Strengthening and Activating District Health System (Sahas) Fifth Bi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CHITWAN-ANNAPURNA LANDSCAPE: a RAPID ASSESSMENT Published in August 2013 by WWF Nepal
Hariyo Ban Program CHITWAN-ANNAPURNA LANDSCAPE: A RAPID ASSESSMENT Published in August 2013 by WWF Nepal Any reproduction of this publication in full or in part must mention the title and credit the above-mentioned publisher as the copyright owner. Citation: WWF Nepal 2013. Chitwan Annapurna Landscape (CHAL): A Rapid Assessment, Nepal, August 2013 Cover photo: © Neyret & Benastar / WWF-Canon Gerald S. Cubitt / WWF-Canon Simon de TREY-WHITE / WWF-UK James W. Thorsell / WWF-Canon Michel Gunther / WWF-Canon WWF Nepal, Hariyo Ban Program / Pallavi Dhakal Disclaimer This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Kathmandu Forestry College (KAFCOL) and do not necessarily reflect the views of WWF, USAID or the United States Government. © WWF Nepal. All rights reserved. WWF Nepal, PO Box: 7660 Baluwatar, Kathmandu, Nepal T: +977 1 4434820, F: +977 1 4438458 [email protected] www.wwfnepal.org/hariyobanprogram Hariyo Ban Program CHITWAN-ANNAPURNA LANDSCAPE: A RAPID ASSESSMENT Foreword With its diverse topographical, geographical and climatic variation, Nepal is rich in biodiversity and ecosystem services. It boasts a large diversity of flora and fauna at genetic, species and ecosystem levels. Nepal has several critical sites and wetlands including the fragile Churia ecosystem. These critical sites and biodiversity are subjected to various anthropogenic and climatic threats. Several bilateral partners and donors are working in partnership with the Government of Nepal to conserve Nepal’s rich natural heritage. USAID funded Hariyo Ban Program, implemented by a consortium of four partners with WWF Nepal leading alongside CARE Nepal, FECOFUN and NTNC, is working towards reducing the adverse impacts of climate change, threats to biodiversity and improving livelihoods of the people in Nepal. -

Submitted to Submitted by Constraints of the Construction
Constraints of the Construction Market in Earthquake Affected Districts in Nepal Market Research Study for the NPER Programme Final Report February 25, 2018 Submitted By Submitted To Nepal Development Research Institute Mott MacDonald), Shree Durbar Tole, Pulchowk, Lalitpur Kathmandu, Nepal GPO Box: 8975, EPC 2201, Kathmandu, Nepal Email: [email protected] Telephone: +977-1-5537362, 5554975 Table of Contents Abbreviation ....................................................................................................................... iii List of Tables ........................................................................................................ iv List of Graphs and Figures ....................................................................................... v Executive Summary ........................................................................................................... vi 1. Introduction ..................................................................................................................... 1 1.1 Background ........................................................................................................................................... 1 Objective of Study ....................................................................................................................................... 2 2. Methodology .................................................................................................................... 3 2.1 Approach of Study ............................................................................................................................... -

Inner Page Final.Indd
136-145 J. Nat. Hist. Mus. Vol. 26, 2012 LYMPHATIC FILARIASIS: EPIDEMIOLOGICAL ANALYSIS OF THE SITUATION IN SALYANTAR VDC OF DHADING DISTRICT, NEPAL R. Byanju1 and R. Gupta2 ABSTRACT A cross sectional survey was carried out by taking 516 mid night blood samples from 206 households in 1,2 and 3 wards of Salyantar village development committee of Dhading dis- trict, Nepal with the objective to analyze the epidemiological situation of lymphatic fi lariasis. The main aim of the study was to provide the data essential for the planning, implementation and evaluation of the services to the prevention, control and treatment of lymphatic fi lariasis. Questionnaire survey was conducted for the collection of information of the respondents. Blood samples were collected by means of ear-lobe prick method. Microscopical examination of the collected blood samples revealed 117 positive cases i.e. 22.67%. Males (24.54%) were found to be infected more than females (21.28%) in the ration of 1.2:1. The highest distribution of microfi larial parasites was in the age group >70 years (36.36%) while the least was in the age group ≤10 years (12.37%). The infected youngest person was 4 years old boy and the oldest was 85 years old man. Endemicity rate and crude disease rate was reported to be 44.76% and 22.09% respectively. Illiteracy, lack of awareness about the disease, poor sanitation, carelessness in using bed-nets and health were identifi ed as the major risk factors for fi lariasis. Key Words: lymphodema, elephantiasis, microfi laria, Wuchereria bancrofti, hydrocoele, crude disease rate INTRODUCTION Lymphatic fi lariasis (LF), also known as elephantiasis is a parasitic disease caused by fi larial nematode, Wuchereria bancrofti, the infection of which causes the infl ammation of lymphatic system resulting hydrocoele of scrotum, breast enlargement, lymphodema of limbs, enlarge- ment of penis, swollen clitoris and vulva. -

