2012 AACR CPR Text 2.0 Layout 1 10/20/12 4:27 AM Page 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Development of a Central Nervous System Axonal Myelination Assay for High Throughput Screening Karen D
Lariosa‑Willingham et al. BMC Neurosci (2016) 17:16 DOI 10.1186/s12868-016-0250-2 BMC Neuroscience METHODOLOGY ARTICLE Open Access Development of a central nervous system axonal myelination assay for high throughput screening Karen D. Lariosa‑Willingham1,2, Elen S. Rosler1,3, Jay S. Tung1, Jason C. Dugas1,4, Tassie L. Collins1,5 and Dmitri Leonoudakis1,2* Abstract Background: Regeneration of new myelin is impaired in persistent multiple sclerosis (MS) lesions, leaving neurons unable to function properly and subject to further degeneration. Current MS therapies attempt to ameliorate auto‑ immune-mediated demyelination, but none directly promote the regeneration of lost and damaged myelin of the central nervous system (CNS). Development of new drugs that stimulate remyelination has been hampered by the inability to evaluate axonal myelination in a rapid CNS culture system. Results: We established a high throughput cell-based assay to identify compounds that promote myelination. Culture methods were developed for initiating myelination in vitro using primary embryonic rat cortical cells. We developed an immunofluorescent phenotypic image analysis method to quantify the morphological alignment of myelin characteristic of the initiation of myelination. Using γ-secretase inhibitors as promoters of myelination, the optimal growth, time course and compound treatment conditions were established in a 96 well plate format. We have characterized the cortical myelination assay by evaluating the cellular composition of the cultures and expres‑ sion of markers of differentiation over the time course of the assay. We have validated the assay scalability and consist‑ ency by screening the NIH clinical collection library of 727 compounds and identified ten compounds that promote myelination. -

Title 16. Crimes and Offenses Chapter 13. Controlled Substances Article 1
TITLE 16. CRIMES AND OFFENSES CHAPTER 13. CONTROLLED SUBSTANCES ARTICLE 1. GENERAL PROVISIONS § 16-13-1. Drug related objects (a) As used in this Code section, the term: (1) "Controlled substance" shall have the same meaning as defined in Article 2 of this chapter, relating to controlled substances. For the purposes of this Code section, the term "controlled substance" shall include marijuana as defined by paragraph (16) of Code Section 16-13-21. (2) "Dangerous drug" shall have the same meaning as defined in Article 3 of this chapter, relating to dangerous drugs. (3) "Drug related object" means any machine, instrument, tool, equipment, contrivance, or device which an average person would reasonably conclude is intended to be used for one or more of the following purposes: (A) To introduce into the human body any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (B) To enhance the effect on the human body of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (C) To conceal any quantity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; or (D) To test the strength, effectiveness, or purity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state. (4) "Knowingly" means having general knowledge that a machine, instrument, tool, item of equipment, contrivance, or device is a drug related object or having reasonable grounds to believe that any such object is or may, to an average person, appear to be a drug related object. -

October 2004
Myelin Repair Foundation Research Progress Summary October 2004 This summary outlines progress made by the Myelin Repair Foundation research team since June 2004 and includes findings from on-going research funded by other sources that members of the team found relevant to MRF research plan. Since the success of MRF is dependent on collaboration, rather than reporting on the progress of individual projects, this report describes progress towards MRF’s overall research goals and the contributions of various team members towards completing our understanding of critical aspects of myelination and how it is affected by the multiple sclerosis (MS) disease process. 1. Fundamental control of myelination: There are several MRF investigations focused on understanding the processes that control both myelination in development and remyelination after myelin loss due to inflammation and cell death: • Dr. Ben Barres’ lab has screened thousands of genes and identified 46 genes, specific to the myelination process, that show significantly higher or lower activity levels during developmental myelination than before or after the myelination process. In addition, Dr. Barres’ lab has demonstrated the timing of these changes during the developmental myelination process. The next step is to analyze the function of each of these 46 genes by artificially controlling its level of activity (expression) and observing the effect it has on myelin formation. Finding ways to artificially manipulate the expression of each gene is a formidable task. Although the functional analysis of each gene in this group is a significant project that may take several years to complete because of the large number of genes to be analyzed, the initial identification of these active genes is providing clues to other MRF researchers that will help prioritize which genes to evaluate first and which to ignore. -

