Resuscitative Thoracotomy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Rare Case of Penetrating Trauma of Frontal Sinus with Anterior Table Fracture Himanshu Raval1*, Mona Bhatt2 and Nihar Gaur3
ISSN: 2643-4474 Raval et al. Neurosurg Cases Rev 2020, 3:046 DOI: 10.23937/2643-4474/1710046 Volume 3 | Issue 2 Neurosurgery - Cases and Reviews Open Access CASE REPORT Case Report: A Rare Case of Penetrating Trauma of Frontal Sinus with Anterior Table Fracture Himanshu Raval1*, Mona Bhatt2 and Nihar Gaur3 1 Department of Neurosurgery, NHL Municipal Medical College, SVP Hospital Campus, Gujarat, India Check for updates 2Medical Officer, CHC Dolasa, Gujarat, India 3GAIMS-GK General Hospital, Gujarat, India *Corresponding author: Dr. Himanshu Raval, Resident, Department of Neurosurgery, NHL Municipal Medical College, SVP Hospital Campus, Elisbridge, Ahmedabad, Gujarat, 380006, India, Tel: 942-955-3329 Abstract Introduction Background: Head injury is common component of any Road traffic accident (RTA) is the most common road traffic accident injury. Injury involving only frontal sinus cause of cranio-facial injury and involvement of frontal is uncommon and unique as its management algorithm is bone fractures are rare and constitute 5-9% of only fa- changing over time with development of radiological modal- ities as well as endoscopic intervention. Frontal sinus inju- cial trauma. The degree of association has been report- ries may range from isolated anterior table fractures causing ed to be 95% with fractures of the anterior table or wall a simple aesthetic deformity to complex fractures involving of the frontal sinuses, 60% with the orbital rims, and the frontal recess, orbits, skull base, and intracranial con- 60% with complex injuries of the naso-orbital-ethmoid tents. Only anterior table injury of frontal sinus is rare in pen- region, 33% with other orbital wall fractures and 27% etrating head injury without underlying brain injury with his- tory of unconsciousness and questionable convulsion which with Le Fort level fractures. -

Traumatic Intracranial Aneurysms Due to Penetrating Brain Injury. a Case Report and Suggested Management Guidelines Breck Aaron Jones MD; Alex Patrick Michael MD
Traumatic Intracranial Aneurysms Due to Penetrating Brain Injury. A Case Report and Suggested Management Guidelines Breck Aaron Jones MD; Alex Patrick Michael MD Southern Illinois University School of Medicine Methods Learning Objectives Introduction Angiogram Traumatic intracranial aneurysms A Pubmed search of the literature Identification of traumatic intracranial pertaining to traumatic aneurysms. (TICA) are rare in occurrence and pseudoaneurysms and penetrating Classification of traumatic intracranial equally rare in the literature. Less brain trauma. The literature was aneurysms. than 1% of intracranial aneurysms reviewed for case reports and Treatment and management of are caused by blunt trauma, while management recommendations. traumatic intracranial aneurysms. even fewer are caused by penetrating trauma. Penetrating Results References Traumatic intracranial aneurysm 1.Aarabi B. Management of traumatic aneurysms caused by trauma creates a unique type of high-velocity missile head wounds. Neurosurg Clin N Am. formation is the most commonly aneurysm that does not incorporate Oct 1995;6(4):775-797. described vascular injury after 2.Rao GP, Rao NS, Reddy PK. Technique of removal of an all three vessel wall layers. Because penetrating brain injury. impacted sharp object in a penetrating head injury using the of their rarity, the natural history and Histologically, traumatic aneurysms lever principle. Br J Neurosurg. Dec 1998;12(6):569-571. 3.Vascular complications of penetrating brain injury. J can be described as true management of TICAs are not well Trauma. Aug 2001;51(2 Suppl):S26-28. Angiogram showing traumatic intracranial (incorporating intima, media, defined in the literature. Here we 4.Crompton MR. The pathogenesis of cerebral aneurysms. aneurysm following a gunshot wound to adventitia), false (incorporating one or Brain. -

