Bladder Carcinoma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bladder Cancer
Clinical Practice in Urology Series Editor: Geoffrey D. Chisholm Titles in the series already published Urinary Diversion Edited by Michael Handley Ashken Chemotherapy and Urological Malignancy Edited by A. S. D. Spiers Urodynamics Paul Abrams, Roger Feneley and Michael Torrens Male Infertility Edited by T. B. Hargreave The Pharmacology of the Urinary Tract Edited by M. Caine Forthcoming titles in the series Urological Prostheses, Appliances and Catheters Edited by J. P. Pryor Percutaneous and Interventional Uroradiology Edited by Erich K. Lang Adenocarcinoma of the Prostate Edited by Andrew W. Bruce and John Trachtenberg Bladder Cancer Edited by E. J. Zingg and D. M. A. Wallace With 50 Figures Springer-Verlag Berlin Heidelberg New York Tokyo E. J. Zingg, MD Professor and Chairman, Department of Urology, Univ~rsity of Berne, Inselspital, 3010 Berne, Switzerland D. M. A. Wallace, FRCS Consultant Urologist, Department of Urology, Queen Elizabeth Medical Centre, Birmingham, England Series Editor Geoffrey D. Chisholm, ChM, FRCS, FRCSEd Professor of Surgery, University of Edinburgh; Consultant Urological Surgeon, Western General Hospital, Edinburgh, Scotland ISBN -13: 978-1-4471-1364-5 e-ISBN -13: 978-1-4471-1362-1 DOI: 10.1007/978-1-4471-1362-1 Library of Congress Cataloging in Publication Data Main entry under title: Bladder Cancer (Clinical Practice in Urology) Includes bibliographies and index. 1. Bladder - Cancer. I. Zingg, Ernst J. II. Wallace, D.M.A. (David Michael Alexander), 1946- DNLM: 1. Bladder Neoplasms. WJ 504 B6313 RC280.B5B632 1985 616.99'462 85-2572 ISBN-13:978-1-4471-1364-5 (U.S.) This work is subject to copyright. -

A Comprehensive Review of a Rare Subclass of Mucosal Melanoma with Emphasis on Differential Diagnosis and Therapeutic Approaches
cancers Review Urological Melanoma: A Comprehensive Review of a Rare Subclass of Mucosal Melanoma with Emphasis on Differential Diagnosis and Therapeutic Approaches Gerardo Cazzato 1,*,† , Anna Colagrande 1,†, Antonietta Cimmino 1, Concetta Caporusso 1, Pragnell Mary Victoria Candance 1, Senia Maria Rosaria Trabucco 1, Marcello Zingarelli 2, Alfonso Lorusso 2, Maricla Marrone 3 , Alessandra Stellacci 3 , Francesca Arezzo 4, Andrea Marzullo 1, Gabriella Serio 1, Angela Filoni 5, Domenico Bonamonte 5, Paolo Romita 5, Caterina Foti 5, Teresa Lettini 1 , Vera Loizzi 4, Gennaro Cormio 4 , Leonardo Resta 1 , Roberta Rossi 1,‡ and Giuseppe Ingravallo 1,‡ 1 Section of Pathology, Department of Emergency and Organ Transplantation (DETO), University of Bari “Aldo Moro”, 70124 Bari, Italy; [email protected] (A.C.); [email protected] (A.C.); [email protected] (C.C.); [email protected] (P.M.V.C.); [email protected] (S.M.R.T.); [email protected] (A.M.); [email protected] (G.S.); [email protected] (T.L.); [email protected] (L.R.); [email protected] (R.R.); [email protected] (G.I.) 2 Section of Urology, Deparment of Emergency and Organ Transplantation (DETO), University of Bari “Aldo Moro”, 70124 Bari, Italy; [email protected] (M.Z.); [email protected] (A.L.) 3 Section of Legal Medicine, Interdisciplinary Department of Medicine, Bari Policlinico Hospital, Citation: Cazzato, G.; Colagrande, University of Bari Aldo Moro, Piazza Giulio Cesare 11, 70124 Bari, Italy; [email protected] (M.M.); A.; Cimmino, A.; Caporusso, C.; [email protected] (A.S.) Candance, P.M.V.; Trabucco, S.M.R.; 4 Section of Ginecology and Obstetrics, Department of Biomedical Sciences and Human Oncology, Zingarelli, M.; Lorusso, A.; Marrone, University of Bari Aldo Moro, Piazza Giulio Cesare 11, 70124 Bari, Italy; [email protected] (F.A.); M.; Stellacci, A.; et al. -

