WO 2017/077391 A2 11 May 2017 (11.05.2017) P O P C T
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cow's Milk Allergy in Dutch Children
Petrus et al. Clin Transl Allergy (2016) 6:16 DOI 10.1186/s13601-016-0105-z Clinical and Translational Allergy RESEARCH Open Access Cow’s milk allergy in Dutch children: an epigenetic pilot survey Nicole C. M. Petrus1*†, Peter Henneman2†, Andrea Venema2, Adri Mul2, Femke van Sinderen2, Martin Haagmans2, Olaf Mook2, Raoul C. Hennekam1,2, Aline B. Sprikkelman1‡ and Marcel Mannens2‡ Abstract Background: Cow’s milk allergy (CMA) is a common disease in infancy. Early environmental factors are likely to con- tribute to CMA. It is known that epigenetic gene regulation can be altered by environmental factors. We have set up a proof of concept study, aiming to detect epigenetic associations specific with CMA. Methods: We studied children from the Dutch EuroPrevall birth cohort study (N 20 CMA, N 23 controls, N 10 tolerant boys), age and gender matched. CMA was challenge proven. Bisulfite converted= DNA =(blood) was analyzed= using the 450K infinium DNA-methylation array. Four groups (combined, girls, boys and tolerant boys) were analysed between CMA and controls. Statistical analysis and pathway-analysis were performed in “R” using IMA, Minfi and the global-test package. Differentially methylated regions in DHX58, ZNF281, EIF42A and HTRA2 genes were validated by quantitative amplicon sequencing (ROCHE 454®). Results: General hypermethylation was found in the CMA group compared to control children, while this effect was absent in the tolerant group. Methylation differences were, among others, found in regions of DHX58, ZNF281, EIF42A and HTRA2 genes. Several of these genes are known to be involved in immunological pathways and associated with other allergies. Conclusion: We show that epigenetic associations are involved in CMA. -

Noelia Díaz Blanco
Effects of environmental factors on the gonadal transcriptome of European sea bass (Dicentrarchus labrax), juvenile growth and sex ratios Noelia Díaz Blanco Ph.D. thesis 2014 Submitted in partial fulfillment of the requirements for the Ph.D. degree from the Universitat Pompeu Fabra (UPF). This work has been carried out at the Group of Biology of Reproduction (GBR), at the Department of Renewable Marine Resources of the Institute of Marine Sciences (ICM-CSIC). Thesis supervisor: Dr. Francesc Piferrer Professor d’Investigació Institut de Ciències del Mar (ICM-CSIC) i ii A mis padres A Xavi iii iv Acknowledgements This thesis has been made possible by the support of many people who in one way or another, many times unknowingly, gave me the strength to overcome this "long and winding road". First of all, I would like to thank my supervisor, Dr. Francesc Piferrer, for his patience, guidance and wise advice throughout all this Ph.D. experience. But above all, for the trust he placed on me almost seven years ago when he offered me the opportunity to be part of his team. Thanks also for teaching me how to question always everything, for sharing with me your enthusiasm for science and for giving me the opportunity of learning from you by participating in many projects, collaborations and scientific meetings. I am also thankful to my colleagues (former and present Group of Biology of Reproduction members) for your support and encouragement throughout this journey. To the “exGBRs”, thanks for helping me with my first steps into this world. Working as an undergrad with you Dr. -