COVID-19 Commodity Issued Detail Report, May 10 to June
COVID-19 Commodity issued detail report, May 10 to June 16th June 2021, Source eLMIS, 16th June,2021 Dispatched Health Facility with items Quantity Province Health Logistic Management Center, Biratnagar 3 Way Connector 1000 Adult diaper 118 Ambu Bag with mask 30 Antigen Kit Covid-19 186750 Azithromycin 500 mg Tablet 200 Biochlor Disinfectant 10ml Sachet (Sodium Hypochlorite) 19800 Bipap Machine 15 Central Venous Catheter (CVS) 80 CPAP 15 Dead Body Bag 296 Depo (DMPA-Injectable) 100000 Disposable Syringe 50 ml 2000 Examination (loose) Gloves COVID-19 108500 Exteena 1600 Face Shield (COVID 19) 70000 Foleys Catheter 16 G 300 Gown for reusable (COVID-19) 1625 Gown Set (COVID-19) 13200 Hand Sanitizer 1000 ML 1200 Hydrocortisone Injection 400 Infrared Thermometer Piece COVID-19 55 IV Cannula 18 g 600 IV Cannula 20 g 600 IV Set 4600 Mask (COVID-19) 1046500 N95 Mask (COVID-19) 177880 Nasal Cannula 200 Nebulization Set 200 NG Tube 600 Oxygen Concentrator 10 Ltr 30 Oxygen Concentrator 5 Ltr 30 Oxygen Cylinder 40L 450 Paracetamol 125 mg / 5 ml 60 ml Syrup 2000 Pills Cycle 2400 Pulse Oxymeter spot check 649 Safety Goggles (COVID-19) 5300 Shoe Cover (COVID 19) 3200 Surgical Cap 3000 Syringe 2 ml 100000 T piece 600 Underpad (60*90 cm silicon release liner) 400 Urinal Disposable 270 Urobag 7 Ventilator Circuit 50 Venturi Mask 100 Yankauer Suction 550 Province Health Logistic Management Center, Butwal Antigen Kit Covid-19 221750 Biochlor Disinfectant 10ml Sachet (Sodium Hypochlorite) 21600 Bipap Machine 5 Collection Tube 1.5ml 4000 CPAP 5 Dead Body Bag -

Rural Municipality Transport Master Plan(RMTMP)
Local Government Gangajamuna Rural Municipality Office of the Rural Municipal Executive Phulkharka, Dhading Bagamati Province, Nepal Rural Municipality Transport Master Plan (RMTMP) Volume- I-Main Report Final Draft Submitted By Sarthak Engineering Consultancy Pvt. Ltd. Baneshwor, Kathmandu Gangajamuna Rural Municipality Office of the Rural Municipal Executive Bagmati Province, Dhading district This document is the draft report prepared for the project, “Rual Municipality Transport Master Plan (RMTMP)” undertaken by Gangajamuna Rural Municipal Office, Dhading district. This document has been prepared by Sarthak Engineering Consultancy Pvt. Ltd. for Gangajamuna Rural Municipality, Office of the Rural Municipal Executive, Dhading district. The opinions, findings and conclusions expressed herein are those of the Consultant and do not necessarily reflect those of the Rural Municipality. Data Sources and Credits Data sets, drawings and other miscellaneous data are produced/ developed by Sarthak Engineering Consultancy Pvt. Ltd. for the project during 2019/2020. These data are owned by Gangajamuna Rural Municipality, Office of the Rural Municipal Executive, Dhading. Authorization from the owner is required for the usage and/or publication of the data in part or whole. Name of the Project Rural Municipality Transport Master Plan (RMTMP) of Gangajamuna Rural Municipality Project Executing Agency Gangajamuna Rural Municipality Office of the Rural Municipal Executive Bagmati Province, Dhading district Implementing Agency Gangajamuna Rural Municipality -