Quality of Life Outcomes After Brachytherapy for Early Prostate Cancer
Prostate Cancer and Prostatic Diseases (1999) 2 Suppl 3, S19±S20 ß 1999 Stockton Press All rights reserved 1365±7852/99 $15.00 http://www.stockton-press.co.uk/pcan Quality of life outcomes after brachytherapy for early prostate cancer MS Litwin1, JM Brandeis1, CM Burnison1 and E Reiter1 1UCLA Departments of Urology, Health Services, and Radiation Oncology, UCLA, California, USA Despite the absence of empirical evidence, there is a XRT. Sildena®l appeared to have little effect in the radical popular perception that brachytherapy results in less prostatectomy patients. However, brachytherapy patients impairment of health-related quality of life. This study not receiving hormonal ablation or XRT who took silde- compared general and disease-speci®c health-related na®l had better sexual function and bother scores than quality of life in men who had undergone either brachy- those patients who did not. therapy (with and without pre-treatment XRT) or radical prostatectomy, and in healthy age-matched controls. Method Conclusion We surveyed all patients with clinical T2 or less prostate General health-related quality of life did not differ greatly cancer who had undergone interstitial seed brachyther- between the three groups, but there were variations in apy at UCLA during the previous 3±17 months. Each was disease-speci®c (urinary, bowel and sexual) health-related paired with two randomly selected, temporally matched quality of life. Radical prostatectomy patients had the radical prostatectomy patients. Healthy, age-matched worst urinary function (leakage), but brachytherapy controls were drawn from the literature. Surgery and patients were also signi®cantly worse than the controls. -

Prostate Biopsy in the Staging of Prostate Cancer
Prostate Cancer and Prostatic Diseases (1997) 1, 54±58 ß 1997 Stockton Press All rights reserved 1365±7852/97 $12.00 Review Prostate Biopsy in the staging of prostate cancer L Salomon, M Colombel, J-J Patard, D Gasman, D Chopin & C-C Abbou Service d'Urologie, CHU, Henri Mondor, CreÂteil, France The use of prostate biopsies was developed in parallel with progress in our knowledge of prostate cancer and the use of prostate-speci®c antigen (PSA). Prostate biopsies were initially indicated for the diagnosis of cancer, by the perineal approach under general anesthesia. Nowadays prostate biopsies are not only for diagnostic purposes but also to determine the prognosis, particularly before radical prostatectomy. They are performed in patients with elevated PSA levels, by the endorectal approach, sometimes under local anesthesia.(1±3) The gold standard is the sextant biopsy technique described by Hodge4,5, which is best to diagnose prostate cancer, particularly in case of T1c disease (patients with serum PSA elevation).6±13 Patients with a strong suspicion of prostate cancer from a negative series of biopsies can undergo a second series14;15 with transition zone biopsy16,17 or lateral biopsy.18,19 Karakiewicz et al 20 and Uzzo et al 21 proposed that the number of prostate biopsies should depend on prostate volume to improve the positivity rate. After the diagnosis of prostate cancer, initial therapy will depend on several prognostic factors. In the case of radical prostatectomy, the results of sextant biopsy provide a wealth of information.22,23 The aim of this report is to present the information given by prostate biopsy in the staging of prostate cancer. -

