Spinal Fractures Classification System an Aospine Knowledge Forum Initiative
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Disability Classification System
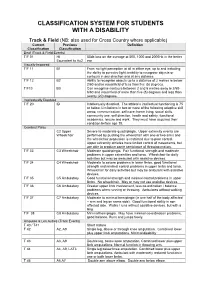
CLASSIFICATION SYSTEM FOR STUDENTS WITH A DISABILITY Track & Field (NB: also used for Cross Country where applicable) Current Previous Definition Classification Classification Deaf (Track & Field Events) T/F 01 HI 55db loss on the average at 500, 1000 and 2000Hz in the better Equivalent to Au2 ear Visually Impaired T/F 11 B1 From no light perception at all in either eye, up to and including the ability to perceive light; inability to recognise objects or contours in any direction and at any distance. T/F 12 B2 Ability to recognise objects up to a distance of 2 metres ie below 2/60 and/or visual field of less than five (5) degrees. T/F13 B3 Can recognise contours between 2 and 6 metres away ie 2/60- 6/60 and visual field of more than five (5) degrees and less than twenty (20) degrees. Intellectually Disabled T/F 20 ID Intellectually disabled. The athlete’s intellectual functioning is 75 or below. Limitations in two or more of the following adaptive skill areas; communication, self-care; home living, social skills, community use, self direction, health and safety, functional academics, leisure and work. They must have acquired their condition before age 18. Cerebral Palsy C2 Upper Severe to moderate quadriplegia. Upper extremity events are Wheelchair performed by pushing the wheelchair with one or two arms and the wheelchair propulsion is restricted due to poor control. Upper extremity athletes have limited control of movements, but are able to produce some semblance of throwing motion. T/F 33 C3 Wheelchair Moderate quadriplegia. Fair functional strength and moderate problems in upper extremities and torso. -
IPC Accessibility Guide
2 TABLE OF CONTENTS FIGURES AND TABLES ................................................................................................................. 8 Foreword ........................................................................................................................................... 10 Introduction ................................................................................................................................. 10 Evolving content ......................................................................................................................... 10 Disclosure ...................................................................................................................................... 11 Structure and content of the IPC Accessibility Guide ...................................................... 11 Content ........................................................................................................................................... 11 Executive summary ......................................................................................................................... 12 Aim and purpose of the Guide ................................................................................................ 12 Key objectives of the Guide ..................................................................................................... 12 Target audience of the Guide ................................................................................................. 12 1 General information -

2018 Jessica Uniack Beach to Bay Race Long Beach Yacht Club