S.N Batch RS/RV GID SLIP NO Grievant Name PA NO
S.N Batch RS/RV GID SLIP_NO Grievant Name PA_NO Houseowner Name DISTRICT GP/NP Ward Recommendation Clarification 1 2 RS 987011 9931965 Shanta Gyawali G-51-5-3-0-0001 Shanta Gyawali Arghakhanchi Parini Rural Municipality 3 RCB Probable Beneficiary 2 2 RS 987001 9987747 Sabitra Poudel G-51-2-14-0-0001 Sabitra Poudel Arghakhanchi Sitganga Urban Municipality 14 RCB Probable Beneficiary 3 2 RS 987105 9935600 Umakanta Sapkota G-45-1-5-0-0001 Umakanta Sapkota Baglung Baglung Urban Municipality 5 RCB Probable Beneficiary 4 2 RS 987014 9825919 Janaki Sarkini G-45-1-12-0-0012 Janaki Sarkini Baglung Baglung Urban Municipality 12 RCB Probable Beneficiary 5 2 RS 987004 9824704 Parbati Sunar G-45-6-4-0-0001 Parbati Sunar Baglung Kathekhola Rural Municipality 4 RCB Probable Beneficiary 6 2 RS 987012 9824712 Top Bahadur Pun G-45-6-4-0-0002 Top Bahadur Pun Baglung Kathekhola Rural Municipality 4 RCB Probable Beneficiary 7 2 RS 987007 9825846 Dil Bahadur Kami G-45-7-1-0-0001 Dil Bahadur Kami Baglung Tamankhola Rural Municipality 1 RCB Probable Beneficiary 8 2 RV 383437 1308742Madan Bahadur RanamagarR-10-4-1-5-0001 Madan Bdr Rana Magar Bhojpur Ramprasadrai Rural Municipality 1 RTB Retrofit Beneficiary 9 2 RS 383157 9885107 Hemraj Rai R-10-3-6-2-0002 Hemraj Rai Bhojpur Tyamkemaiyum Rural Municipality 6 RTB Retrofit Beneficiary 10 2 RV 987004 9885137 Tek Bahadur Rai R-10-3-6-2-0003 Tek Bahadur Rai Bhojpur Tyamkemaiyum Rural Municipality 6 RTB Retrofit Beneficiary 11 2 RV 987004 9884907 Yashoda Basneth R-10-3-9-2-0001 Yashoda Basneth Bhojpur Tyamkemaiyum Rural -

