Bilateral Torus Mandibularis: a Case Report with Mini 2018; 1(1): 27-28 Received: 16-01-2018 Review Accepted: 20-02-2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
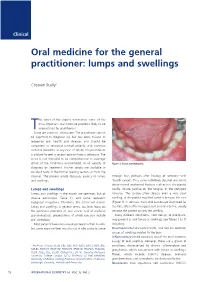
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

WHAT HAPPENED? CDR, a 24-Year-Old Chinese Male
CHILDHOOD DEVELOPMENTAL SCREENING 2020 https://doi.org/10.33591/sfp.46.5.up1 FINDING A MASS WITHIN THE ORAL CAVITY: WHAT ARE THE COMMON CAUSES AND 4-7 GAINING INSIGHT: WHAT ARE THE ISSUES? In Figure 2 below, a list of masses that could arise from each site Figure 3. Most common oral masses What are the common salivary gland pathologies Salivary gland tumours (Figure 7) commonly present as channel referrals to appropriate specialists who are better HOW SHOULD A GP MANAGE THEM? of the oral cavity is given and elaborated briey. Among the that a GP should be aware of? painless growing masses which are usually benign. ey can equipped in centres to accurately diagnose and treat these Mr Tan Tai Joum, Dr Marie Stella P Cruz CDR had a slow-growing mass in the oral cavity over one year more common oral masses are: torus palatinus, torus occur in both major and minor salivary glands but are most patients, which usually involves surgical excision. but sought treatment only when he experienced a sudden acute mandibularis, pyogenic granuloma, mucocele, broma, ere are three pairs of major salivary glands (parotid, commonly found occurring in the parotid glands. e most 3) Salivary gland pathology may be primary or secondary to submandibular and sublingual) as well as hundreds of minor ABSTRACT onset of severe pain and numbness. He was fortunate to have leukoplakia and squamous cell carcinoma – photographs of common type of salivary gland tumour is the pleomorphic systemic causes. ese dierent diseases may present with not sought treatment as it had not caused any pain. -

Preprosthetic Surgery
Principles of Preprosthetic Surgery Preprosthetic Surgery • Define Preprosthetic Surgery • Review the work-up • Armamanterium • Importance of thinking SURGICALLY…… to enhance the PROSTHETICS • Review commonly occurring preprosthetic scenarios What is preprosthetic surgery? “Any surgical procedure performed on a patient aiming to optimize the existing anatomic conditions of the maxillary or mandibular alveolar ridges for successful prosthetic rehabilitation” What is preprosthetic surgery? “Procedures intended to improve the denture bearing surfaces of the mandible and maxilla” Preprosthetic Surgery • Types of Pre-Prosthetic Surgery – Resective – Recontouring – Augmentation • Involved areas – Osseous tissues – Soft tissues • Category of Patient – Completely edentulous patient – Partially edentulous patient Preprosthetic Surgery • Alteration of alveolar bone – Removing of undesirable features/contours • Osseous plasty/shaping/recontouring – Bone reductions – Bone repositioning – Bone grafting • Soft tissue modifications – Soft tissue plasty/recontouring – Soft tissue reductions – Soft tissue excisions – Soft tissue repositioning – Soft tissue grafting Preprosthetic Surgery Goals • Goals - To provide improvement to both form and function – Address functional impairments – Cosmetic - Improve the denture bearing surfaces – Alveolar (bone) ridges – Adjacent soft tissues Prosthetic Surgery Work-up Preprosthetic Surgery Work-Up • Considerations in developing the treatment plan – Chief complaint and expectations • Ascertain what the patient really -