2018 Jessica Uniack Beach to Bay Race Long Beach Yacht Club Results for 2018 Jessica Uniack Beach to Bay Race CFJ Class Sailed: 1, Discards: 0, To count: 1, Entries: 25, Scoring system: Appendix A Class SailNo Club HelmName CrewName R1 Total Nett CFJ HHSF Jack Haliday Nicholas Ridout CFJ HHSF Trae Sanchez Ben Hagadorn CFJ LBYC 7 LBYC Nicky Lech Kai Bramble 1.0 1.0 1.0 CFJ 22 ABYC Nicholas Muller Ulises Lewis 2.0 2.0 2.0 CFJ LBYC 10 LBYC Preston Woodworth Alex Lech 3.0 3.0 3.0 CFJ 43 ABYC Summer Drake Paige Odell 4.0 4.0 4.0 CFJ 23 ABYC Nikhil Stewart Jamarcus Parker 5.0 5.0 5.0 CFJ 42 ABYC Sean colley Thomas Dobson 6.0 6.0 6.0 CFJ 44 ABYC Nicolas Sanchez Nicole Morikawa 7.0 7.0 7.0 CFJ 24 ?? 8.0 8.0 8.0 CFJ 0 HHSF Trae Sanchez Ben H 9.0 9.0 9.0 CFJ LBYC 2 LBYC Kyer Fox Isaure Chalandon 10.0 10.0 10.0 CFJ LBYC 9 LBYC Sawyer Bambam-Moak Katin Cathey 11.0 11.0 11.0 Class SailNo Club HelmName CrewName R1 Total Nett CFJ 46 ABYC Elisabeth Rossbach Troy Davidson 12.0 12.0 12.0 CFJ 00 HHSF Jack Haliday Nicholas 13.0 13.0 13.0 CFJ 41 ABYC Michael Colley Emilia Anctil 14.0 14.0 14.0 CFJ 6161 DPYC Riley Lenthall 15.0 15.0 15.0 CFJ 9PYSF HHYC Jack Busche Nolan Davis 16.0 16.0 16.0 CFJ 1510 DPYC Ryan Brown Colin Sekerka 17.0 17.0 17.0 CFJ 5151 DPYC Christopher Andersen Hunter Laws 18.0 18.0 18.0 CFJ LBYC 3 LBYC Luke Bramble Rio Dumont 19.0 19.0 19.0 CFJ LBYC 5 LBYC Jack Snow Reese Lapham 26.0 DSQ 26.0 26.0 CFJ 6161 DPYC Carsen Lenthall 26.0 DNC 26.0 26.0 CFJ 6161 DPYC Riley Lenthall 26.0 DNC 26.0 26.0 CFJ 5151 DPYC Hunter Laws Christopher Anderson -

Decision Tree Learning– Solution
Decision Tree Learning{ Solution 1) Assume that you have the following training examples available: F1 F2 F3 F4 F5 Class Example 1 t t f f f p Example 2 f f t t f p Example 3 t f f t f p Example 4 t f t f t p Example 5 f t f f f n Example 6 t t f t t n Example 7 f t t t t n Use all of the training examples to construct a decision tree. In case of ties between features, break ties in favor of features with smaller numbers (for ex- ample, favor F1 over F2, F2 over F3, and so on). How does the resulting decision tree classify the following example: F1 F2 F3 F4 F5 Class Example 8 f f f t t ? Answer: Let H(x; y) denote the entropy of a data set with x examples belonging to class p and y examples belonging to class n. That is, x x y y H(x; y) = − log − log : x + y 2 x + y x + y 2 x + y We precompute the values for some H(x; y), which will be useful when con- structing the decision tree. H(0; x) = H(x; 0) = −1 log2 1 − 0 log2 0 = 0 H(x; x) = −(1=2) log2 (1=2) − (1=2) log2 (1=2) = 1 H(1; 2) = H(2; 1) = −(1=3) log2 (1=3) − (2=3) log2 (2=3) = 0:918 H(1; 3) = H(3; 1) = −(1=4) log2 (1=4) − (3=4) log2 (3=4) = 0:811 First, we choose from f F1, F2, F3, F4, F5 g to become the root. -
Ifds Functional Classification System & Procedures
IFDS FUNCTIONAL CLASSIFICATION SYSTEM & PROCEDURES MANUAL 2009 - 2012 Effective – 1 January 2009 Originally Published – March 2009 IFDS, C/o ISAF UK Ltd, Ariadne House, Town Quay, Southampton, Hampshire, SO14 2AQ, GREAT BRITAIN Tel. +44 2380 635111 Fax. +44 2380 635789 Email: [email protected] Web: www.sailing.org/disabled 1 Contents Page Introduction 5 Part A – Functional Classification System Rules for Sailors A1 General Overview and Sailor Evaluation 6 A1.1 Purpose 6 A1.2 Sailing Functions 6 A1.3 Ranking of Functional Limitations 6 A1.4 Eligibility for Competition 6 A1.5 Minimum Disability 7 A2 IFDS Class and Status 8 A2.1 Class 8 A2.2 Class Status 8 A2.3 Master List 10 A3 Classification Procedure 10 A3.0 Classification Administration Fee 10 A3.1 Personal Assistive Devices 10 A3.2 Medical Documentation 11 A3.3 Sailors’ Responsibility for Classification Evaluation 11 A3.4 Sailor Presentation for Classification Evaluation 12 A3.5 Method of Assessment 12 A3.6 Deciding the Class 14 A4 Failure to attend/Non Co-operation/Misrepresentation 16 A4.1 Sailor Failure to Attend Evaluation 16 A4.2 Non Co-operation during Evaluation 16 A4.3 International Misrepresentation of Skills and/or Abilities 17 A4.4 Consequences for Sailor Support Personnel 18 A4.5 Consequences for Teams 18 A5 Specific Rules for Boat Classes 18 A5.1 Paralympic Boat Classes 18 A5.2 Non-Paralympic Boat Classes 19 Part B – Protest and Appeals B1 Protest 20 B1.1 General Principles 20 B1.2 Class Status and Protest Opportunities 21 B1.3 Parties who may submit a Classification Protest -

What Are We Doing with (Or To) the F-Scale?
