Assessment of the USAID/Bangladesh Component of DELIVER Project a Success to Build On
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

View IFT /PQ / REOI / RFP Notice Details
View IFT /PQ / REOI / RFP Notice Details Ministry : Ministry of Housing and Division : Public Works Organization : Public Works Department Procuring Entity Name Rajshahi PWD Division-2 (PWD) : Procuring Entity Code : Raj02 Procuring Entity Rajshahi District : Procurement Nature : Works Procurement Type : NCT Event Type : TENDER Invitation for : Tender - Single Lot Invitation Reference 942,Date-05/02/2019 No. : App ID : 149149 Tender/Proposal ID : 280821 Key Information and Funding Information : Procurement Method : Open Tendering Method Budget Type : Development (OTM) Source of Funds : Government Particular Information : Project Code : 560 / mosques Project Name : Establishing 560 model mosques and Islamic Cultural Centers in Zila and Upazila of Bangladesh Tender/Proposal Model Mosque/Puthia Package No. and Construction of 3 Storied Building with 3 Storied Foundation of Puthia Upazila Description : Model Masjid in the District of Rajshahi Under the project of Establishment of 560 Model Masjid and Islamic Cultural Centers in Zilla and Upazilla of Bangladesh FY-2018-2019. Category : Construction work;Site preparation work;Building demolition and wrecking work and earthmoving work;Test drilling and boring work;Works for complete or part construction and civil engineering work;Building construction work;Engineering works and construction works;Construction work for pipelines, communication and power lines, for highways, roads, airfields and railways; flatwork;Construction work for water projects;Construction works for plants, mining and manufacturing -

Esdo Profile
ECO-SOCIAL DEVELOPMENT ORGANIZATION (ESDO) ESDO PROFILE Head Office Address: Eco-Social Development Organization (ESDO) Collegepara (Gobindanagar), Thakurgaon-5100, Thakurgaon, Bangladesh Phone:+88-0561-52149, +88-0561-61614 Fax: +88-0561-61599 Mobile: +88-01714-063360, +88-01713-149350 E-mail:[email protected], [email protected] Web: www.esdo.net.bd Dhaka Office: ESDO House House # 748, Road No: 08, Baitul Aman Housing Society, Adabar,Dhaka-1207, Bangladesh Phone: +88-02-58154857, Mobile: +88-01713149259, Email: [email protected] Web: www.esdo.net.bd 1 Eco-Social Development Organization (ESDO) 1. Background Eco-Social Development Organization (ESDO) has started its journey in 1988 with a noble vision to stand in solidarity with the poor and marginalized people. Being a peoples' centered organization, we envisioned for a society which will be free from inequality and injustice, a society where no child will cry from hunger and no life will be ruined by poverty. Over the last thirty years of relentless efforts to make this happen, we have embraced new grounds and opened up new horizons to facilitate the disadvantaged and vulnerable people to bring meaningful and lasting changes in their lives. During this long span, we have adapted with the changing situation and provided the most time-bound effective services especially to the poor and disadvantaged people. Taking into account the government development policies, we are currently implementing a considerable number of projects and programs including micro-finance program through a community focused and people centered approach to accomplish government’s development agenda and Sustainable Development Goals (SDGs) of the UN as a whole. -

