Histology List 106 0828
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Scalp Eczema Factsheet the Scalp Is an Area of the Body That Can Be Affected by Several Types of Eczema
12 Scalp eczema factsheet The scalp is an area of the body that can be affected by several types of eczema. The scalp may be dry, itchy and scaly in a chronic phase and inflamed (red), weepy and painful in an acute (eczema flare) phase. Aside from eczema, there are a number of reasons why the scalp can become dry and itchy (e.g. psoriasis, fungal infection, ringworm, head lice etc.), so it is wise to get a firm diagnosis if there is uncertainty. Types of eczema • Hair clips and headgear – especially those containing that affect the scalp rubber or nickel. Seborrhoeic eczema (dermatitis) is one of the most See the NES booklet on Contact Dermatitis for more common types of eczema seen on the scalp and hairline. details. It can affect babies (cradle cap), children and adults. The Irritant contact dermatitis is a type of eczema that skin appears red and scaly and there is often dandruff as occurs when the skin’s surface is irritated by a substance well, which can vary in severity. There may also be a rash that causes the skin to become dry, red and itchy. on other parts of the face, such as around the eyebrows, For example, shampoos, mousses, hair gels, hair spray, eyelids and sides of the nose. Seborrhoeic eczema can perm solution and fragrance can all cause irritant contact become infected. See the NES factsheets on Adult dermatitis. See the NES booklet on Contact Dermatitis for Seborrhoeic Dermatitis and Infantile Seborrhoeic more details. Dermatitis and Cradle Cap for more details. -

Nail Anatomy and Physiology for the Clinician 1
Nail Anatomy and Physiology for the Clinician 1 The nails have several important uses, which are as they are produced and remain stored during easily appreciable when the nails are absent or growth. they lose their function. The most evident use of It is therefore important to know how the fi ngernails is to be an ornament of the hand, but healthy nail appears and how it is formed, in we must not underestimate other important func- order to detect signs of pathology and understand tions, such as the protective value of the nail plate their pathogenesis. against trauma to the underlying distal phalanx, its counterpressure effect to the pulp important for walking and for tactile sensation, the scratch- 1.1 Nail Anatomy ing function, and the importance of fi ngernails and Physiology for manipulation of small objects. The nails can also provide information about What we call “nail” is the nail plate, the fi nal part the person’s work, habits, and health status, as of the activity of 4 epithelia that proliferate and several well-known nail features are a clue to sys- differentiate in a specifi c manner, in order to form temic diseases. Abnormal nails due to biting or and protect a healthy nail plate [1 ]. The “nail onychotillomania give clues to the person’s emo- unit” (Fig. 1.1 ) is composed by: tional/psychiatric status. Nail samples are uti- • Nail matrix: responsible for nail plate production lized for forensic and toxicology analysis, as • Nail folds: responsible for protection of the several substances are deposited in the nail plate nail matrix Proximal nail fold Nail plate Fig. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Pedicure: Nail Enhancements