5.6 What Are We Doing with (or to) the F-Scale? Daniel McCarthy, Joseph Schaefer and Roger Edwards NOAA/NWS Storm Prediction Center Norman, OK 1. Introduction Dr. T. Theodore Fujita developed the F- Scale, or Fujita Scale, in 1971 to provide a way to compare mesoscale windstorms by estimating the wind speed in hurricanes or tornadoes through an evaluation of the observed damage (Fujita 1971). Fujita grouped wind damage into six categories of increasing devastation (F0 through F5). Then for each damage class, he estimated the wind speed range capable of causing the damage. When deriving the scale, Fujita cunningly bridged the speeds between the Beaufort Scale (Huler 2005) used to estimate wind speeds through hurricane intensity and the Mach scale for near sonic speed winds. Fujita developed the following equation to estimate the wind speed associated with the damage produced by a tornado: Figure 1: Fujita's plot of how the F-Scale V = 14.1(F+2)3/2 connects with the Beaufort Scale and Mach number. From Fujita’s SMRP No. 91, 1971. where V is the speed in miles per hour, and F is the F-category of the damage. This Amazingly, the University of Oklahoma equation led to the graph devised by Fujita Doppler-On-Wheels measured up to 318 in Figure 1. mph flow some tens of meters above the ground in this tornado (Burgess et. al, 2002). Fujita and his staff used this scale to map out and analyze 148 tornadoes in the Super 2. Early Applications Tornado Outbreak of 3-4 April 1974. -

Reframing Sport Contexts: Labeling, Identities, and Social Justice
Reframing Sport Contexts: Labeling, Identities, and Social Justice Dr. Ted Fay and Eli Wolff Sport in Society Disability in Sport Initiative Northeastern University Critical Context • Marginalization (Current Status Quo) vs. • Legitimatization (New Inclusive Paradigm) Critical Context Naturalism vs. Trans-Humanism (Wolbring, G. (2009) How Do We Handle Our Differences related to Labeling Language and Cultural Identities? • Stereotyping? • Prejudice? • Discrimination? (Carr-Ruffino, 2003, p. 1) Ten Major Cultural Differences 1) Source of Control 2) Collectivism or Individualism 3) Homogeneous or Heterogeneous 4) Feminine or Masculine 5) Rank Status 6) Risk orientation 7) Time use 8) Space use 9) Communication Style 10) Economic System (Carr – Ruffino, 2003, p.27) Rationale for Inclusion • Divisioning by classification relative to “fair play” and equity principles • Sport model rather than “ism” segregated model (e.g., by race, gender, disability, socio-economic class, sexual orientation, look (body image), sect (religion), age) • Legitimacy • Human rights and equality Social Dynamics of Inequality Reinforce and reproduce Social Institutions Ideology Political (Patriarchy) Economic Educational Perpetuates Religious Prejudice & Are institutionalized by Discrimination Cultural Practices (ISM) Sport Music Art (Sage, 1998) Five Interlinking Conceptual Frameworks • Critical Change Factors Model (CCFM) • Organizational Continuum in Sport Governance (OCSG) • Criteria for Inclusion in Sport Organizations (CISO) • Individual Multiple Identity Sport Classifications Index (IMISCI) • Sport Opportunity Spectrum (SOS) Critical Change Factors Model (CCFM) F1) Change/occurrence of major societal event (s) affecting public opinion toward ID group. F2) Change in laws, government and court action in changing public policies toward ID group. F3) Change in level of influence of high profile ID group role models on public opinion. -

Marelli D6C & D5C ATEX Motor Technical Catalogue