Medicinal Plants Used by the Village Pania Under Baghmara District
ANALYSISANALYSIS ARTICLE 54(266), February 1, 2018 ISSN 2278–5469 EISSN 2278–5450 Discovery Medicinal plants used by the local people at the village Pania under Baghmara Upazila of Rajshahi District, Bangladesh Mst. Mafroja Khatun, Mahbubur Rahman AHM☼ Plant Taxonomy Laboratory, Department of Botany, Faculty of Life and Earth Sciences, University of Rajshahi, Rajshahi-6205, Bangladesh ☼Corresponding Author: Professor, Department of Botany, Faculty of Life and Earth Sciences, University of Rajshahi, Rajshahi-6205, Bangladesh E-mail: [email protected], [email protected], [email protected] Phone: 880 721 751485, Mobile: 88 01714657224 Article History Received: 29 November 2017 Accepted: 2 January 2018 Published: 1 February 2018 Citation Mst. Mafroja Khatun, Mahbubur Rahman AHM. Medicinal plants used by the local people at the village Pania under Baghmara Upazila of Rajshahi District, Bangladesh. Discovery, 2018, 54(266), 60-71 Publication License This work is licensed under a Creative Commons Attribution 4.0 International License. General Note Article is recommended to print as color digital version in recycled paper. Save trees, save nature ABSTRACT 6060 60 Medicinal plants used by the local people at the village Pania under Baghmara upazila of Rajshahi district, Bangladesh was carried out from December 2016 to November 2017. A total of 56 species belonging to 52 genera under 39 families were recorded. PagePage Page © 2018 Discovery Publication. All Rights Reserved. www.discoveryjournals.org OPEN ACCESS ANALYSIS ARTICLE Magnoliopsida is represented by 33 family, 46 genera and 49 species and Liliopsida is represented by 6 family 6 genera and 7 species. For each species botanical name, local name, habit, parts used, ailments, treatment process and family were provided. -
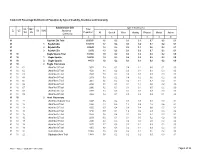
Table C-09: Percentage Distribution of Population by Type of Disability, Residence and Community
Table C-09: Percentage Distribution of Population by Type of disability, Residence and Community Administrative Unit Type of disability (%) UN / MZ / Total ZL UZ Vill RMO Residence WA MH Population All Speech Vision Hearing Physical Mental Autism Community 1 2 3 4 5 6 7 8 9 10 81 Rajshahi Zila Total 2595197 1.6 0.2 0.3 0.1 0.7 0.2 0.1 81 1 Rajshahi Zila 1740578 1.7 0.2 0.3 0.2 0.7 0.2 0.1 81 2 Rajshahi Zila 830649 1.3 0.2 0.2 0.1 0.6 0.2 0.1 81 3 Rajshahi Zila 23970 1.5 0.2 0.3 0.2 0.7 0.2 0.1 81 10 Bagha Upazila Total 184183 1.9 0.2 0.4 0.2 0.8 0.2 0.0 81 10 1 Bagha Upazila 140010 1.9 0.2 0.4 0.2 0.8 0.2 0.0 81 10 2 Bagha Upazila 44173 1.8 0.2 0.3 0.1 0.9 0.2 0.0 81 10 2 Bagha Paurashava 81 10 01 Ward No-01 Total 3973 1.3 0.2 0.4 0.1 0.6 0.1 0.0 81 10 02 Ward No-02 Total 4532 1.1 0.2 0.0 0.1 0.4 0.3 0.0 81 10 03 Ward No-03 Total 2647 2.0 0.2 0.6 0.0 0.9 0.3 0.0 81 10 04 Ward No-04 Total 2653 1.6 0.2 0.4 0.2 0.6 0.2 0.0 81 10 05 Ward No-05 Total 2661 1.5 0.2 0.2 0.1 0.7 0.2 0.1 81 10 06 Ward No-06 Total 2746 1.1 0.1 0.1 0.1 0.6 0.2 0.0 81 10 07 Ward No-07 Total 2906 1.2 0.1 0.3 0.1 0.5 0.2 0.0 81 10 08 Ward No-08 Total 2203 1.3 0.3 0.2 0.0 0.7 0.0 0.0 81 10 09 Ward No-09 Total 3302 1.3 0.1 0.0 0.2 0.9 0.1 0.0 81 10 2 Arani Paurashava 81 10 11 Ward No-01 (Arani) Total 1448 1.6 0.2 0.3 0.3 0.3 0.3 0.1 81 10 12 Ward No-02 Total 1368 4.4 0.3 1.3 0.9 1.2 0.6 0.1 81 10 13 Ward No-03 Total 1050 3.0 0.4 0.8 0.4 0.8 0.5 0.2 81 10 14 Ward No-04 Total 1718 5.9 0.1 1.4 0.6 2.9 0.8 0.2 81 10 15 Ward No-05 Total 1558 1.3 0.4 0.1 0.0 0.7 0.0 0.1 81 10 -