Abscesses Apicectomy
BChD, Dip Odont. (Mondchir.) MBChB, MChD (Chir. Max.-Fac.-Med.) Univ. of Pretoria Co Reg: 2012/043819/21 Practice.no: 062 000 012 3323 ABSCESSES WHAT IS A TOOTH ABSCESS? A dental/tooth abscess is a localised acute infection at the base of a tooth, which requires immediate attention from your dentist. They are usually associated with acute pain, swelling and sometimes an unpleasant smell or taste in the mouth. More severe infections cause facial swelling as the bacteria spread to the nearby tissues of the face. This is a very serious condition. Once the swelling begins, it can spread rapidly. The pain is often made worse by drinking hot or cold fluids or biting on hard foods and may spread from the tooth to the ear or jaw on the same side. WHAT CAUSES AN ABSCESS? Damage to the tooth, an untreated cavity, or a gum disease can cause an abscessed tooth. If the cavity isn’t treated, the inside of the tooth can become infected. The bacteria can spread from the tooth to the tissue around and beneath it, creating an abscess. Gum disease causes the gums to pull away from the teeth, leaving pockets. If food builds up in one of these pockets, bacteria can grow, and an abscess may form. An abscess can cause the bone around the tooth to dissolve. WHY CAN'T ANTIBIOTIC TREATMENT ALONE BE USED? Antibiotics will usually help the pain and swelling associated with acute dental infections. However, they are not very good at reaching into abscesses and killing all the bacteria that are present. -

Risks and Complications of Orthodontic Miniscrews
SPECIAL ARTICLE Risks and complications of orthodontic miniscrews Neal D. Kravitza and Budi Kusnotob Chicago, Ill The risks associated with miniscrew placement should be clearly understood by both the clinician and the patient. Complications can arise during miniscrew placement and after orthodontic loading that affect stability and patient safety. A thorough understanding of proper placement technique, bone density and landscape, peri-implant soft- tissue, regional anatomic structures, and patient home care are imperative for optimal patient safety and miniscrew success. The purpose of this article was to review the potential risks and complications of orthodontic miniscrews in regard to insertion, orthodontic loading, peri-implant soft-tissue health, and removal. (Am J Orthod Dentofacial Orthop 2007;131:00) iniscrews have proven to be a useful addition safest site for miniscrew placement.7-11 In the maxil- to the orthodontist’s armamentarium for con- lary buccal region, the greatest amount of interradicu- trol of skeletal anchorage in less compliant or lar bone is between the second premolar and the first M 12-14 noncompliant patients, but the risks involved with mini- molar, 5 to 8 mm from the alveolar crest. In the screw placement must be clearly understood by both the mandibular buccal region, the greatest amount of inter- clinician and the patient.1-3 Complications can arise dur- radicular bone is either between the second premolar ing miniscrew placement and after orthodontic loading and the first molar, or between the first molar and the in regard to stability and patient safety. A thorough un- second molar, approximately 11 mm from the alveolar derstanding of proper placement technique, bone density crest.12-14 and landscape, peri-implant soft-tissue, regional anatomi- During interradicular placement in the posterior re- cal structures, and patient home care are imperative for gion, there is a tendency for the clinician to change the optimal patient safety and miniscrew success. -

Recognition and Management of Oral Health Problems in Older Adults by Physicians: a Pilot Study
J Am Board Fam Pract: first published as 10.3122/jabfm.11.6.474 on 1 November 1998. Downloaded from BRIEF REPORTS Recognition and Management of Oral Health Problems in Older Adults by Physicians: A Pilot Study Thomas V. Jones, MD, MPH, Mitchel J Siegel, DDS, andJohn R. Schneider, A1A Oral health problems are among the most com of the nation's current and future health care mon chronic health conditions experienced by needs, the steady increase in the older adult popu older adults. Healthy People 2000, an initiative to lation, and the generally high access elderly per improve the health of America, has selected oral sons have to medical care provided by family health as a priority area. l About 11 of 100,000 physicians and internists.s,7,8 Currently there is persons have oral cancer diagnosed every year.2 very little information about the ability of family The average age at which oral cancer is diagnosed physicians or internists, such as geriatricians, to is approximately 65 years, with the incidence in assess the oral health of older patients. We con creasing from middle adulthood through the sev ducted this preliminary study to determine how enth decade of life. l-3 Even though the mortality family physicians and geriatricians compare with rate associated with oral cancer (7700 deaths an each other and with general practice dentists in nually)4 ranks among the lowest compared with their ability to recognize, diagnose, and perform other cancers, many deaths from oral cancer initial management of a wide spectrum of oral might be prevented by improved case finding and health problems seen in older adults. -