Pharmaceuticals As Environmental Contaminants
PharmaceuticalsPharmaceuticals asas EnvironmentalEnvironmental Contaminants:Contaminants: anan OverviewOverview ofof thethe ScienceScience Christian G. Daughton, Ph.D. Chief, Environmental Chemistry Branch Environmental Sciences Division National Exposure Research Laboratory Office of Research and Development Environmental Protection Agency Las Vegas, Nevada 89119 [email protected] Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada Why and how do drugs contaminate the environment? What might it all mean? How do we prevent it? Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada This talk presents only a cursory overview of some of the many science issues surrounding the topic of pharmaceuticals as environmental contaminants Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada A Clarification We sometimes loosely (but incorrectly) refer to drugs, medicines, medications, or pharmaceuticals as being the substances that contaminant the environment. The actual environmental contaminants, however, are the active pharmaceutical ingredients – APIs. These terms are all often used interchangeably Office of Research and Development National Exposure Research Laboratory, Environmental Sciences Division, Las Vegas, Nevada Office of Research and Development Available: http://www.epa.gov/nerlesd1/chemistry/pharma/image/drawing.pdfNational -

Photodynamic Therapy for the Treatment of Actinic Keratoses and Other Skin Lesions
Photodynamic Therapy for the Treatment of Actinic Keratoses and Other Skin Lesions Policy Number: Current Effective Date: MM.02.016 March 22, 2019 Lines of Business: Original Effective Date: HMO; PPO; QUEST Integration April 01, 2008 Place of Service: Precertification: Office Not Required I. Description Photodynamic therapy (PDT) refers to light activation of a photosensitizer to generate highly reactive intermediaries, which ultimately cause tissue injury and necrosis. Photosensitizing agents are being proposed for use with dermatologic conditions such as actinic keratoses and nonmelanoma skin cancers.For individuals who have nonhyperkeratotic actinic keratoses on the face or scalp who receive PDT, the evidence includes randomized controlled trials (RCTs). The relevant outcomes are symptoms, change in disease status, quality of life, and treatment-related morbidity. Evidence from multiple RCTs has found that PDT improves the net health outcome in patients with nonhyperkeratotic actinic keratoses on the face or scalp compared with placebo or other active interventions. The evidence is sufficient to determine that the technology results in a meaningful improvement in the net health outcome. For individuals who have low-risk basal cell carcinoma who receive PDT, the evidence includes RCTs and systematic reviews of RCTs. The relevant outcomes are symptoms, change in disease status, quality of life, and treatment-related morbidity. Systematic reviews of RCTs have found that PDT may not be as effective as surgery for superficial and nodular basal cell carcinoma. In the small number of trials available, PDT was more effective than placebo. The available evidence from RCTs has suggested that PDT has better cosmetic outcomes than surgery. -
Wo 2010/068920 A2
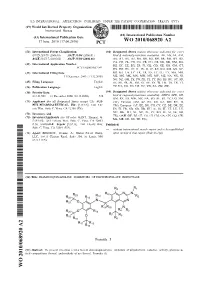
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date 17 June 2010 (17.06.2010) WO 2010/068920 A2 (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every C07D 239/78 (2006.01) A61P 31/04 (2006.01) kind of national protection available): AE, AG, AL, AM, A61K 31/51 7 (2006.01) A61P 35/00 (2006.01) AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, (21) Number: International Application DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, PCT/US2009/067749 HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, (22) International Filing Date: KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, 11 December 2009 ( 11.12.2009) ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, PE, PG, PH, PL, PT, RO, RS, RU, SC, SD, (25) Filing Language: English SE, SG, SK, SL, SM, ST, SV, SY, TJ, TM, TN, TR, TT, (26) Publication Language: English TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (30) Priority Data: (84) Designated States (unless otherwise indicated, for every 61/121,965 12 December 2008 (12.12.2008) US kind of regional protection available): ARIPO (BW, GH, GM, KE, LS, MW, MZ, NA, SD, SL, SZ, TZ, UG, ZM, (71) Applicant (for all designated States except US): AUS- ZW), Eurasian (AM, AZ, BY, KG, KZ, MD, RU, TJ, PEX PHARMACEUTICAL, INC. -