All Hair Services Include Shampoo All Services Based on Student Availability Long Hair is Extra & Senior Price Available Hair Cuts: Color: (Does Not Include Cut & Style) Hair Cut (Hood dryer) $6.50 Retouch/Tint/PM Shine $14.50 With Blowdry $13.50 Additional Application $8.00 With Blowdry & Flat Iron $21.50 Color (All over color) $20.00 Foils Each $4.00 Hair Styles: Hair Length to Collar $38.00 Shampoo/Set $6.75 Hair Length to Shoulder $48.00 Spiral Rod Set $20.00 Hair Length past Shoulder $58.00 Shampoo/ Blowdry $9.00 Frosting with Cap $17.50 With Thermal Iron $13.00 Men’s Comb Highlight with Cut $15.00 With Flat Iron $15.00 With Press & Curl $18.00 Perms & Relaxers: (Includes Cut & Style) Wrap Only $6.50 Regular or Normal Hair $20.95 Wrap with Roller Set $10.50 Resistant or Tinted Hair $26.00 Fingerwaves with Style $17.50 Spiral or Piggyback $36.00 Twists $3.00 Relaxer $35.00 Straight Back $20.00 Curled $15.00 Other Hair Services: Spiral $20.00 Shampoo Only $2.00 French Braids with Blowdry $15.00 Line-up $3.00 Under 10 Braids $20.00 Deep Condition $5.00 Over 10 Braids $25.00 Keratin Treatment $15.00 Braid Removal $15.00 Updo or French Roll $20.00 Manicure: Spa Manicure $9.50 Waxing: French Manicure $8.00 Brow $6.00 Manicure $6.42 Lip $5.00 Chin $5.00 Pedicure: Full Face $15.00 Spa Pedicure $20.00 Half Leg $15.00 French Pedicure $17.00 Full Leg $30.00 Pedicure $15.00 Underarm $15.00 Half Arm $10.00 Nail Enhancements: Full Arm $15.00 Shellac (French $2) $15.00 Mid Back & Up $15.00 Overlay (Natural Nail) $12.00 Full Back $25.00 Acrylic Full Set $16.50 Bikini $25.00 Gel Full Set $18.00 Fill-in Gel & Acrylic $12.00 Massages: Nail Repair( Per Nail) $2.00 Relaxation $15.00 Soak Off $3.00 Deep Tissue $19.95 Nail Art (Per Nail) $1.00 Other Nail Services: Nails & Waxing Services Taxable Polish Change $4.00 Nails Clipped $5.00 Paraffin Dip Wax $5.00 . -

318 Reports the Scalp Topography of the Human Visually Evoked Subcortical Potential. G. F. A
Invest. Ophthalmol. Vis. Sci. 318 Reports March 1980 We are indebted to Dr. G. van Lith, Oogziekenhuis, gested the optic nerve as its origin. Cracco and Rotterdam, and to Dr. D. van Norren, Ooglijdersgast- Cracco3 described early oscillatory potentials at huis, Utrecht, for testing our lens design and for sug- 100 cy/sec recorded from a wide scalp distribution gestions for improvement in the manuscript. of electrodes, referred to earlobe electrodes. Early From the Kliniek voor Oogheelkunde, Rijks-Universi- in 1979 we identified a triphasic positive- teit Groningen, Groningen, The Netherlands. Submit- negative-positive component (msec) in some sub- ted for publication July 2, 1979. Reprint requests: Aart jects at latencies of positive 22 (P22)> negative 27 C. Kooijman, Kliniek voor Oogheelkunde, Rijks-Uni- (N27), and positive 35 (Pas).4 Since it appeared im- versiteit Groningen, Oostersingel 59, 9713 EZ Gronin- portant to delineate this component from both the gen, The Netherlands. scalp-recorded ERG and the VECP, we have car- Key words: ERG, Ganzfeld stimulator, LED light ried out a topographic study of the scalp dis- tribution. Materials and method. Observations were made REFERENCES on 14 normal volunteer subjects (eight male and 1. Thijssen JM, Braakhuis W, Pinckers A, and van Lith six female) ages between 19 and 38 years (mean 26 G: Standardized electro-ophthalmography. In Pro- years). All had visual acuities of 6/6 or better. For ceedings of the 170th meeting of the Netherlands this topographical study, electrodes were placed Ophthalmological Society. Junk, The Hague, 1976, according to the International 10/20 system.5 In p. -
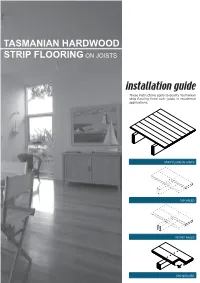
Tasmanian Hardwood Strip Flooring on Joists Guide for Installing
TASMANIAN HARDWOOD STRIP FLOORING ON JOISTS installation guide These instructions apply to quality Tasmanian strip flooring fixed over joists in residential applications. STRIP FLOOR ON JOISTS TOP NAILED SECRET NAILED END MATCHED TOOLS Simple tools are adequate in most applications. Necessary tools are: Tool Requirement Checklist Pencil, tape measure and square Hammer, punch and nail bag Stringline, spirit level and straight edge Hand saw and jig saw Safety glasses, dust mask and knee pads Spacers (about 100mm long and 2 mm thick) Rubber mallet, broom and vacuum cleaner Framing chisel For specialist applications, a drop saw, an air power staple gun, a