GUIDE to SUTURING with Sections on Diagnosing Oral Lesions and Post-Operative Medications
Journal of Oral and Maxillofacial Surgery Journal of Oral and Maxillofacial August 2015 • Volume 73 • Supplement 1 www.joms.org August 2015 • Volume 73 • Supplement 1 • pp 1-62 73 • Supplement 1 Volume August 2015 • GUIDE TO SUTURING with Sections on Diagnosing Oral Lesions and Post-Operative Medications INSERT ADVERT Elsevier YJOMS_v73_i8_sS_COVER.indd 1 23-07-2015 04:49:39 Journal of Oral and Maxillofacial Surgery Subscriptions: Yearly subscription rates: United States and possessions: individual, $330.00 student and resident, $221.00; single issue, $56.00. Outside USA: individual, $518.00; student and resident, $301.00; single issue, $56.00. To receive student/resident rate, orders must be accompanied by name of affiliated institution, date of term, and the signature of program/residency coordinator on institution letter- head. Orders will be billed at individual rate until proof of status is received. Prices are subject to change without notice. Current prices are in effect for back volumes and back issues. Single issues, both current and back, exist in limited quantities and are offered for sale subject to availability. Back issues sold in conjunction with a subscription are on a prorated basis. Correspondence regarding subscriptions or changes of address should be directed to JOURNAL OF ORAL AND MAXILLOFACIAL SURGERY, Elsevier Health Sciences Division, Subscription Customer Service, 3251 Riverport Lane, Maryland Heights, MO 63043. Telephone: 1-800-654-2452 (US and Canada); 314-447-8871 (outside US and Canada). Fax: 314-447-8029. E-mail: journalscustomerservice-usa@ elsevier.com (for print support); [email protected] (for online support). Changes of address should be sent preferably 60 days before the new address will become effective. -

And Maxillofacial Pathology
Oral Med Pathol 12 (2008) 57 Proceedings of the 3rd Annual Meeting of the Asian Society of Oral and Maxillofacial Pathology Date: November 17-18, 2007 Venue: Howard International House, Taipei, the Republic of China Oraganizaing Committee: President: Chun-Pin Chiang, School of dentistry, College of Medicine, National Taiwan University Vice Presidents: Li-Min Lin, College of Dental Medicine kaohsiung Medical University, Ying-Tai Jin, National Cheng Kung University Secretary General: Ying-Tai Jin, Nationatl Cheng Kung University Organizers: Taiwan Academy of Oral Pathology and School of Dentistry of Medicine, National Taiwan University myoepithelial and/or basal cells, glycogen-rich clear cells, Special lecture squamous epithelial cells and oncocytic cells may also be found focally or extensively in different tumour types. 1. Classification and diagnosis of salivary gland Grading of malignancy: The presence of many low-grade tumors based on the revised WHO classification and intermediate-grade carcinomas, which show greater Hiromasa Nikai propensity for the indolent aggression, and the ability of Hiroshima University, Hiroshima, Japan long standing benign tumours to undergo malignant transformation are striking features of salivary carcinomas. (1) General remarks of salivary gland tumours Therefore, the most important work for pathologists at We oral pathologists often have difficulties and confuse diagnosis of salivary gland neoplasms is to distinguish these in diagnosis of salivary gland tumours. This will be low- or intermediate grade carcinomas from both benign and attributable to our lack of accumulated experience due to highly aggressive tumour types often bearing microscopic their overall rarity, comprising only about 1% of human resemblances for determining the choice of treatments. -