Survey on Major Diseases of Vegetable and Fruit Crops in Chittagong Region
ISSN 0258-7122 Bangladesh J. Agril. Res. 35(3) : 423-429, September 2010 SURVEY ON MAJOR DISEASES OF VEGETABLE AND FRUIT CROPS IN CHITTAGONG REGION M. T. HOSSAIN1, S. M. M. HOSSAIN2, M. A. BAKR3 A. K. M. MATIAR RAHMAN4 AND S. N. UDDIN5 Abstract A survey was conducted during October 2006 to June 2008 to observe disease prevalence of vegetable and fruit crops in Chittagong region. Through the survey, 24 diseases with their incidence and severity were recorded. The average higher leaf infection in early blight of potato and fruit infection in soft rot of potato were recorded 37% and 39%, respectively. The highest leaf infection (43%) of early blight of tomato that was more frequented (mode) 36% in different locations with ±0.45% ranges (Standard error) for causing the disease as recorded at Sadar Anwara upazila of Chittagong. The highest fruit infection of soft rot of potato (43%) was recorded at Dohazari, Chandanaish upazila in Chittagong. The average of higher disease severity of leaf (27%) and fruit (33%) was recorded in early blight of tomato and soft rot of potato, respectively, and the highest disease severity of leaf (29%) and fruit (35%) was recorded in Phomopsis blight and early blight of tomato and soft rot of potato, respectively. Keywords : Diseases, vegetable, fruit, survey. Introduction Bangladesh is an agrarian country. Its economy is mainly dependent on agriculture. Crop loss owing to the diseases poses a great threat to Bangladesh agriculture. More than 454 diseases in around 100 cultivated crops have so far been recorded in Bangladesh (Anon., 2006). The diseases cause substantial losses to crops. -

Social Monitoring Report BAN: South Asia Subregional Economic Cooperation Chittagong-Cox's Bazar Railway Project, Phase 1
Social Monitoring Report Semiannual Report (July–December 2019) January 2020 BAN: South Asia Subregional Economic Cooperation Chittagong-Cox's Bazar Railway Project, Phase 1 - Tranche 1 Construction of Single Line Dual Gauge Railway Track from Dohazari to Cox’s Bazar via Ramu and Ramu to Gundum Near Myanmar Prepared by Bangladesh Railway, for the Government of the People’s Republic of Bangladesh and the Asian Development Bank. This social monitoring report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. GOVERNMENT OF THE PEOPLE’S REPUBLIC OF BANGLADESH MINISTRY OF RAILWAYS BANGLADESH RAILWAY SASEC: Chittagong - Cox’s Bazar Railway Project, Phase-1 Construction of Single Line Dual Gauge Railway Track from Dohazari to Cox’s Bazar via Ramu and Ramu to Gundum Near Myanmar Social Monitoring Report (SMR) (July 2019 to December 2019) January 2020 SASEC: Chittagong – Co’s Bazar Railwa Project, Phase-1 Abbreviation ADB : Asian Development Bank AH : Affected Household AP : Affected Person APD : Additional Project Director BR : Bangladesh Railway COI : Corridor of Impact CPR : Common Property Resources CCL : Cash Compensation -

Prevalence and Antimicrobial Susceptibility Profiles of Non- Typhoidal Salmonella Isolated from Chickens in Rajshahi, Bangladesh
DOI: 10.1002/vms3.440 ORIGINAL ARTICLE Prevalence and antimicrobial susceptibility profiles of non- typhoidal Salmonella isolated from chickens in Rajshahi, Bangladesh Bindu R. Sarker1 | Sumon Ghosh2 | Sukanta Chowdhury2 | Avijit Dutta3 | Liton Chandra Deb4 | Bidhan Krishna Sarker2 | Tania Sultana1 | Khandoker Mohammad Mozaffor Hossain1 1Department of Veterinary and Animal Sciences, Faculty of Agriculture, University Abstract of Rajshahi, Rajshahi, Bangladesh Salmonellosis in poultry is an important disease that seriously impedes the development 2 Infectious Diseases Division, International of the poultry industry. The increased resistance to antimicrobials against Salmonella has Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Dhaka, Bangladesh been a major public health concern worldwide. We conducted a study from January to 3Chittagong Veterinary and Animal Sciences June 2016 in and around the Rajshahi district of Bangladesh on the commercial chicken University, Chittagong, Bangladesh to isolate, identify and characterize poultry- specific Salmonella, to assess the potential 4Department of Public Health, North Dakota State University, Fargo, ND, USA risk factors and to determine the antimicrobial resistance pattern of the isolates. The overall prevalence of Salmonella enterica was 41% (49/120) [95% CI: 31.95%– 50.17%] Correspondence Sumon Ghosh, International Centre for with 41.7% in broiler chicken (25/60) [95% CI: 29.06%– 55.12%] and 40% in layer chicken Diarrhoeal Disease Research, ICDDR,b, (24/60, 40%) [95% CI: 27.56%– 53.46%]. Samples collected from Rajshahi city (OR = 1.37, Mohakhali, Dhaka 1212, Bangladesh. Email:[email protected] 95% CI: 0.50– 3.73) and Puthia Upazila (OR = 1.51, 95% CI: 0.56– 4.12) were more likely to be positive for Salmonella than Charghat Upazila. -