MRF Archive Compiled Research Summaries
Myelin Repair Foundation Archived Research Summaries Summaries – 2008 Bailey, S. L., B. Schreiner, and S. D. Miller. 2008. CNS dendritic cells in inflammation and disease. In: Central Nervous System Diseases and Inflammation. (T. E. Lane, M. Carson, C. Bergmann and T. Wyss-Coray, eds.). Springer, New York, NY. Pp 263-275. http://www.springerlink.com/content/l17910144487u803/ Scientific Summary: CD11c+ DCs play a major role in both the initiation and progression of autoimmune inflammatory disease in the CNS. Since the CNS serves as the primary site where activation of pathogenic Th1/Th17 cells specific for endogenous myelin epitopes (i.e., epitope spreading), which play a critical role in driving progressive autoimmune disease, the current data suggests that the inflamed CNS can function as a neo-lymphoid organ. In support of this our recent unpublished data indicates that expression of genes encoding multiple receptor:ligand pairs involved in lymphoid organogenesis (including LTα1β2/LTβR, CXCL12/CXCR4, CSCL13/CXCR5, CCL21/CCR7, and CCL19/CCR7) are highly upregulated in the CNS. Further, mDCs are the main drivers of epitope spreading displaying the unique ability to acquire and present endogenous myelin peptides, to cluster specifically with naïve CD4+ T cells in the inflamed CNS and to polarize towards a Th17 phenotype when presenting endogenous myelin peptides. In conclusion, understanding the cues that determine DC signals to T cells will be crucial to understanding the fate of pathological (auto)immune inflammation in different tissues and diseases. Moreover, strategies targeting inhibition of the migration of myeloid DCs to the CNS may be an effective therapy for chronic immune-mediated CNS demyelinating diseases including MS. -