Paleovirology of 'Syncytins', Retroviral Env Genes Exapted for a Role in Placentation
Paleovirology of ‘syncytins’, retroviral env genes exapted for a role in placentation Christian Lavialle1,2, Guillaume Cornelis1,2, Anne Dupressoir1,2, Ce´cile Esnault1,2, Odile Heidmann1,2,Ce´cile Vernochet1,2 1,2 rstb.royalsocietypublishing.org and Thierry Heidmann 1UMR 8122, Unite´ des Re´trovirus Endoge`nes et E´le´ments Re´troı¨des des Eucaryotes Supe´rieurs, CNRS, Institut Gustave Roussy, 94805 Villejuif, France 2Universite´ Paris-Sud XI, 91405 Orsay, France Review The development of the emerging field of ‘paleovirology’ allows biologists to reconstruct the evolutionary history of fossil endogenous retroviral sequences Cite this article: Lavialle C, Cornelis G, integrated within the genome of living organisms and has led to the retrieval of conserved, ancient retroviral genes ‘exapted’ by ancestral hosts to fulfil Dupressoir A, Esnault C, Heidmann O, essential physiological roles, syncytin genes being undoubtedly among the Vernochet C, Heidmann T. 2013 Paleovirology most remarkable examples of such a phenomenon. Indeed, syncytins are of ‘syncytins’, retroviral env genes exapted for a ‘new’ genes encoding proteins derived from the envelope protein of endogen- role in placentation. Phil Trans R Soc B 368: ous retroviral elements that have been captured and domesticated on multiple 20120507. occasions and independently in diverse mammalian species, through a pro- http://dx.doi.org/10.1098/rstb.2012.0507 cess of convergent evolution. Knockout of syncytin genes in mice provided evidence for their absolute requirement for placenta development and embryo survival, via formation by cell–cell fusion of syncytial cell layers at One contribution of 13 to a Theme Issue the fetal–maternal interface. -

Polyclonal Antibody to MFSD2 (C-Term) - Aff - Purified
OriGene Technologies, Inc. OriGene Technologies GmbH 9620 Medical Center Drive, Ste 200 Schillerstr. 5 Rockville, MD 20850 32052 Herford UNITED STATES GERMANY Phone: +1-888-267-4436 Phone: +49-5221-34606-0 Fax: +1-301-340-8606 Fax: +49-5221-34606-11 [email protected] [email protected] AP26290PU-N Polyclonal Antibody to MFSD2 (C-term) - Aff - Purified Alternate names: HMFN0656, Major facilitator superfamily domain-containing protein 2, PP9177 Quantity: 0.1 mg Background: Multidrug transporters, such as MFSD2A, are membrane proteins that expel a wide spectrum of cytotoxic compounds from the cell and render cells resistant to multiple drugs. Major Facilitator Superfamily (MFS) members are capable of transporting various substrates such as sugars, polyols, drugs, neurotransmitters, amino acids, peptides, and inorganic anions, although most members are substrate-specific. MFSD2A is a novel lung cancer tumor suppressor gene that regulates cell cycle progression and matrix attachment and has recently been described as the human receptor for syncytin-2, a retrovirus-derived protein mediating fusion of placental trophoblasts. MFSD2A is expressed in many tissues and is highly induced in liver and brown adipose tissue (BAT) during fasting. The activation of the betaAR signaling pathway plays a major role in the induction of MFSD2A expression during adaptive thermogenesis. Uniprot ID: Q8NA29 NCBI: NP_001129965 GeneID: 84879 Host: Rabbit Immunogen: 18 amino acid peptide near the carboxy terminus of human MFSD2A Format: State: Liquid Ig fraction Purification: Affinity chromatography purified via peptide column Buffer System: PBS containing 0.02% sodium azide Applications: ELISA. Western blot: 1 - 2 µg/ml. Positive control: Lung Tissue Lysate. -
Supplementary Data
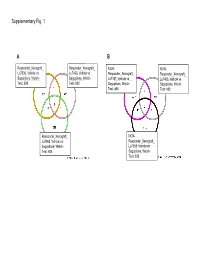
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type -

Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva
UCSF UC San Francisco Previously Published Works Title Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva. Permalink https://escholarship.org/uc/item/95h5g8mq Journal Cell reports, 33(7) ISSN 2211-1247 Authors Saitou, Marie Gaylord, Eliza A Xu, Erica et al. Publication Date 2020-11-01 DOI 10.1016/j.celrep.2020.108402 Peer reviewed eScholarship.org Powered by the California Digital Library University of California HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Cell Rep Manuscript Author . Author manuscript; Manuscript Author available in PMC 2020 November 30. Published in final edited form as: Cell Rep. 2020 November 17; 33(7): 108402. doi:10.1016/j.celrep.2020.108402. Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva Marie Saitou1,2,3, Eliza A. Gaylord4, Erica Xu1,7, Alison J. May4, Lubov Neznanova5, Sara Nathan4, Anissa Grawe4, Jolie Chang6, William Ryan6, Stefan Ruhl5,*, Sarah M. Knox4,*, Omer Gokcumen1,8,* 1Department of Biological Sciences, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 2Section of Genetic Medicine, Department of Medicine, University of Chicago, Chicago, IL, U.S.A 3Faculty of Biosciences, Norwegian University of Life Sciences, Ås, Viken, Norway 4Program in Craniofacial Biology, Department of Cell and Tissue Biology, School of Dentistry, University of California, San Francisco, CA, U.S.A 5Department of Oral Biology, School of Dental Medicine, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 6Department of Otolaryngology, School of Medicine, University of California, San Francisco, CA, U.S.A 7Present address: Weill-Cornell Medical College, Physiology and Biophysics Department 8Lead Contact SUMMARY Salivary proteins are essential for maintaining health in the oral cavity and proximal digestive tract, and they serve as potential diagnostic markers for monitoring human health and disease. -

Suppressyn Localization and Dynamic Expression Patterns in Primary Human Tissues Support a Physiologic Role in Human Placentation Jun Sugimoto1,4,5*, Danny J
www.nature.com/scientificreports OPEN Suppressyn localization and dynamic expression patterns in primary human tissues support a physiologic role in human placentation Jun Sugimoto1,4,5*, Danny J. Schust3,5, Tadatsugu Kinjo2, Yoichi Aoki2, Yoshihiro Jinno1 & Yoshiki Kudo4 We previously identifed suppressyn (SUPYN), a placental protein that negatively regulates the cell fusion essential for trophoblast syncytialization via binding to the trophoblast receptor for syncytin-1, ASCT2, and hypothesized that SUPYN may thereby regulate cell-cell fusion in the placenta. Here, we redefne in vivo SUPYN localization using specifc monoclonal antibodies in a rare early placental sample, showing SUPYN localization in villous and extravillous trophoblast subtypes, the decidua and even in placental debris in the maternal vasculature. In human trophoblast cell lines, we show SUPYN alters ASCT2 glycosylation within the secretory pathway and that this binding is associated with inhibition of cell fusion. Using newly-optimized trophoblast isolation protocols that allow tracking of ex vivo cell fusion, we present transcription and translation dynamics of fusion-related proteins over 96 hours in culture and the efects of changes in ambient oxygen levels on these processes. We report converse syncytin-1 and SUPYN transcriptional and translational responses to surrounding oxygen concentrations that suggest both are important in the efects of hypoxia and hyperoxia on placental syncytialization. Our results suggest that SUPYN’s anti-fusogenic properties may be exerted at several sites in the maternal body and its dysregulation may be associated with diseases of abnormal placentation. Tere are several types of human trophoblast cells, each with fairly well-characterized localization and function at the maternal-fetal interface. -

Catenin/T-Cell Factor Signaling Identified by Gene Expression Profiling of Ovarian Endometrioid Adenocarcinomas1
[CANCER RESEARCH 63, 2913–2922, June 1, 2003] Novel Candidate Targets of -Catenin/T-cell Factor Signaling Identified by Gene Expression Profiling of Ovarian Endometrioid Adenocarcinomas1 Donald R. Schwartz,2 Rong Wu,2 Sharon L. R. Kardia, Albert M. Levin, Chiang-Ching Huang, Kerby A. Shedden, Rork Kuick, David E. Misek, Samir M. Hanash, Jeremy M. G. Taylor, Heather Reed, Neali Hendrix, Yali Zhai, Eric R. Fearon, and Kathleen R. Cho3 Comprehensive Cancer Center and Departments of Pathology [D. R. S., R. W., H. R., N. H., Y. Z., E. R. F., K. R. C.], Internal Medicine [E. R. F., K. R. C.], Pediatrics and Communicable Diseases [R. K., D. E. M., S. M. H.], and Biostatistics [C-C. H., J. M. G. T.], School of Medicine, Department of Epidemiology [S. L. R. K., A. M. L.], School of Public Health and Statistics [K. A. S.], College of Literature Science and the Arts, University of Michigan, Ann Arbor, Michigan 48109-0638 ABSTRACT specific molecular and pathobiological features [reviewed by Feeley and Wells (2) and Aunoble et al. (3)].   The activity of -catenin ( -cat), a key component of the Wnt signaling OEAs4 are characterized by frequent (16–54%) mutations of pathway, is deregulated in about 40% of ovarian endometrioid adenocar- CTNNB1, the gene encoding -cat, a critical component of the Wnt cinomas (OEAs), usually as a result of CTNNB1 gene mutations. The signaling pathway (4–9). Wnts are a highly conserved family of function of -cat in neoplastic transformation is dependent on T-cell factor (TCF) transcription factors, but specific genes activated by the secreted growth factors that bind members of the frizzled family of interaction of -cat with TCFs in OEAs and other cancers with Wnt transmembrane receptors and, through downstream signaling, modu- pathway defects are largely unclear. -