power actuated fastener system and a cramping system may be useful. MATERIALS Use quality boards of the correct thickness. Grade descriptions for strip flooring are set out in the Australian Standard AS 2796 and are available at: www.tastimber.tas.gov.au. Boards at least 19 mm thick are needed to span 450 mm. Board width - Only secret nail boards up to 85 mm cover width. Secret nailed flooring is fixed through the tongue of specially profiled boards. Since they are only secured with one fastener per joist or batten, their width is limited to 85 mm cover. Board over 85 cover must be top nailed with two fasteners per joist. Use the correct nails for the job. The nail sizes required by Australian Standard 1684 are: Nail sizes for T & G flooring to joists* Nail sizes for T & G flooring to plywood substrate* Nailing Softwood Hardware & Strip flooring Rec. nailing (min.15mm substrate) joists cypress joists thicknes (mm) Hand 65 x 2.8 mm 50 x 2.8 mm 38 x 16 guage chisel point staples or driven bullet head bullet head 19 or 20 38 x 2.2 mm nails at 300mm spacing 32 x 16 guage chisel point staples or Machine 12,19 or 20 driven 65 x 2.5 mm 50 x 2.5 mm 30 x 2.2 mm nails at 200mm spacing *Alternative fasteners can be used for substrates types not listed subject to manufacturers’ recommendation. -

Regional Handwashing Policy
SOUTHERN CALIFORNIA GRADUATE MEDICAL EDUCATION POLICY AND PROCEDURE POLICY INFECTION PREVENTION AND CONTROL POLICIES EFFECTIVE DATE: SECTION: AND PROCEDURES 7/1/2014 TITLE: Hand Health & Hygiene Page: 1 of 8 BACKGROUND Studies have shown that handwashing causes a reduction in the carriage of potential pathogens on the hands. Microorganisms proliferate on the hands within the moist environment of gloves. Handwashing results in the reduction of patient morbidity and mortality from health care associated infections. The Centers for Disease Control and Prevention states that handwashing is the single most important procedure for preventing health-care associated infections. Artificial nails are more likely than natural nails to harbor pathogens that can lead to health care associated infections. There are four types of hand washing (see body of policy for detailed instructions): TYPE PURPOSE METHOD Routine Handwashing To remove soil and transient Wash hands with soap and microorganisms. water for at least 15 seconds. Hand antisepsis To remove soil and remove or Wash hands with antimicrobial destroy transient soap and water for at least 15 microorganisms. seconds. Hand rub/degerming To destroy transient and Rub alcohol-based hand resident microorganisms on degermer into hands vigorously UNSOILED hands. until dry. Surgical hand scrub To remove or destroy transient Wash hands and forearms with microorganisms and reduce antimicrobial soap and water resident flora. with brush to achieve friction. Or alcohol-based preparation rubbed vigorously -

White Nail As a Static Physical Finding: Revitalization of Physical Examination
Case Report White Nail as a Static Physical Finding: Revitalization of Physical Examination Ryuichi Ohta 1,* and Chiaki Sano 2 1 Community Care, Unnan City Hospital, 699-1221 96-1 Iida, Daito-cho, Unnan 699-1221, Shimane Prefecture, Japan 2 Department of Community Medicine Management, Faculty of Medicine, Shimane University, 89-1 Enya cho, Izumo 693-8501, Shimane Prefecture, Japan; [email protected] * Correspondence: [email protected]; Tel.: +81-9050605330 Abstract: Physical examinations are critical for diagnosis and should be differentiated into static and dynamic categories. One of the static findings is white nail, such as Terry’s and Lindsay’s nails. Here, we report the cases of two older patients with acute diseases who had nail changes that aided evaluation of their clinical course. Two elderly women who presented with acute conditions were initially thought to have normal serum albumin levels. They were found to have