Oral Mucosal Lesions and Developmental Anomalies in Dental Patients of a Teaching Hospital in Northern Taiwan
Journal of Dental Sciences (2014) 9,69e77 Available online at www.sciencedirect.com journal homepage: www.e-jds.com ORIGINAL ARTICLE Oral mucosal lesions and developmental anomalies in dental patients of a teaching hospital in Northern Taiwan Meng-Ling Chiang a,b, Yu-Jia Hsieh b,c, Yu-Lun Tseng d, Jr-Rung Lin e, Chun-Pin Chiang f,g* a Department of Pediatric Dentistry, Chang Gung Memorial Hospital, Taipei, Taiwan b College of Medicine, Chang Gung University, Taoyuan, Taiwan c Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital, Taoyuan, Taiwan d Department of Psychiatry, College of Medicine, China Medical University, Taichung, Taiwan e Clinical Informatics and Medical Statistics Research Center, Chang Gung University, Taoyuan, Taiwan f Graduate Institute of Oral Biology, School of Dentistry, National Taiwan University, Taipei, Taiwan g Department of Dentistry, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei, Taiwan Received 1 June 2013; Final revision received 10 June 2013 Available online 27 July 2013 KEYWORDS Abstract Background/purpose: Oral mucosal lesions and developmental anomalies are dental patient; frequently observed in dental practice. The purpose of this study was to evaluate the preva- developmental lence of oral mucosal lesions and developmental anomalies in dental patients in a teaching anomaly; hospital in northern Taiwan. northern Taiwan; Materials and methods: The study group comprised 2050 consecutive dental patients. From oral mucosal lesion; January 2003 to December 2007, the patients received oral examination and treatment in prevalence; the dental department of the Chang Gung Memorial Hospital (Taipei, Taiwan). type Results: Only 7.17% of dental patients had no oral mucosal lesions or developmental anoma- lies. -

Perio 430 Study Review
PERIO 430 STUDY REVIEW A TASTY PERIO DX REVIEW 3 PRINCIPLES OF PERIODONTAL SURGERY 6 TYPES OF PERIO SURGERY 6 RESTORATIVE INTERRELATIONSHIP 9 BIOLOGIC WIDTH 9 CROWN LENGTHENING OR TEETH EXTRUSION 10 DRUG-INDUCED GINGIVAL OVERGROWTH 12 GINGIVECTOMY + GINGIVOPLASTY 13 OSSEOUS RESECTION 14 BONY ARCHITECTURE 14 OSTEOPLASTY + OSTECTOMY 15 EXAMINATION AND TX PLANNING 15 PRINCIPLES AND SEQUENCE OF OSSEOUS RESECTION SURGERY 16 SPECIFIC OSSEOUS RESHAPING SITUATIONS 17 SYSTEMIC EFFECTS IN PERIODONTOLOGY 18 SYSTEMIC MODIFIERS 18 MANIFESTATION OF SYSTEMIC DISEASES 19 SPECIFIC EFFECTS OF ↑ INFLAMMATION 21 SOFT TISSUE WOUND HEALING 22 HOW DO WOUNDS HEAL? 22 DELAYED WOUND HEALING AND CHRONIC WOUNDS 25 ORAL MUCOSAL HEALING 25 PERIODONTAL EMERGENCIES 25 NECROTIZING GINGIVITIS (NG) 26 NECROTIZING PERIODONTITIS 27 ACUTE HERPETIC GINGIVOSTOMATITIS 27 ABSCESSES OF THE PERIODONTIUM 28 ENDO-PERIODONTAL LESIONS 30 POSTOPERATIVE CARE 31 MUCOGINGIVAL PROBLEMS 32 MUCOSA AND GINGIVA 33 MILLER CLASSIFICATION FOR RECESSION 33 1 | P a g e SURGICAL PROCEDURES 34 ROOT COVERAGE 36 METHODS 37 2 | P a g e A tasty Perio Dx Review Gingival and Periodontal Health Gingivitis Periodontitis 3 | P a g e Staging: Periodontitis Stage I Stage II Stage III Stage IV Features Severity Interdental CAL 1-2mm 2-4mm ≥ 5mm ≥ 5mm Radiographic Bone Loss <15% (Coronal 1/3) 15-30% >30% (Middle 3rd +) >30% (Middle 3rd +) (RBL) Tooth Loss (from perio) No Tooth Loss ≤ 4 teeth ≥ 5 teeth Complexity Local -Max probing ≤ 4mm -Max Probing ≤5mm -Probing ≥ 6mm Rehab due to: -Horizontal Bone loss -Horizontal -