Prehospital Spine Immobilization for Penetrating Trauma—Review and Recommendations from the Prehospital Trauma Life Support Executive Committee
REVIEW ARTICLE Prehospital Spine Immobilization for Penetrating Trauma—Review and Recommendations From the Prehospital Trauma Life Support Executive Committee Lance E. Stuke, MD, MPH, Peter T. Pons, MD, Jeffrey S. Guy, MD, MSc, MMHC, Will P. Chapleau, RN, EMT-P, Frank K. Butler, MD, Capt MC USN (Ret), and Norman E. McSwain, MD pine immobilization in trauma patients suspected of hav- In the case of penetrating injuries, delays in transport Sing a spinal injury has been a cornerstone of prehospital prolong the time before patients receive the prompt surgical treatment for decades. Current practices are based on the care needed to arrest hemorrhage. Even with experienced belief that a patient with an injured spinal column can prehospital providers, spine immobilization is time consum- deteriorate neurologically without immobilization. Most ing. The time required for experienced emergency medical treatment protocols do not differentiate between blunt and technicians to properly immobilize a cervical spine has been penetrating mechanisms of injury. Current Emergency Med- reported to be 5.64 minutes (Ϯ1.49 minutes).6 This scene ical Service (EMS) protocols for spinal immobilization of delay can be catastrophic for a patient with penetrating penetrating trauma are based on historic practices rather than trauma requiring urgent surgical intervention for airway com- scientific merits. Although blunt spinal column injuries will promise or hemorrhage. Studies have demonstrated that cervical collars increase occasionally produce unstable vertebral -

Deaths from Abdominal Trauma: Analysis of 1888 Forensic Autopsies
DOI: 10.1590/0100-69912017006006 Original Article Deaths from abdominal trauma: analysis of 1888 forensic autopsies Óbitos por trauma abdominal: análise de 1888 autopsias médico-legais POLYANNA HELENA COELHO BORDONI1; DANIELA MAGALHÃES MOREIRA DOS SANTOS2; JAÍSA SANTANA TEIXEIRA2; LEONARDO SANTOS BORDONI2-4. ABSTRACT Objective: to evaluate the epidemiological profile of deaths due to abdominal trauma at the Forensic Medicine Institute of Belo Horizonte, MG - Brazil. Methods: we conducted a retrospective study of the reports of deaths due to abdominal trauma autopsied from 2006 to 2011. Results: we analyzed 1.888 necropsy reports related to abdominal trauma. Penetrating trauma was more common than blunt one and gun- shot wounds were more prevalent than stab wounds. Most of the individuals were male, brown-skinned, single and occupationally active. The median age was 34 years. The abdominal organs most injured in the penetrating trauma were the liver and the intestines, and in blunt trauma, the liver and the spleen. Homicide was the most prevalent circumstance of death, followed by traffic accidents, and almost half of the cases were referred to the Forensic Medicine Institute by a health unit. The blood alcohol test was positive in a third of the necropsies where it was performed. Cocaine and marijuana were the most commonly found substances in toxicology studies. Conclusion: in this sam- ple. there was a predominance of penetrating abdominal trauma in young, brown and single men, the liver being the most injured organ. Keywords: Autopsy. Forensic Medicine. Homicide. Abdominal Injuries. INTRODUCTION In addition, the accuracy of abdominal phy- sical examination is low and the level of consciousness eaths from external causes represent the second produced by hemorrhages or by the association of ab- Dleading cause of mortality in Brazil and the main dominal trauma (AT) with traumatic brain injury and/or cause when considering individuals under the age of effects of central nervous system of previously consu- 351. -

Updated Mild Traumatic Brain Injury Guideline for Adults
Heads Up to Clinicians: Updated Mild Traumatic Brain Injury Guideline for Adults This Guideline is based on the 2008 Mild TBI Clinical Policy for adults, which revises the previous 2002 Clinical Policy. To help improve diagnosis, treatment, and outcomes for patients with mild TBI, it is critical that you become familiar with this guideline. The guideline is especially important for clinicians working in hospital-based emergency care. Inclusion Criteria: This guideline is intended for patients with non-penetrating trauma to the head who present to the ED within 24 hours of injury, who have a Glascow Coma Scale (GCS) score of 14 or 15 on initial evaluation in the ED, and are ≥ 16 years old. Exclusion Criteria: This guideline is not intended for patients with penetrating trauma or multisystem trauma who have a GCS score of < 14 on initial evaluation in the ED and are < 16 years old. Please turn over. What You Need to Know: This guideline provides recommendations for determining which patients with a known or suspected mild TBI require a head CT and which may be safely discharged. Here are a few important points to note: There is no evidence to recommend the use of a head Discuss discharge instructions with patients and give MRI over a CT in acute evaluation. them a discharge instruction sheet to take home and share with their family and/or caregiver. Be sure to: A noncontrast head CT is indicated in head trauma patients with loss of consciousness or posttraumatic • Alert patients to look for postconcussive symptoms amnesia in presence of specific symptoms. -