Needle Biopsy and Radical Prostatectomy Specimens David J Grignon
Modern Pathology (2018) 31, S96–S109 S96 © 2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 Prostate cancer reporting and staging: needle biopsy and radical prostatectomy specimens David J Grignon Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, IUH Pathology Laboratory, Indianapolis, IN, USA Prostatic adenocarcinoma remains the most common cancer affecting men. A substantial majority of patients have the diagnosis made on thin needle biopsies, most often in the absence of a palpable abnormality. Treatment choices ranging from surveillance to radical prostatectomy or radiation therapy are largely driven by the pathologic findings in the biopsy specimen. The first part of this review focuses on important morphologic parameters in needle biopsy specimens that are not covered in the accompanying articles. This includes tumor quantification as well as other parameters such a extraprostatic extension, seminal vesicle invasion, perineural invasion, and lymphovascular invasion. For those men who undergo radical prostatectomy, pathologic stage and other parameters are critical in prognostication and in determining the appropriateness of adjuvant therapy. Staging parameters, including extraprostatic extension, seminal vesicle invasion, and lymph node status are discussed here. Surgical margin status is also an important parameter and definitions and reporting of this feature are detailed. Throughout the article the current reporting guidelines published by the College of American Pathologists and the International Collaboration on Cancer Reporting are highlighted. Modern Pathology (2018) 31, S96–S109; doi:10.1038/modpathol.2017.167 The morphologic aspects of prostatic adenocarcinoma hormonal therapy.4,5 For needle biopsy specimens the have a critical role in the management and prognos- data described below are largely based on standard tication of patients with prostatic adenocarcinoma. -

Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis
www.kjurology.org DOI:10.4111/kju.2010.51.1.70 Case Report Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis Kyung Hwa Choi, Seung Hwan Lee, Won Sug Jung1, Byung Ha Chung Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, 1National Health Insurance Corporation Ilsan Hospital, Goyang, Korea We report a rare case of robot-assisted laparoscopic radical prostatectomy (RARP) in Article History: a patient with a preexisting penile prosthesis. In this case, we completed RARP without received 27 August, 2009 14 October, 2009 removing the reservoir by using a deflation-inflation technique, and there were no com- accepted plications related to the prosthesis. The patient had a negative surgical margin. The Corresponding Author: preserved three-piece inflatable penile prosthesis continued to function properly in 1 Byung Ha Chung month. Reservoir-preserving RARP is technically feasible and safe. However, it is im- Department of Urology, Yonsei portant to be aware of device-related complications. Long-term studies on the mechan- University Health System, Gangnam Severance Hospital, 712, Eonju-ro, ical survival rate and patient satisfaction should be also performed. Dogok-dong, Gangnam-gu, Seoul Key Words: Robotics, Prostatectomy, Penile prosthesis, Prostatic neoplasms 135-720, Korea TEL: +82-2-2019-3474 FAX: +82-2-3462-8887 E-mail: [email protected] Prostate cancer has been reported to occur most frequently CASE REPORT in men over 40 years of age. In organ-confined cases, radical prostatectomy is the treatment of choice. After the in- 1. Patient troduction of the da VinciⓇ surgical system (Intuitive The patient was a 64-year-old male diagnosed with aci- Surgical, Sunnyvale, USA), robot-assisted laparoscopic nar-type prostate adenocarcinoma with a Gleason score of radical prostatectomy (RARP) has become a mainstay of 6 (3+3) by prostate biopsy. -

