospital screening tools (13%), and feedback for performance improvement (7%); and (3) smartphone application algorithm for screening/decision-making (6%) and ambulance-based telemedicine (6%). -

SUNY Buffalo
UNIVERSITY OF MARYLAND Colvin Institute of Real Estate Development 2018 Case Study Challenge Team 7 “We look at each of the different stakeholders needs - the community, tenants, developer, and investors - on - Paul F. Ciminelli - President & CEO Conventus, we came in 4 for 4.” Ciminelli Real Estate Corporation • With over 20 partners in • An estimated 1,500 • Conventus surpassed all design, engineering and visitors/patients come financial metrics that construction, Conventus through Conventus’ doors Ciminelli Real Estate was completed on time and each week. The impact on Corporation had set out on budget delivering one of the Buffalo Niagara Medical with from inception. the premier Class A Campus is impressive with properties in Buffalo, NY. housing prices and incomes • Conventus was 95% in all surrounding leased prior to its • Nearly 50% of Conventus neighborhoods on the rise. completion; an indication of incorporates recycled the acknowledgment and the building content materials, • Conventus is a catalyst for acceptance of the Buffalo and over 25% of total new development in the Niagara Medical Campus materials were extracted, Buffalo Niagara Medical as a regional leader in the processed and Campus and surrounding medical and life sciences manufactured regionally, Western New York Region. fields, and specifically, of within 500 miles of the site. Conventus as an integral part of the Campus itself. Table of Contents page 3 Introduction page 11 Building Analysis page 4 Context page 14 Sustainability page 6 Development Team page 15 Financials