white nail with differences in nail involvement of the first finger, which subsequently revealed their hypoalbuminemia. The clinical courses were different following the distribution of nail whitening. Our findings show that examination of a white nail could indicate the previous clinical status more clearly than laboratory data. It can be useful for evaluating preclinical conditions in patients with acute diseases. Further evaluation is needed to establish the relationship between clinical outcomes and the presence of white nail in acute conditions among older patients. Citation: Ohta, R.; Sano, C. White Keywords: Lindsay’s nail; nail findings; nutritional assessment; physical examination; Terry’s nail; Nail as a Static Physical Finding: white nail Revitalization of Physical Examination. -

Curry-Assisted Diagnosis in the Rheumatology Clinic Sarah L
Oxford Medical Case Reports, 2015; 6, 297–299 doi: 10.1093/omcr/omv040 Case Report CASE REPORT Curry-assisted diagnosis in the rheumatology clinic Sarah L. Donaldson1,*, Maura Cobine-Davies1, Ann W. Morgan2, Andrew Gough3, and Sarah L. Mackie2 1Leeds Teaching Hospitals NHS Trust, Leeds, UK, 2Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds, Leeds, UK, and 3Rheumatology Department, Harrogate and District Foundation NHS Trust, Harrogate, UK *Correspondence address. 25 Oakdale Glen, Harrogate, North Yorkshire HG1 2JY, UK. Tel: +44-7745700247; E-mail: [email protected] Abstract We report five cases of glucocorticoid-responsive mouth symptoms in polymyalgia rheumatica/giant cell arteritis (GCA); three cases of tongue pain exacerbated by hot/spicy food, a case of scalp pain made worse by eating hot/spicy food and a case of sore tongue as a presenting feature of GCA. These cases emphasize the importance of asking about mouth symptoms and changes in taste when evaluating patients with suspected GCA. INTRODUCTION pain on eating [8]. The author mentions that burning or painful tongue has been reported in three previous cases of GCA [8]. Giant cell arteritis (GCA) is a systemic large-vessel vasculitis We report five cases of glucocorticoid-responsive mouth (LVV) affecting people older than 50 years. It classically causes symptoms in PMR/GCA; three cases of tongue pain exacerbated headache and ischaemia of cranial structures, resulting in jaw by spicy food, a case of scalp pain made worse by eating spicy claudication and visual disturbance. GCA may be accompanied food and a case of sore tongue as a presenting feature of GCA. -

Pretty Scary 2 Unmasking Toxic Chemicals in Kids’ Makeup
Prevention October 2016 Starts Here Campaign for Safe Cosmetics Pretty Scary 2 Unmasking toxic chemicals in kids’ makeup breastcancerfund.org 1 Acknowledgements Developed and published by the Breast Cancer Fund and spearheaded by their Campaign for Safe Cosmetics, this report was written by Connie Engel, Ph.D.; Janet Nudelman, MA; Sharima Rasanayagam, Ph.D.; Maija Witte, MPH; and Katie Palmer. Editing, messaging and vision were contributed by Denise Halloran and Erika Wilhelm. Sara Schmidt, MPH, MSW, coordinated the purchasing of products reviewed in this report and worked closely with partners to share the message. Thank you to James Consolantis, our contributing content specialist and Rindal&Co for design direction. WE ARE GRATEFUL FOR THE GENEROUS CONTRIBUTIONS FROM OUR FUNDERS: As You Sow Foundation, Jacob and Hilda Blaustein Foundation, Lisa and Douglas Goldman Foundation, Park Foundation, Passport Foundation, and the Serena Foundation. breastcancerfund.org 2 Our partners in purchasing products Pam Miller, Alaska Community Action on Toxics, Alaska Brooke Sarmiento, BEE-OCH Organics, Colorado Sara Schmidt, Breast Cancer Fund, California Susan Eastwood, Clean Water Action, Connecticut Anne Hulick, Clean Water Action, Connecticut Johnathan Berard, Clean Water Action, Rhode Island Lauren Carson, Clean Water Action, Rhode Island Cindy Luppi, Clean Water Action, Massachusetts Kadineyse Ramize Peña, Clean Water Action, Massachusetts Elizabeth Saunders, Clean Water Action, Massachusetts Sara Lamond, Fig & Flower, Georgia Beverly Johnson, -