Bangladesh Municipal Water Supply and Sanitation Project (BMWSSP) Public Disclosure Authorized
Bangladesh Municipal Water Supply and Sanitation Project (BMWSSP) Public Disclosure Authorized Environmental Management Framework (EMF) Public Disclosure Authorized Final Report July 2018 Public Disclosure Authorized Department of Public Health Engineering (DPHE) Ministry of Local Government, Rural Development and Cooperatives Government of the People's Republic of Bangladesh Public Disclosure Authorized . The Environmental Management Framework (EMF) for the Bangladesh Municipal Water Supply and Sanitation Project (BMWSSP) has been prepared by Bureau of Research, Testing and Consultation (BRTC). Bangladesh University of Engineering and Technology (BUET), Dhaka b TABLE OF CONTENTS Executive Summary .................................................................................................................. iv 1.0 Introduction .................................................................................................................. 1 1.1 Background ................................................................................................................... 1 1.2 WB Safeguard Policies and Basis of the EMF ................................................................ 2 1.3 Specific Objectives of EMF ............................................................................................ 4 1.4 Overall Structure of the EMF ........................................................................................ 5 2.0 Policy Legal and Administrative Framework .............................................................. -

Pre-Feasibility Study Report Natore Economic Zone
Bangladesh Economic Zones Authority Pre-feasibility Study Report Natore Economic Zone Prepared By: Infrastructure Investment Facilitation Company Sub-consultants: BETS Consulting Services Ltd. Shahidul Consultants 24 December 2018 Pre-feasibility Study Report Natore Economic Zone 24 December 2018 Prefeasibility Study of Natore Economic Zone Table of Contents EXECUTIVE SUMMARY ...................................................................................................7 1 INTRODUCTION .................................................................................................... 14 1.1 Bangladesh Economy .............................................................................................. 14 1.2 Vision 2021 ............................................................................................................. 15 1.3 Labor Force ............................................................................................................. 16 1.4 Industrial Zone Regime ........................................................................................... 16 2 APPROACH AND METHODOLOGY ........................................................................ 18 2.1 The Assignment....................................................................................................... 18 2.2 Approach................................................................................................................. 18 2.3 Component 1: Competitive and Comparative Advantage ....................................... 18 2.4 Component -

Department of Sociology University of Dhaka Dhaka University Institutional Repository
THE NATURE AND EXTENT OF HOMICIDE IN BANGLADESH: A CONTENT ANALYSIS ON REPORTS OF MURDER IN DAILY NEWSPAPERS T. M. Abdullah-Al-Fuad June 2016 Department of Sociology University of Dhaka Dhaka University Institutional Repository THE NATURE AND EXTENT OF HOMICIDE IN BANGLADESH: A CONTENT ANALYSIS ON REPORTS OF MURDER IN DAILY NEWSPAPERS T. M. Abdullah-Al-Fuad Reg no. 111 Session: 2011-2012 Submitted in partial fulfillment of the requirements of the degree of Master of Philosophy June 2016 Department of Sociology University of Dhaka Dhaka University Institutional Repository DEDICATION To my parents and sister Dhaka University Institutional Repository Abstract As homicide is one of the most comparable and accurate indicators for measuring violence, the aim of this study is to improve understanding of criminal violence by providing a wealth of information about where homicide occurs and what is the current nature and trend, what are the socio-demographic characteristics of homicide offender and its victim, about who is most at risk, why they are at risk, what are the relationship between victim and offender and exactly how their lives are taken from them. Additionally, homicide patterns over time shed light on regional differences, especially when looking at long-term trends. The connection between violence, security and development, within the broader context of the rule of law, is an important factor to be considered. Since its impact goes beyond the loss of human life and can create a climate of fear and uncertainty, intentional homicide (and violent crime) is a threat to the population. Homicide data can therefore play an important role in monitoring security and justice. -