Western Trauma Association Critical Decisions in Trauma: Penetrating Chest Trauma
WTA 2014 ALGORITHM Western Trauma Association Critical Decisions in Trauma: Penetrating chest trauma Riyad Karmy-Jones, MD, Nicholas Namias, MD, Raul Coimbra, MD, Ernest E. Moore, MD, 09/30/2020 on BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3Ypodx1mzGi19a2VIGqBjfv9YfiJtaGCC1/kUAcqLCxGtGta0WPrKjA== by http://journals.lww.com/jtrauma from Downloaded Martin Schreiber, MD, Robert McIntyre, Jr., MD, Martin Croce, MD, David H. Livingston, MD, Jason L. Sperry, MD, Ajai K. Malhotra, MD, and Walter L. Biffl, MD, Portland, Oregon Downloaded from http://journals.lww.com/jtrauma his is a recommended algorithm of the Western Trauma Historical Perspective TAssociation for the acute management of penetrating chest The precise incidence of penetrating chest injury, varies injury. Because of the paucity of recent prospective randomized depending on the urban environment and the nature of the trials on the evaluation and management of penetrating chest review. Overall, penetrating chest injuries account for 1% to injury, the current algorithms and recommendations are based 13% of trauma admissions, and acute exploration is required in by on available published cohort, observational and retrospective BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3Ypodx1mzGi19a2VIGqBjfv9YfiJtaGCC1/kUAcqLCxGtGta0WPrKjA== 5% to 15% of cases; exploration is required in 15% to 30% of studies, and the expert opinion of the Western Trauma Asso- patients who are unstable or in whom active hemorrhage is ciation members. The two algorithms should be reviewed in the suspected. Among patients managed by tube thoracostomy following sequence: Figure 1 for the management and damage- alone, complications including retained hemothorax, empy- control strategies in the unstable patient and Figure 2 for the ema, persistent air leak, and/or occult diaphragmatic injuries management and definitive repair strategies in the stable patient. -

ABC Ofmajor' Trauma ABDOMINAL TRAUMA BMJ: First Published As 10.1136/Bmj.301.6744.172 on 21 July 1990
ABC ofMajor' Trauma ABDOMINAL TRAUMA BMJ: first published as 10.1136/bmj.301.6744.172 on 21 July 1990. Downloaded from Andrew Cope, William Stebbings The aim ofthis article is to enable all those concerned with the management of patients with abdominal trauma to perform a thorough examination and assessment with the help of diagnostic tests and to institute safe and correct treatment. Intra-abdominal injuries carry a high morbidity and mortality because they are often not detected or their severity is underestimated. This is particularly common in cases of blunt trauma, in which there may be few or no external signs. Always have a high index ofsuspicion ofabdominal injury when the history suggests severe trauma. Traditionally, abdominal trauma is classified as either blunt or penetrating, but the initial assessment and, if required, resuscitation are essentially the same. Blunt trauma Road traffic accidents are one of the commonest causes of blunt injuries. Since wearing seat belts was made compulsory the number of fatal head injuries has declined, but a pattern of blunt abdominal trauma that is specific to seat belts has emerged. This often includes avulsion injuries of the mesentery of the small bowel. The symptoms and signs of blunt abdominal trauma can be subtle, and consequently diagnosis is difficult. A high degree of suspicion of underlying intra-abdominal injury must be adopted when dealing with blunt trauma. Blunt abdominal trauma is -usually associated with trauma to other areas, especially the head, chest, http://www.bmj.com/ .. , :and pelvis. Penetrating trauma Penetrating wounds are either due to low velocity projectiles such as on 1 October 2021 by guest. -
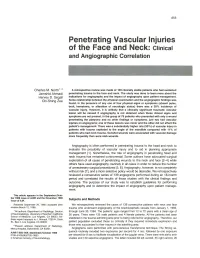
Penetrating Vascular Injuries of the Face and Neck: Clinical and Angiographic Correlation
855 Penetrating Vascular Injuries of the Face and Neck: Clinical and Angiographic Correlation Charles M. North 1. 2 A retrospective review was made of 139 clinically stable patients who had sustained Jamshid Ahmadi penetrating trauma to the face and neck. The study was done to learn more about the Hervey D. Segall indications for angiography and the impact of angiography upon patient management. Chi-Shing Zee Some relationship between the physical examination and the angiographic findings was found. In the presence of anyone of four physical signs or symptoms (absent pulse, bruit, hematoma, or alteration of neurologic status) there was a 30% incidence of vascular injury. However, it is unlikely that a clinically significant traumatic vascular lesion will be missed if angiography is not obtained when these clinical signs and symptoms are not present. In the group of 78 patients who presented with only a wound penetrating the ' platysma and no other findings or symptoms, just two had vascular injuries on angiograms; one of these lesions was minor and the other did not affect the patient's management. There was a substantially higher rate (50%) of vascular injury in patients with trauma cephalad to the angle of the mandible compared with 11 % of patients who had neck trauma. Gunshot wounds were associated with vascular damage more frequently than were stab wounds. Angiography is often performed in penetrating trauma to the head and neck to evaluate the possibility of vascular injury and to aid in planning appropriate management [1]. Nonetheless, the role of angiography in penetrating head and neck trauma has remained controversial. -