Management of Ingested Foreign Bodies in Children: a Clinical Report of the NASPGHAN Endoscopy Committee
COMMITTEE COMMENTARY Management of Ingested Foreign Bodies in Children: A Clinical Report of the NASPGHAN Endoscopy Committee ÃRobert E. Kramer, yDiana G. Lerner, zTom Lin, §Michael Manfredi, jjManoj Shah, ôThomas C. Stephen, #Troy E. Gibbons, ÃÃHarpreet Pall, yyBen Sahn, zzMark McOmber, §§George Zacur, ÃJoel Friedlander, jjjjAntonio J. Quiros, ôôDouglas S. Fishman, and ##Petar Mamula ABSTRACT ingestion. Furthermore, changes in the types of ingestions encountered, Foreign body ingestions in children are some of the most challenging clinical specifically button batteries and high-powered magnet ingestions, create scenarios facing pediatric gastroenterologists. Determining the indications an even greater potential for severe morbidity and mortality among and timing for intervention requires assessment of patient size, type of object children. As a result, clinical guidelines regarding management of these ingested, location, clinical symptoms, time since ingestion, and myriad other ingestions in children remain varied and sporadic, with little in the way of factors. Often the easiest and least anxiety-producing decision is the one to prospective data to guide their development. An expert panel of pediatric proceed to endoscopic removal, instead of observation alone. Because of endoscopists was convened and produced the present article that outlines variability in pediatric patient size, there are less firm guidelines available to practical clinical approaches to the pediatric patient with a variety of determine which type of object will safely pass, as opposed to the clearer foreign body ingestions. This guideline is intended as an educational tool guidelines in the adult population. In addition, the imprecise nature of the that may help inform pediatric endoscopists in managing foreign body ingestions in children. -
Healthy Hair Healthy Scalp
Healthy hair starts with a healthy scalp Understanding and treating common scalp problems #1 dermatologist recommended therapeutic shampoo brand Recognizing common scalp conditions The largest organ of the human body is the skin. Like any DANDRUFF organ or other part of the body, the skin is constantly healing Symptoms typically include itching, and rebuilding itself by creating new cells and shedding flaking, and dryness of the scalp. old ones. The same regenerative process happens on the scalp when skin cells complete their life cycle, then flake off. This kind of flaking is healthy and usually unnoticeable. Sometimes, people experience increased levels of scalp dryness and flaking. This can result from temporary changes like cold weather, washing hair too often or not often enough, or even stress. SCALP PSORIASIS Dandruff, on the other hand, is a chronic condition Symptoms include inflammation recognized by persistent flaking, itching, and irritation of and the build-up of powdery, large, the scalp. Dandruff has many causes including dry skin, silvery plaques on the skin’s surface, infrequent shampooing, sensitivity to hair care products, a especially on the knees, elbows, and yeast-like fungus, or a skin condition that causes a disruption scalp. The severity of scalp psoriasis can vary from thin and loose, to thick in the rhythm of skin renewal on the scalp that can result in and crusted plaques. too many cells shedding too quickly. While dandruff is responsible for most itchy, flaky scalp symptoms, two less common conditions also cause SEBORRHEIC DERMATITIS persistent flaking and scalp irritation: scalp psoriasis and Symptoms include reddened, irritated seborrheic dermatitis.