Invasive Bladder Cancer After Cyclophosphamide Administration for N Ephrotic Syndrome- a Case Report
121 Hiroshima J. Med. Sci. Vol. 49, No. 2, 121-123, June, 2000 HIJM49-18 Invasive Bladder Cancer after Cyclophosphamide Administration for N ephrotic Syndrome- A Case Report Takahisa NAKAMOTO, Yoshinobu KASAOKA, Yoshihiko IKEGAMI and Tsuguru USUI Department of Urology, Hiroshima University School of Medicine, 1-2-3, Kasumi, Minami-ku, Hiroshima 734-8551 Japan ABSTRACT We report a case of invasive bladder cancer after cyclophosphamide administration for nephrotic syndrome, and briefly discuss the association of bladder cancer and cyclophos phamide. A 6-year-old boy, who was diagnosed as having neph!otic syndrome, was treated with oral administration of prednisolone and cyclophosphamide for 4 years, receiving a total dose of 49.5 g cyclophosphamide. At age 27, a gross hematuria with bloody clots appeared and he presented with postrenal renal failure. He underwent a radical cystourethrectomy and ileal conduit for stage a pT3a pNO MO transitional cell carcinoma of the bladder. He was not given any adjuvant treatments because of his renal insufficiency, and he died from the disease 14 months after rad ical surgery. Key words: Bladder cancer, Cyclophosphamide, Nephrotic syndrome Cyclophosphamide, a cytotoxic alkylating agent, at the Department of N ephrology, Hiroshima is widely used in various malignancies, immune University Hospital on April 25, 1997. An abdomi disorders and organ transplantation1i. Cyclophos nal ultrasound revealed bilateral hydronephrosis phamide is known to cause hemorrhagic cystitis and a large mass on the posterior of the bladder. and, rarely, bladder fibrosis and has also been He was presented to our Department and immedi associated with urothelial malignancies, both ately underwent right percutaneous nephrostomy. -
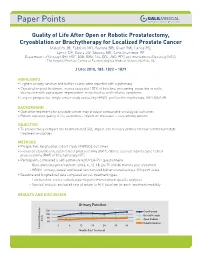
Quality of Life After Open Or Robotic Prostatectomy, Cryoablation Or
Quality of Life After Open or Robotic Prostatectomy, Cryoablation or Brachytherapy for Localized Prostate Cancer Malcolm JB, Fabrizio MD, Barone BB, Given RW, Lance RS, Lynch DF, Davis JW, Shaves ME, Schellhammer PF Departments of Urology (JBM, MDF, BBB, RWG, RSL, DFL, JWD, PFS) and Interventional Radiology (MES), The Virginia Prostate Center at Eastern Virginia Medical School, Norfolk, VA J Urol 2010, 183: 1822 – 1829 HIGHLIGHTS • Highest urinary function and bother scores were reported with cryotherapy • Cryoablation post treatment scores exceeded 100% of baseline, presuming reduction in outlet obstruction with subsequent improvement in obstructive and irritative symptoms • Largest prospective, single center study evaluating HRQOL profiles for cryotherapy, ORP, RAP, BT BACKGROUND • Operative treatments for prostate cancer may produce comparable oncological outcomes • Patient reported quality of life outcomes – important measures – vary among options OBJECTIVE • To prospectively compare the health related QOL impact and recovery profiles for four common prostate treatment modalities METHODS • Prospective, longitudinal cohort study of HRQOL outcomes • Evaluated cryoablation, open radical prostatectomy (ORP), robotic assisted laparoscopic radical prostatectomy (RAP) or brachytherapy (BT) • Participants completed a self-administered UCLA-PCI questionnaire - Questionnaires pre treatment and 3, 6, 12, 18, 24, 30 and 36 months post treatment - HRQOL urinary, sexual and bowel function and bother scored using a 100-point scale • Baseline and -

ARRO Case: HDR Prostate Brachytherapy
ARRO Case: HDR Prostate Brachytherapy Karna Sura, MD (PGY-5) Faculty Advisor: Sirisha Nandalur, MD Department of Radiation Oncology Beaumont Health Case Presentation • 67 year old male presented with an elevated PSA at 3.55 ng/mL • Found to have no evidence of abnormalities on DRE • Underwent prostate biopsy May 22, 2018 Case presentation continued • Discussed various treatment options including: – Active surveillance – Radical prostatectomy – External beam radiation – HDR prostate brachytherapy as a monotherapy – Other options include LDR brachytherapy and SBRT • Patient wanted to proceed with brachytherapy May 22, 2018 Brief History of Prostate Brachytherapy • 1917 – Barringer inserted radium needles transperineally in the prostate • 1952 – Flocks et al. injected radioactive gold solution into prostate cancer • 1972 – Willet Whitmore described an open implant technique using 125I • 1983 – H. Holm described technique of implanting the prostate with radioactive seeds May 22, 2018 Radiobiology behind prostate brachytherapy • Prostate tumors have small fraction of cycling cells and possibly a low α/β ratio • A meta-analysis of 20+ studies has estimated the α/β ratio between 1-4 Gy with a mean of 2.7 Gy • Thus, hypofractionation might be more effective for prostate cancer Patient history • Urologic history – Prior transurethral or open resection of the prostate or other surgery on the urethra – Prior procedure for BPH – Medication for urinary obstructive symptoms – Erectile function • Prior diagnosis of cancer, especially rectal or bladder -