Oral Health and Disease
Downloaded from bmj.com on 19 August 2005 ABC of oral health: Oral health and disease Ruth Holt, Graham Roberts and Crispian Scully BMJ 2000;320;1652-1655 doi:10.1136/bmj.320.7250.1652 Updated information and services can be found at: http://bmj.com/cgi/content/full/320/7250/1652 These include: Rapid responses One rapid response has been posted to this article, which you can access for free at: http://bmj.com/cgi/content/full/320/7250/1652#responses You can respond to this article at: http://bmj.com/cgi/eletter-submit/320/7250/1652 Email alerting Receive free email alerts when new articles cite this article - sign up in the box at service the top right corner of the article Topic collections Articles on similar topics can be found in the following collections Dentistry and Oral Medicine (79 articles) Notes To order reprints of this article go to: http://www.bmjjournals.com/cgi/reprintform To subscribe to BMJ go to: http://bmj.bmjjournals.com/subscriptions/subscribe.shtml Clinical review Downloaded from bmj.com on 19 August 2005 ABC of oral health Oral health and disease Ruth Holt, Graham Roberts, Crispian Scully A healthy dentition and mouth is important to both quality of life and nutrition, and oral disease may affect systemic health, as Enamel covering crown Gingival crevice discussed in later articles in this series. (gingival sulcus) Dentine Development of the dentition Gingiva Pulp chamber Teeth form mainly from neuroectoderm and comprise a crown of insensitive enamel surrounding sensitive dentine and a root Periodontal ligament that has no enamel covering. -

Oral Mucosa Alterations in a Socioeconomically Deprived Region: Prevalence and Associated Factors
Epidemiology Epidemiology Oral mucosa alterations in a socioeconomically deprived region: prevalence and associated factors Raquel Gonçalves Abstract: This study aimed to evaluate the prevalence and factors as- (a) Vieira-Andrade sociated with oral mucosa alterations in patients from Vale do Jequiti- Flávia de Faria Zuquim Guimarães(b) nhonha, Brazil. The sample consisted of 511 patients of both genders. Charlles da Silva Vieira(b) Questionnaires were used to obtain information about patient gender, (b) Sarah Teixeira Carvalho Freire age, race, systemic disease state, medication use, cigarette use and alco- Maria Letícia Ramos-Jorge(a) Anacélia Mendes Fernandes(b) hol consumption. Physical examinations were then performed to identify lesions of the oral mucosa. Descriptive analyses, Chi-squared tests and logistic regressions were then used to analyze the results (p < 0.05, 95% (a) Departament of Pediatric Dentistry, School CI). In this population, 84.9% (434/511) of patients were found to have of Dentistry, Federal University of Vales of Jequitinhonha and Mucuri, Diamantina, alterations in their oral mucosa. The most common alterations were mel- MG, Brazil. anotic maculae (36.0%), linea alba (33.9%), traumatic ulcers (21.5%), (b) Departament of Stomatology, School of Fordyce’s granules (20.4%), coated tongue (12.5%) and fissured tongue Dentistry, Federal University of Vales of (10.0%). Melanotic maculae were more frequently observed in black pa- Jequitinhonha and Mucuri, Diamantina, tients, with an odds ration (OR) of 7.51. Being female was a statistically MG, Brazil. significant predictive factor for having a visible linea alba (OR: 1.90) and a fissured tongue (OR: 2.11).