Modern Management of Traumatic Hemothorax
rauma & f T T o re l a t a m n r e u n o t J Mahoozi, et al., J Trauma Treat 2016, 5:3 Journal of Trauma & Treatment DOI: 10.4172/2167-1222.1000326 ISSN: 2167-1222 Review Article Open Access Modern Management of Traumatic Hemothorax Hamid Reza Mahoozi, Jan Volmerig and Erich Hecker* Thoraxzentrum Ruhrgebiet, Department of Thoracic Surgery, Evangelisches Krankenhaus, Herne, Germany *Corresponding author: Erich Hecker, Thoraxzentrum Ruhrgebiet, Department of Thoracic Surgery, Evangelisches Krankenhaus, Herne, Germany, Tel: 0232349892212; Fax: 0232349892229; E-mail: [email protected] Rec date: Jun 28, 2016; Acc date: Aug 17, 2016; Pub date: Aug 19, 2016 Copyright: © 2016 Mahoozi HR. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Hemothorax is defined as a bleeding into pleural cavity. Hemothorax is a frequent manifestation of blunt chest trauma. Some authors suggested a hematocrit value more than 50% for differentiation of a hemothorax from a sanguineous pleural effusion. Hemothorax is also often associated with penetrating chest injury or chest wall blunt chest wall trauma with skeletal injury. Much less common, it may be related to pleural diseases, induced iatrogenic or develop spontaneously. In the vast majority of blunt and penetrating trauma cases, hemothoraces can be managed by relatively simple means in the course of care. Keywords: Traumatic hemothorax; Internal chest wall; Cardiac Hemodynamic response injury; Clinical manifestation; Blunt chest-wall injuries; Blunt As above mentioned the hemodynamic response is a multifactorial intrathoracic injuries; Penetrating thoracic trauma response and depends on severity of hemothorax according to its classification. -

Abdominal Trauma 4/4/19, 12�41 AM
Abdominal Trauma 4/4/19, 1241 AM (/microsites/cdem) Abdominal Trauma Author: Nur-Ain Nadir. MD. Director of Medical Student Education. Core Faculty, Assistant Clinical Professor. University of Illinois College of Medicine Peoria. Editor: Nicholas E. Kman, MD FACEP Director, EM Clerkship Clinical-Associate Professor of Emergency Medicine OSU Wexner Medical Center Department of Emergency Medicine 780 Prior Hall, 376 West 10th Ave, Columbus, OH 43210 Objectives Upon completion of this module, you should be able to: https://saem.org/cdem/education/online-education/m4-curriculum/group-m4-trauma/abdominal-trama Page 1 of 9 Abdominal Trauma 4/4/19, 1241 AM 1. Diagnose, resuscitate, stabilize and manage abdominal trauma patients; 2. Identify common pathophysiologic conditions in abdominal trauma patients; 3. Describe the components of a primary survey in an abdominal trauma patient; Generate a differential diagnosis of potential traumatic injuries based on history, mechanism, and physical exam; 4. List commonly utilized imaging modalities in abdominal trauma; 5. Discuss the eventual disposition of abdominal trauma patients based on their diagnosis; 6. Appreciate the necessity for emergent surgical intervention in certain abdominal trauma conditions. Introduction Abdominal trauma is seen quite often in the Emergency Department where it can take the shape of blunt or penetrating mechanisms occasionally a combination of both. Blunt abdominal trauma (BAT) is frequently encountered in the form of motor vehicle accidents (75%), followed by falls and direct abdominal impact1. Three kinds of forces are seen with BAT: shearing forces, that occur due to rapid deceleration causing tearing at fixed points of attachments. Crushing forces, that cause intra-abdominal contents to be crushed between anterior abdominal wall and posterior ribs and vertebrae; and external compression which is the sudden and rapid rise in intra-abdominal pressure leading to rupture of viscous organs.2 Penetrating abdominal trauma (PAT) is on the rise with increasing gang violence. -