Cerebellar Syndrome in a Man Treated with Natalizumab from the National Multiple Sclerosis Society Case Conference Proceedings
DIAGNOSTIC AND TREATMENT CHALLENGES OPEN ACCESS Cerebellar syndrome in a man treated with natalizumab From the National Multiple Sclerosis Society Case Conference Proceedings David A. Lapides, MD, Prem P. Batchala, MD, Joseph H. Donahue, MD, Robert P. Lisak, MD,* Correspondence Ethan I. Meltzer, MD,§* Ram N. Narayan, MD,* Avi Nath, MD, PhD,* Teresa C. Frohman, MPAS, MSCSPA-C,‡* Dr. Goldman [email protected] ‡ † Kathleen Costello, MS, ANP-BC, * Myla D. Goldman, MD, MSc, Scott S. Zamvil, MD, PhD,* and or Dr. Zamvil Elliot M. Frohman, MD, PhD*† [email protected] or Dr. Frohman Neurol Neuroimmunol Neuroinflamm 2019;6:e546. doi:10.1212/NXI.0000000000000546 [email protected] A 57-year-old man with a medical history significant for bipolar disorder, depression, and anxiety presented in 2010 with bilateral lower extremity numbness progressing to perineal numbness and urinary retention. A “working” diagnosis of relapsing-remitting MS (RRMS) was supported by disseminated T2 hyperintensities on MRI investigations of the brain and spinal cord. Furthermore, CSF analysis revealed 4 unique oligoclonal bands not identified in blood. Initial treatment with IM interferon beta-1a exacerbated the patient’s depression, prompting discontinuation after only 6 weeks of injection therapy. He was then transitioned to daily subcutaneous glatiramer acetate, which was well tolerated and resulted in disease stabilization for approximately 12 months. He had a relapse in 2011 with symptoms corresponding to a new enhancing lesion in the thoracic spinal cord. The pronounced MS disease burden in the spinal cord, in conjunction with breakthrough disease activity while on glatiramer acetate, prompted the treating team to recommend in- tensification of disease-modifying therapy with natalizumab, which was administered IV every 4 weeks from 2011 to 2014 for a total of 33 treatments. -
Aacr Cancer Progress Report
AACR CANCER PROGRESS REPORT CANCER PROGRESS AACR 615 Chestnut Street, 17th Floor, Philadelphia, PA 19106-4404 2017 AACR CANCER PROGRESS REPORT 2017 Harnessing Research Discoveries to Save Lives AACR.org CancerProgressReport.org #CancerProgress17 For your FREE copy of the full report, go to www.CancerProgressReport.org AACR CANCER PROGRESS REPORT 2017 Harnessing Research Discoveries to Save Lives AACR.org CancerProgressReport.org #CancerProgress17 Please cite this report as: cancerprogressreport.org [Internet]. Philadelphia: American Association for Cancer Research; ©2017 [cited year month date]. Available from http://www.cancerprogressreport.org/. HARNESSING RESEARCH TABLE OF DISCOVERIES TO SAVE LIVES 48 Biomedical Research 48 CONTENTS Progress across the Clinical Cancer Care Continuum 54 Cancer Prevention, Detection, and Diagnosis 54 Simplifying the HPV Vaccination Schedule 54 Enhancing Cancer Detection AACR CANCER PROGRESS and Diagnosis with Technology 54 REPORT 2017 STEERING COMMITTEE iii Treatment with Surgery, Radiotherapy, and Cytotoxic Chemotherapy 56 AACR STAFF iv Improving Outcomes by Combining Existing Treatments 56 Reducing the Adverse Effects of Surgery 56 A MESSAGE FROM THE AACR 1 Tailoring Radiotherapy: Less Is Sometimes More 57 EXECUTIVE SUMMARY 3 Treatment with Molecularly Targeted Therapeutics 57 Cancer in 2017 3 Adding Precision to Treatment for Acute Myeloid Leukemia 61 Targeting Soft Tissue Sarcoma 62 Preventing Cancer: Understanding Risk Factors 4 Increasing Options for Patients with Ovarian Cancer 64 Screening for -

2.01.44 Dermatologic Applications of Photodynamic Therapy
Medical Policy 2.01.44 Dermatologic Applications of Photodynamic Therapy Original Policy Date: June 1, 2001 Effective Date: February 1, 2021 Section: 2.0 Medicine Page: Page 1 of 30 Policy Statement Photodynamic therapy may be considered medically necessary as a treatment of any of the following: I. Nonhyperkeratotic actinic keratoses of the face and scalp (see policy guidelines) II. Nonhyperkeratotic actinic keratoses of the upper extremities (see policy guidelines) III. Low-risk (e.g., superficial and nodular) basal cell skin cancer only when surgery and radiation are contraindicated IV. Cutaneous squamous cell carcinoma in situ (Bowen disease) only when surgery and radiation are contraindicated Photodynamic therapy is considered investigational for other dermatologic applications, including, but not limited to: I. Acne vulgaris II. Hidradenitis suppurativa III. High-risk basal cell carcinomas IV. Mycoses Photodynamic therapy is considered not medically necessary as a technique of any of the following: I. Altering normal structures of the body in order to improve appearance II. Hair removal III. Skin rejuvenation NOTE: Refer to Appendix A to see the policy statement changes (if any) from the previous version. Policy Guidelines Surgery and radiation are the preferred treatments for low-risk basal cell cancer and Bowen disease (see Rationale section). If photodynamic therapy is selected for these indications because of contraindications to surgery or radiation, patients and physicians need to be aware that it may have a lower cure rate than surgery or radiation. Photodynamic therapy typically involves 2 office visits: 1 to apply the topical aminolevulinic acid and a second visit to expose the patient to blue light. -