Knowledge, Power and Policy the Case of Agricultural Development in Dhading District, Nepal
Knowledge, power and policy The case of agricultural development in Dhading District, Nepal Gopi Krishna Sedhain, Ajay B Mathema, Nawang Sherpa, and Binay B Adhikari Country Report Food and agriculture Keywords: November 2014 Agricultural policies, Knowledge, Evidence, Sustainable intensification, Political economy analysis About the authors Dr Gopi Krishna Sedhain, Senior Agriculture Consultant Ajay Bakta Mathema, Team Leader, Director, Asian Center for Environment Management and Sustainable Development (AEMS), [email protected] Nawang Sherpa, Program Officer, AEMS Binay B Adhikari, Research Coordinator, AEMS Produced by IIED’s Natural Resources Group The aim of the Natural Resources Group is to build partnerships, capacity and wise decision-making for fair and sustainable use of natural resources. Our priority in pursuing this purpose is on local control and management of natural resources and other ecosystems. Partner organisation The mission of AEMS (Asian Centre for Environment Management and Sustainable Development) is to establish a functional partnership among the countries of Asia having common environmental issues of development, and to ensure sharing of knowledge and technology. Its main objectives are (1) to carry out research activities on present day environmental degradation and its impacts, (2) to provide consulting services and to carry out trainings, seminars and workshops in national as well as international levels to address the issues of environmental concerns; (3) to carry out development and construction works regarding management of the environment and sustainability in development, (4) to establish national and international cooperation with educational institutions like universities involved in environmental management, and (5) to establish a resource center providing information on environmental and development programmes and projects. -
Written Examination for the Position of Trainee Assistant
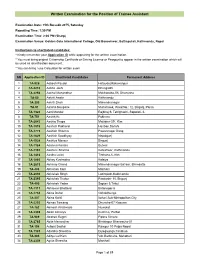
Written Examination for the Position of Trainee Assistant Examination Date: 15th Baisakh 2075, Saturday Reporting Time: 1:30 PM Examination Time: 2:00 PM (Sharp) Examination Venue: Golden Gate International College, Old Baneshwor, Battisputali, Kathmandu, Nepal Instructions to shortlisted candidates: * Kindly remember your Application ID while appearing for the written examination. * You must bring original Citizenship Certificate or Driving License or Passport to appear in the written examination which will be used as identification document. * You can bring / use Calculator for written exam. SN Application ID Shortlisted Candidates Permanent Address 1 TA-926 Aabesh Paudel Hetauda,Makawanpur 2 TA-2210 Aabha Joshi Dhangadhi 3 TA-2254 Aachal Manandhar Makhanaha-08, Dhanusha 4 TA-60 Aakriti Awale Kathmandu 5 TA-303 Aakriti Shah Mahendranagar 6 TA-51 Aalisha Neupane Murlichowk, Ward No.: 12, Birgunj, Parsa 7 TA-1320 Aarti Mandal Rajbiraj-9, Tetrighachi, Sapatari- 6. 8 TA-751 Aashik Kc Pokhara 9 TA-2643 Aashiq Thapa Maitidevi-29 , Ktm 10 TA-1919 Aashish Pokharel Hariban,Sarlahi 11 TA-1775 Aashish Sharma Pawannagar Dang 12 TA-1629 Aashish Upadhyay Nepalgunj 13 TA-1924 Aashiya Mansur Birgunj 14 TA-1184 Aashma Koirala Butwal 15 TA-1191 Aashree Sharma Koteshwor, Kathmandu 16 TA-1416 Aastha Luitel Tinthana-6, Ktm 17 TA-1880 Abhay Kushwaha Kalaiya 18 TA-2619 Abhinay Chand Mahendranagar Bazaar, Bhimdatta 19 TA-408 Abhishek Karn Matihani 20 TA-2030 Abhishek Singh Lazimpath,Kathmandu 21 TA-2395 Abhishek Thakur Panitanki- 10, Birgunj 22 TA-490 Abhishek -

English Grammar & Composition
DYNAMIC ENGLISH GRAMMAR & COMPOSITION 10 Author Krishna Prasad Regmi Edited by Koushalya Gurung Publisher Shubharambha Publication Pvt. Ltd. Kathmandu, Nepal This book belongs to: Name: .............................................................................. Class: ............................................................................... Roll Number: ............................................................................... Address: .............................................................................. Contact Number: ............................................................................... Author : Krishna Prasad Regmi Layout Design : Ram Malakar Copyright © : Publisher New Edition : 2075 Revised Edition: 2077 Publication : Shubharambha Publication Pvt. Ltd. Kathmandu, Nepal Preface Dynamic English Grammar and Composition has been designed according to the new English Curriculum prescribed by the Curriculum Development Centre. The series comprises of ten textbooks from grade one to grade ten. The present book is an amalgamation of survey of rules, structures and forms presented in lucid modern English and illustrated with numerous examples. The aim of this book is to bring about a change in teaching and learning English grammar and composition-a change that will enable the learners to use grammar in context using both inductive and deductive approaches aiming to develop four language skills immensely. Practice in composition tasks will help to develop the learner’s writing skills. It will encourage to writing