Motors for This catalogue refers to ATEX Motors belonging to Group I Category M2 and Group II Category 2G, 2D, 2GD as described. STANDARDS ® BEARINGS Hazardous Areas The ATEX Motors described in this catalogue are manufactured in accordance with IEC 60034-1-5-6-7-8-9-12-14, IEC 60072-1, EN 50347, EN 60079- D5, D6 SERIES Frame Size (mm) D - end N - end Frame Size Poles B 3 V 1 MarelliMotori 0-1-7, EN 61241-0-1. 71* 6202-2Z 6202-2Z D - end N - end D - end N - end I M2, II 2G, II 2D EUROPEAN DIRECTIVES 355-400 2 6217-C3 6217-C3 6217-C3 7217 B 80* 6204-2Z 6204-2Z Ex d/de I, Ex d/de IIB, Ex tD A21 IP65 Title Directive 90* 6205-2Z 6205-2Z 355 4 NU222-C3 6217-C3 NU222-C3 6217-C3 + 7217 B Equipment and protective system intended for use in potentially explosive atmospheres (ATEX) 94/9/EC 100* 6206-2Z 6206-2Z 400 4 NU222-C3 6222-C3 NU222-C3 6222-C3 + 7222 B Electromagnetic Compatibility (EMC) 2004/108/IEC 112* 6206-2Z 6206-2Z Low Voltage Directive (LVD) 2006/95/EC 132* 6308-2Z 6308-2Z HEADQUARTERS ITALIAN OFFICES Machinery Directive (MD) 98/37/EC 160 - 180M 6310-Z-C3 6209-Z-C3 Marelli Motori S.p.A. Milan CERTIFICATES 180L 6310-Z-C3 6210-Z-C3 Via Sabbionara, 1 Via Cesare Cantù, 29 200 6312-Z-C3 6210-Z-C3 Frame size Number Temperature Limits 36071 Arzignano (VI) Italy 20092 Cinisello Balsamo (MI) Italy 225 6313-Z-C3 6213-Z-C3 71-132 BVI 08 ATEX 0001 -20°C +40°C* 160-315 CESI 02 ATEX 071 -20 C +40 C* 250 6314-Z-C3 6213-Z-C3 (T) +39.0444.479711 (T) +39.02.660.131.66 ° ° These tables describe the bearing types used in standard configurations. -
World Para Nordic Skiing WC Points Winter Season 2019/20
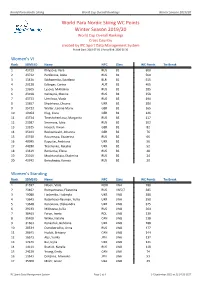
World Para Nordic Skiing World Cup Overall Rankings Winter Season 2019/20 World Para Nordic Skiing WC Points Winter Season 2019/20 World Cup Overall Rankings Cross Country created by IPC Sport Data Management System Period Start: 2019-07-01 | Period End: 2020-06-30 Women's VI Rank SDMS ID Name NPC Class WC Points Tie Break 1 43739 Khlyzova, Vera RUS B2 600 2 43732 Panferova, Anna RUS B2 560 3 13436 Sakhanenka, Sviatlana BLR B2 515 4 29128 Edlinger, Carina AUT B1 405 5 13605 Lysova, Mikhalina RUS B2 285 6 23918 Galitsyna, Marina RUS B1 258 7 43733 Umrilova, Vlada RUS B3 190 8 13657 Shyshkova, Oksana UKR B2 180 9 35723 Walter, Leonie Maria GER B2 165 10 19064 Klug, Clara GER B1 126 11 43734 Tereshchenkova, Margarita RUS B3 117 12 23987 Smirnova, Iuliia RUS B2 102 13 13525 Hoesch, Vivian GER B1 82 14 35103 Recktenwald, Johanna GER B2 76 15 43740 Razumnaia, Ekaterina RUS B2 66 16 40995 Kapustei, Andriana UKR B2 56 17 44280 Tkachenko, Nataliia UKR B2 52 18 13619 Remizova, Elena RUS B3 48 19 23919 Moshkovskaia, Ekaterina RUS B2 24 20 43742 Berezhnaia, Kseniia RUS B2 20 Women's Standing Rank SDMS ID Name NPC Class WC Points Tie Break 1 31597 Nilsen, Vilde NOR LW4 780 2 23402 Rumyantseva, Ekaterina RUS LW5/7 385 3 19080 Liashenko, Liudmyla UKR LW8 380 4 13643 Batenkova-Bauman, Yuliia UKR LW6 350 5 13648 Kononova, Oleksandra UKR LW8 325 6 29233 Mikheeva, Iuliia RUS LW8 264 7 30463 Faron, Iweta POL LW8 239 8 35400 Wilkie, Natalie CAN LW8 238 9 31663 Konashuk, Bohdana UKR LW8 188 10 20534 Ostroborodko, Anna RUS LW8 177 11 20641 Hudak, Brittany CAN -

A. Legal Permanent Resident Aliens
A. Classes Currently in Use - Legal Permanent Resident Aliens (continued) Symbol: *Arrival/ Statistical Document Adjust Section of Law Description FY AM1 AM-1 N Sec. 584(b)(1)(A) of Amerasian born in AM6 AM-6 A PL 100-202 Vietnam after (Dec. 22, 1987) Jan. 1, 1962 and before Jan. 1, 1976 who was fathered by a U.S. citizen. AM2 AM-2 N Sec. 584(b)(1)(B) of Spouse or child of an AM7 AM-7 A PL 100-202 alien classified as (Dec. 22, 1987) AM1 or AM6. AM3 AM-3 N Sec. 584(b)(1)(C) of Mother, guardian, or AM8 AM-8 A PL 100-202 next-of-kin of an (Dec. 22, 1987) alien classified as AM1 or AM6, and spouse or child of the mother, guardian, or next-of-kin. AR1 AR-1 N Sec. 201(b)(2)(A)(i) Amerasian child of a AR6 AR-6 A of the I&N Act and U.S. citizen born in 204(g) as added by Cambodia, Korea, PL 97-359 (Oct. 22, Laos, Thailand, or 1982) Vietnam (immediate relative child). AS6 AS-6 A Sec. 209(b) of the Asylee principal I&N Act as added by PL 96-212 (Mar. 17, 1980) AS7 AS-7 A Sec. 209(b) of the Spouse of an alien I&N Act as added by classified as AS6. PL 96-212 (Mar. 17, 1980) AS8 AS-8 A Sec. 209(b) of the Child of an alien I&N Act as added by classified as AS6. -