Axonal and Myelin Neuroprotection by the Peptoid BN201 in Brain Inflammation
Neurotherapeutics https://doi.org/10.1007/s13311-019-00717-4 ORIGINAL ARTICLE Axonal and Myelin Neuroprotection by the Peptoid BN201 in Brain Inflammation Pablo Villoslada 1 & Gemma Vila 1 & Valeria Colafrancesco 1 & Beatriz Moreno 1 & Begoña Fernandez-Diez 1 & Raquel Vazquez 1 & Inna Pertsovskaya 1 & Irati Zubizarreta 1 & Irene Pulido-Valdeolivas 1 & Joaquin Messeguer 2 & Gloria Vendrell-Navarro 2 & Jose Maria Frade 3 & Noelia López-Sánchez 3 & Meritxell Teixido 4 & Ernest Giralt 4 & Mar Masso 5 & Jason C Dugas 6 & Dmitri Leonoudakis 6 & Karen D. Lariosa-Willingham 6 & Lawrence Steinman 7 & Angel Messeguer 2 # The American Society for Experimental NeuroTherapeutics, Inc. 2019 Abstract The development of neuroprotective therapies is a sought-after goal. By screening combinatorial chemical libraries using in vitro assays, we identified the small molecule BN201 that promotes the survival of cultured neural cells when subjected to oxidative stress or when deprived of trophic factors. Moreover, BN201 promotes neuronal differentiation, the differentiation of precursor cells to mature oligodendrocytes in vitro , and the myelination of new axons. BN201 modulates several kinases participating in the insulin growth factor 1 pathway including serum –glucocorticoid kinase and midkine, inducing the phosphorylation of NDRG1 and the translocation of the transcription factor Foxo3 to the cytoplasm. In vivo , BN201 prevents axonal and neuronal loss, and it promotes remyelination in models of multiple sclerosis, chemically induced demyelination, and glaucoma. -

Neurimminfl2015006502 1..11
Glatiramer acetate treatment negatively regulates type I interferon signaling Nicolas Molnarfi, PhD* ABSTRACT ’ Thomas Prod homme, Objective: Glatiramer acetate (GA; Copaxone), a disease-modifying therapy for multiple sclerosis (MS), PhD* promotes development of anti-inflammatory (M2, type II) monocytes that can direct differentiation of Ulf Schulze-Topphoff, regulatory T cells. We investigated the innate immune signaling pathways that participate in GA- PhD mediated M2 monocyte polarization. Collin M. Spencer, BS Methods: Monocytes were isolated from myeloid differentiation primary response gene 88 (MyD88)– Martin S. Weber, MD deficient, Toll-IL-1 receptor domain–containing adaptor inducing interferon (IFN)–b (TRIF)–deficient, IFN-a/b Juan C. Patarroyo, BS receptor subunit 1 (IFNAR1)–deficient, and wild-type (WT) mice and human peripheral blood. GA-treated Patrice H. Lalive, MD monocytes were stimulated with Toll-like receptor ligands, then evaluated for activation of kinases and Scott S. Zamvil, MD, transcription factors involved in innate immunity, and secretion of proinflammatory cytokines. GA-treated PhD mice were evaluated for cytokine secretion and susceptibility to experimental autoimmune encephalomyelitis. Results: GA-mediated inhibition of proinflammatory cytokine production by monocytes occurred inde- pendently of MyD88 and nuclear factor–kB, but was blocked by TRIF deficiency. Furthermore, GA did Correspondence to Dr. Zamvil: not provide clinical benefit in TRIF-deficient mice. GA inhibited activation of p38 mitogen-activated [email protected] protein kinase, an upstream regulator of activating transcription factor (ATF)–2, and c-Jun N-terminal kinase 1, which regulates IFN regulatory factor 3 (IRF3). Consequently, nuclear translocation of ATF-2 and IRF3, components of the IFN-b enhanceosome, was impaired.