Robotic-Assisted Laparoscopic Radical Prostatectomy After Aborted Retropubic Radical Prostatectomy
J Robotic Surg (2013) 7:301–304 DOI 10.1007/s11701-012-0377-9 CASE REPORT Robotic-assisted laparoscopic radical prostatectomy after aborted retropubic radical prostatectomy Keith J. Kowalczyk • Andy C. Huang • Stephen B. Williams • Hua-yin Yu • Jim C. Hu Received: 11 March 2012 / Accepted: 31 July 2012 / Published online: 19 August 2012 Ó Springer-Verlag London Ltd 2012 Abstract Robotic-assisted laparoscopic prostatectomy of the endopelvic fascia due to poor visualization, a (RALP) has surged in popularity since US Food and Drug prominent pubic tubercle, and a narrow pelvis. The Administration approval in 2000. Advantages include enhanced visualization and precision of the robotic plat- improved visualization and increased instrument dexterity form allowed adequate exposure of the prostate and within the pelvis. Obesity and narrow pelves have been allowed us to proceed with an uncomplicated prostatecto- associated with increased difficulty during open retropubic my, which was not possible to perform easily via an open radical prostatectomy (RRP), but the robotic platform approach. The bladder was densely adherent to the pubis theoretically allows one to perform a radical prostatectomy and the anterior prostatic contour and apex were difficult to despite these challenges. We present an example of a develop due to a dense fibrotic reaction from the previous RALP performed following an aborted RRP. A 49-year-old endopelvic fascia incision. However, we were able to male with intermediate risk prostate cancer and body mass successfully complete RALP with subtle technical modi- index of 38 kg/m2 presented for RALP after RRP was fications. Estimated blood loss was 160 mL and operating aborted by an experienced open surgeon following incision time was 145 min. -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

Princess Margaret Cancer Centre Clinical Practice Guidelines
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GENITOURINARY UROTHELIAL CANCER GU Site Group – Urothelial Cancer Date Guideline Created: March 2012 Author: Dr. Charles Catton 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS 3 5. PATHOLOGY 5 6. MANAGEMENT 6 6.1 PRIMARY PRESENTATION NON-MUSCLE INVASIVE BLADDER DISEASE 6 6.2 RECURRENT PRESENTATION NON-MUSCLE INVASIVE BLADDER DISEASE 6 6.3 MUSCLE INVASIVE BLADDER DISEASE 7 6.4 METASTATIC TCC 10 6.5 MANAGEMENT OF PROGRESSION AFTER INITIAL THERAPY 10 6.6 EXRAVESICAL TCC 11 6.7 ADENOCARCINOMA OF THE BLADDER 12 6.8 ONCOLOGY NURSING PRACTICE 13 7. SUPPORTIVE CARE 13 7.1 PATIENT EDUCATION 13 7.2 PSYCHOSOCIAL CARE 13 7.3 SYMPTOM MANAGEMENT 13 7.4 CLINICAL NUTRITION 14 7.5 PALLIATIVE CARE 14 7.6 OTHER 14 8. FOLLOW-UP CARE 14 9. APPENDIX 1 – PATHOLOGICAL CLASSIFICATION 16 10. APPENDIX 2 – BLADDER CANCER STAGING 19 2 Last Revision Date – March 2012 1. INTRODUCTION Urothelial cancers arise in the urothelium of the renal collecting systems, the ureters, bladder, prostate and urethra. The bladder is the most frequent site of disease accounting in Canada for 5.8% of new cancers and 3.3% of cancer deaths in males, and 2.1% of new cancers and 1.5% of cancer deaths in females (Canadian Cancer Statistics 2008). This difference in incidence is attributed in part to the smoking patterns seen between Canadian men and women. The most common histology is transitional cell carcinoma (TCC). An important feature of transitional cell malignancy is the propensity to behave as a field defect with multifocal disease in primary and recurrent presentations.