Connexion Client Cataloging Quick Reference
OCLC Connexion Client Cataloging Quick Reference Introduction Keystroke shortcuts The Connexion client is a Windows-based interface to OCLC • Use default keystroke shortcuts or assign your own to activate Connexion® used to access WorldCat for cataloging. commands, insert characters, run macros, and insert text strings. This quick reference provides brief instructions for editing, saving, • View key assignments in View > Assigned Keys.To print or copy exporting, and printing labels for bibliographic records; using local files; the list, click Print or Copy to Clipboard. creating and adding records to WorldCat; replacing WorldCat records; Tip: Before printing, click a column heading to sort the list by data batch processing; and cataloging with non-Latin scripts. in the column. • Assign your own keystrokes in Tools > Keymaps. Multiscript support: The client supports the following non-Latin scripts: • Print a function key template to put at the top of your keyboard: Arabic, Armenian, Bengali, Chinese, Cyrillic, Devanagari, Ethiopic, Greek, Hebrew, Japanese, Korean, Syriac, Tamil, and Thai. www.oclc.org/support/documentation/connexion/client/ gettingstarted/keyboardtemplate.pdf. This quick reference does not cover instructions for authorities work or instructions already available in: Toolbar • Getting Started with Connexion Client • The client installs with three toolbars displayed by default: • Connexion Client Setup Worksheet o Main client toolbar (with command-equivalent buttons) • Connexion: Searching WorldCat Quick Reference o WorldCat quick search tool Quick tools for text strings and user tools Connexion client documentation assumes knowledge of MARC o cataloging. • Customize the main client toolbar: In Tools > Toolbar Editor, drag and drop buttons to add or remove, or reset to the default. -

World Para Alpine Skiing WC Points Winter Season 2020/21
World Para Alpine Skiing World Cup Individual Rankings Winter Season 2020/21 World Para Alpine Skiing WC Points Winter Season 2020/21 World Cup Individual Rankings created by IPC Sport Data Management System Period Start: 2020-07-01 | Period End: 2021-06-30 Women's Slalom VI Rank SDMS ID Name NPC Class WC Points Tie Break 1 23842 Ristau, Noemi Ewa GER B2 220 2 22142 Aigner, Veronika AUT B2 200 3 40290 Aigner, Barbara AUT B3 180 4 44235 Rexova, Alexandra SVK B2 160 5 31601 Bennink, Maaike NED B2 60 6 13349 Farkasova, Henrieta SVK B3 50 Women's Slalom Standing Rank SDMS ID Name NPC Class WC Points Tie Break 1 29162 Rieder, Anna-Maria GER LW9-1 260 2 13162 Rothfuss, Andrea GER LW6/8-2 210 3 29136 Voronchikhina, Varvara RUS LW6/8-2 180 4 13116 Bochet, Marie FRA LW6/8-2 140 5 24067 Smetisko, Lucija CRO LW6/8-2 120 6 41102 Aarsjoe, Ebba SWE LW4 100 7 14585 Khorosheva, Anastasiia RUS LW9-2 50 8 42372 Richard, Aurelie FRA LW6/8-2 45 Women's Slalom Sitting Rank SDMS ID Name NPC Class WC Points Tie Break 1 13161 Forster, Anna-Lena GER LW12-1 400 2 21797 van Bergen, Barbara NED LW11 80 Men's Slalom VI Rank SDMS ID Name NPC Class WC Points Tie Break 1 13724 Deleplace, Hyacinthe FRA B2 230 2 20881 Bertagnolli, Giacomo ITA B3 200 24.30 (§302.3) 3 35366 Simpson, Neil GBR B3 200 35.60 (§302.3) 4= 40291 Aigner, Johannes AUT B2 160 4= 13338 Krako, Jakub SVK B2 160 6 13335 Haraus, Miroslav SVK B2 105 7 44167 Scharnagl, Michael AUT B3 100 IPC Sport Data Management System Page 1 of 7 26 September 2021 at 01:38:04 CEST World Para Alpine Skiing World Cup Individual