The Genome-Wide Landscape of Copy Number Variations in the MUSGEN Study Provides Evidence for a Founder Effect in the Isolated Finnish Population
European Journal of Human Genetics (2013) 21, 1411–1416 & 2013 Macmillan Publishers Limited All rights reserved 1018-4813/13 www.nature.com/ejhg ARTICLE The genome-wide landscape of copy number variations in the MUSGEN study provides evidence for a founder effect in the isolated Finnish population Chakravarthi Kanduri1, Liisa Ukkola-Vuoti1, Jaana Oikkonen1, Gemma Buck2, Christine Blancher2, Pirre Raijas3, Kai Karma4, Harri La¨hdesma¨ki5 and Irma Ja¨rvela¨*,1 Here we characterized the genome-wide architecture of copy number variations (CNVs) in 286 healthy, unrelated Finnish individuals belonging to the MUSGEN study, where molecular background underlying musical aptitude and related traits are studied. By using Illumina HumanOmniExpress-12v.1.0 beadchip, we identified 5493 CNVs that were spread across 467 different cytogenetic regions, spanning a total size of 287.83 Mb (B9.6% of the human genome). Merging the overlapping CNVs across samples resulted in 999 discrete copy number variable regions (CNVRs), of which B6.9% were putatively novel. The average number of CNVs per person was 20, whereas the average size of CNV per locus was 52.39 kb. Large CNVs (41 Mb) were present in 4% of the samples. The proportion of homozygous deletions in this data set (B12.4%) seemed to be higher when compared with three other populations. Interestingly, several CNVRs were significantly enriched in this sample set, whereas several others were totally depleted. For example, a CNVR at chr2p22.1 intersecting GALM was more common in this population (P ¼ 3.3706 Â 10 À44) than in African and other European populations. The enriched CNVRs, however, showed no significant association with music-related phenotypes. -

A Comparative Genomics Approach to Using High-Throughput
The University of Maine DigitalCommons@UMaine Honors College 5-2013 A Comparative Genomics Approach to Using High-Throughput Gene Expression Data to Study Limb Regeneration in Ambystoma Mexicanum and Danio Rerio: Developing a More Completely Annotated Database Justin Bolinger University of Maine - Main Follow this and additional works at: https://digitalcommons.library.umaine.edu/honors Part of the Comparative and Evolutionary Physiology Commons, Genomics Commons, and the Molecular Genetics Commons Recommended Citation Bolinger, Justin, "A Comparative Genomics Approach to Using High-Throughput Gene Expression Data to Study Limb Regeneration in Ambystoma Mexicanum and Danio Rerio: Developing a More Completely Annotated Database" (2013). Honors College. 116. https://digitalcommons.library.umaine.edu/honors/116 This Honors Thesis is brought to you for free and open access by DigitalCommons@UMaine. It has been accepted for inclusion in Honors College by an authorized administrator of DigitalCommons@UMaine. For more information, please contact [email protected]. A COMPARATIVE GENOMICS APPROACH TO USING HIGH-THROUGHPUT GENE EXPRESSION DATA TO STUDY LIMB REGENERATION IN AMBYSTOMA MEXICANUM AND DANIO RERIO: DEVELOPING A MORE COMPLETELY ANNOTATED DATABASE by Justin Bolinger A Thesis Submitted in Partial Fulfillment of the Requirements for a Degree with Honors (Chemical Engineering) The Honors College University of Maine at Orono May 2013 Advisory Committee: Keith Hutchison, Department of Biochemistry and Molecular Biology, Advisor Benjamin King, Staff Scientist, Mount Desert Island Biological Laboratory, co-Advisor John Hwalek, Department of Chemical Engineering François Amar, Department of Chemistry Kevin Roberge, Department of Physics and Astronomy ABSTRACT Axolotl (Ambystoma mexicanum) and the zebrafish (Danio rerio) represent organisms extensively studied because of their remarkable capability of fully regenerating completely functional tissues after a traumatic event takes place. -