Inventory of LGED Road Network, March 2005, Bangladesh
BASIC INFORMATION OF ROAD DIVISION : RAJSHAHI DISTRICT : RAJSHAHI ROAD ROAD NAME CREST TOTAL SURFACE TYPE-WISE BREAKE-UP (Km) STRUCTURE EXISTING GAP CODE WIDTH LENGTH (m) (Km) EARTHEN FLEXIBLE BRICK RIGID NUMBER SPAN NUMBER SPAN PAVEMENT PAVEMENT PAVEMEN (m) (m) (BC) (WBM/HBB/ T BFS) (CC/RCC) 1 2 3 4 5 6 7 8 9 10 11 12 UPAZILA : CHARGHAT ROAD TYPE : UPAZILA ROAD 181252001 Charghat - Puthia via Nandangachi GCCR 7.32 12.900.00 12.90 0.00 0.00 20 57.50 0 0.00 181252002 Arani - Puthia 7.32 7.350.00 7.35 0.00 0.00 8 119.00 0 0.00 181252003 Charghat - Dakra hat 7.32 10.850.00 10.85 0.00 0.00 19 36.00 0 0.00 181252004 Nandangachi - Dakra Via Fultolaghat GCCR 7.32 8.108.10 0.00 0.00 0.00 13 113.62 0 0.00 181252005 Kakramari to Dakra 7.32 9.854.93 4.93 0.00 0.00 20 29.52 0 0.00 181252006 Nandangachi - Arani 7.32 8.503.00 5.50 0.00 0.00 8 18.60 0 0.00 181252007 Nandagachi - Paitkhali. 5.00 3.753.75 0.00 0.00 0.00 2 4.00 0 0.00 181252008 Baladiar Azizul more - Baneshor via Maria 4.80 7.905.60 2.30 0.00 0.00 4 26.00 2 7.00 181252009 Shishatala - Nandangachi 7.32 8.300.00 8.30 0.00 0.00 9 14.10 0 0.00 181252010 Holidagachi national high way to Rajshahi University 4.90 10.500.00 10.50 0.00 0.00 1 0.90 0 0.00 via Belghoria. -

Assessing Groundwater Pollution for Irrigation in Puthia Upazila, Rajshahi
Assessing groundwater pollution for irrigation in Puthia upazila, Rajshahi A. Islam and M.M. Rahman Department of Agricultural Chemistry, Bangladesh Agricultural University, Mymensingh-2202 Abstract: Groundwater samples were collected from Puthia upazila under the district of Rajshahi to determine ionic concentration as pollutant in order to classify them on the basis of their suitability for irrigation usage. Water samples were slightly alkaline (pH = 7.10- 7.24) and were not problematic for crop production. TDS of all water samples were classified as fresh water (TDS<1,000 mg L -1). EC and SAR showed medium salinity (C2) and low alkalinity (S1) hazards combinedly expressed as C2S1. EC values of the collected water samples were in medium salinity hazard and could be safely used for crops growing on soils with moderate level of permeability and leaching. SAR values were excellent in quality for irrigating soils and crops. Out of 15 water samples, 12 samples were classified as excellent and the rest 3 samples were rated as good in quality based on SSP. Waters were free from RSC and belonged to suitable in category. All water samples were hard in quality. The concentrations of HCO3, Fe, Mn, BO3, SO4, PO4 and Cl were below the toxic levels as irrigation water and might not pose threat to soil environment as pollutants. The relationship between different water quality criteria like EC, TDS, SAR, SSP, RSC and HT were established and combinations such as EC vs TDS, EC vs RSC, EC vs HT, SAR vs SSP, SSP vs RSC SSP vs HT and RSC vs HT exhibited significant positive correlation.