Resuscitation and Anaesthesia for Penetrating Trauma Douglas M
Resuscitation and anaesthesia for penetrating trauma Douglas M. Bowley, Simon J. Robertson, Kenneth D Boffard and Sats Bhagwanjee Purpose of review Introduction The worldwide burden of trauma is increasing, but is unequal In 1990, about five million people died worldwide as a between nations. Trauma targets the young and productive in result of injury [1] and it is estimated that by the year society and imposes a major burden on the health infrastructure. 2020, 8.4 million people will die every year from trauma This review provides a distillation of practice in a busy urban [2]. However, volumes and patterns of injury vary trauma centre dealing with large volumes of penetrating trauma. considerably around the world; overall homicide rates Recent findings range from 1.0 per 100 000 in established market The anaesthetist holds a pivotal role in the management of economies to 44.8 per 100 000 in sub-Saharan Africa penetrating injury; the requirements of prompt airway control, [3 .]. While the United States saw a nationwide decrease early delivery to theatre and control of a physiologically brittle in the annual non-fatal firearm-related injury rate of patient can be challenging. Recognition that attempts at 40.3% between 1993 and 1997, with a 21% decline in the definitive surgery in exsanguinating patients may do more harm annual firearm-related death rate during the same period than good has made surgery a tool of resuscitation rather than [4], South Africa is battling with what has been described an end in itself. as ‘a malignant epidemic of trauma’ [5]. Penetrating Summary trauma in South Africa in the 1980s was predominantly Depending on where they practice, clinicians are more or less from stab wounds; however, in recent years gunshot likely to encounter patients with gunshot wounds. -

Case Report PNEUMOTHORAX and PNEUMOPERITONEUM CAUSED by PENETRATING CHEST INJURY 2 4 K.A.B.M Talful Alam1, Md
Journal of Surgical Sciences (2018) Vol. 22(1) @ 2012 Society of Surgeons of Bangladesh JOURNAL OF SURGICAL SCIENCES Case Report PNEUMOTHORAX AND PNEUMOPERITONEUM CAUSED BY PENETRATING CHEST INJURY 2 4 K.A.B.M Talful Alam1, Md. Shah Alam Sarker , Md. Khaled Hasan3, Prawesh Maharjan Abstract Pneumothorax and pneumoperitoneum caused by penetrating chest injury are rare. Pneumo• peritoneum following trauma usually indicates the presence of a perforated intraabdominal hollow viscous. Other causes of pneumoperitoneum are through the abdominal wall, through the diaphragm, through female genital tract and through retroperitoneum. Here we report an unusual case of pneumothorax and pneumoperitoneum caused by penetrat• ing injury in the posterior aspect of chest in a young male patient of 33 years who presented to us with chest & abdominal pain & breathlessness. The diagnosis was made on clinical & radio• logical examination. Tube thoracostomy was done followed by laparotomy and repair of diaphragmatic & splenic injury. Post operative recovery was uneventful & the patient was discharged on 9th p.o.d after removal of thoracostomy tube & wound stiches. Keywords: Pneumothorax, Pneumoperitoneum, Thoracostomy,Laparotomy. Introduction of the mediastinum or change in the hemi The chest serves the important functions of respira• diaphragm. tion & of protection of the vital intrathoracic & upper Pneumoperitoneum following trauma usually abdominal organs from externally applied force and is indicates the presence of a perforated intraabdomi• composed of the rigid structure of the rib cage, nal hollow viscous and the need for laparotomy2. clavicles, sternum, scapulae & heavy overlying Other causes of pneumoperitoneum are through the musculature. Penetrating chest injuries are generally abdominal wall, through the diaphragm, through 3 less common but more deadly than blunt chest injury.