Consistent Biomarkers and Related Pathogenesis Underlying Asthma Revealed by Systems Biology Approach
International Journal of Molecular Sciences Article Consistent Biomarkers and Related Pathogenesis Underlying Asthma Revealed by Systems Biology Approach 1, 1, 1 1 2 3 Xiner Nie y, Jinyi Wei y, Youjin Hao , Jingxin Tao , Yinghong Li , Mingwei Liu , Boying Xu 1 and Bo Li 1,* 1 College of Life Sciences, Chongqing Normal University, Chongqing 401331, China 2 School of Biological Information, Chongqing University of Posts and Telecommunications, Chongqing 400065, China 3 College of Laboratory Medicine, Chongqing Medical University, Chongqing 400046, China * Correspondence: [email protected] These authors contributed equally to this work. y Received: 21 July 2019; Accepted: 17 August 2019; Published: 19 August 2019 Abstract: Asthma is a common chronic airway disease worldwide. Due to its clinical and genetic heterogeneity, the cellular and molecular processes in asthma are highly complex and relatively unknown. To discover novel biomarkers and the molecular mechanisms underlying asthma, several studies have been conducted by focusing on gene expression patterns in epithelium through microarray analysis. However, few robust specific biomarkers were identified and some inconsistent results were observed. Therefore, it is imperative to conduct a robust analysis to solve these problems. Herein, an integrated gene expression analysis of ten independent, publicly available microarray data of bronchial epithelial cells from 348 asthmatic patients and 208 healthy controls was performed. As a result, 78 up- and 75 down-regulated genes were identified -

Retrovirology Biomed Central
Retrovirology BioMed Central Research Open Access Identification of an endogenous retroviral envelope gene with fusogenic activity and placenta-specific expression in the rabbit: a new "syncytin" in a third order of mammals Odile Heidmann†, Cécile Vernochet†, Anne Dupressoir and Thierry Heidmann* Address: Unité des Rétrovirus Endogènes et Eléments Rétroïdes des Eucaryotes Supérieurs, CNRS UMR 8122, Institut Gustave Roussy, 39 rue Camille Desmoulins, F-94805 Villejuif, and Université Paris-Sud, Orsay, F-91405, France Email: Odile Heidmann - [email protected]; Cécile Vernochet - [email protected]; Anne Dupressoir - [email protected]; Thierry Heidmann* - [email protected] * Corresponding author †Equal contributors Published: 27 November 2009 Received: 22 October 2009 Accepted: 27 November 2009 Retrovirology 2009, 6:107 doi:10.1186/1742-4690-6-107 This article is available from: http://www.retrovirology.com/content/6/1/107 © 2009 Heidmann et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: Syncytins are envelope genes of retroviral origin that have been co-opted by the host to mediate a specialized function in placentation. Two of these genes have already been identified in primates, as well as two distinct, non orthologous genes in rodents. Results: Here we identified within the rabbit Oryctolagus cuniculus-which belongs to the lagomorpha order- an envelope (env) gene of retroviral origin with the characteristic features of a bona fide syncytin, that we named syncytin-Ory1.