Bellevue Hospital Center
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

New York Society for Gastrointestinal Endoscopy the Spring Course
New York Society for Gastrointestinal Endoscopy The Spring Course: Best of DDW 2021 Saturday, June 5, 2021 8:00 am – 3:15 pm Virtual Event The Spring Course: Best of DDW 2021 is jointly provided by the Albert Einstein College of Medicine – Montefiore Medical Center and the New York Society for Gastrointestinal Endoscopy Page 1 of 10 Course Description The Spring Course is devoted to a review of the most compelling topics discussed during Digestive Disease Week® 2021. Faculty will present critically important information on new drugs, the etiology and pathophysiology of disease states, the epidemiology of diseases, the medical, surgical and endoscopic treatment of disease, and the social impact of disease states pertaining to gastroenterology, endoscopy, and liver disease. The program includes a video forum of new endoscopic techniques as well as a summary of the major topics presented at the most important academic forum in gastroenterology, making for an invaluable educational experience for those who were unable to attend Digestive Disease Week® and an excellent summary review for all others. Learning Objectives • Discuss the spectrum of gastrointestinal diseases such as motility disorders and colorectal cancer and outline the enhancement and effectiveness of related treatment options such as the use of artificial intelligence in the detection and resection of polyps during colonoscopy • Evaluate advances in the methods of assessing disease status in patients with inflammatory bowel disease and discuss the application of these techniques -

NURSING HOME SHARPS COLLECTION SITES in NEW YORK STATE (Revised on March 15, 2016 )
NURSING HOME SHARPS COLLECTION SITES in NEW YORK STATE (Revised on March 15, 2016 ) County Nursing Home Address Phone # Hours of Operation Location of Drop‐off 780 Albany Shaker Rd., Thursdays Albany County Nursing Home 518-869-2231 Receiving Department Albany Albany, 12111 8 AM- Noon 180 Washington Ave. Ext., Daughters Of Sarah Nursing Center 518-456-7831 8 AM-4 PM Reception desk in lobby Albany Albany, 12203 Reception Main Campus - 40 Autumn Drive, Sharps received in an Eddy Village Green at Beverwyck 518-482-8774 8 AM-8 PM Slingerlands, 12159 appropriate sealed puncture Albany proof container Guilderland Center Rehabilitation 428 Route 146, Guilderland, 518-861-5141 10 AM-1 PM Lobby Albany and Extended Care Facility 12085 Our Lady Of Hope Residence-little 1 Jeanne Jugan Lane, Wednesday 518-785-4551 Lobby Albany Sisters Of The Poor Latham, 12110 9-11AM 2 Mercycare Lane, Monday thru Friday Main Lobby at Reception Our Lady Of Mercy Life Center 518-464-8100 Albany Guilderland, 12084 9:00AM -3:00PM Desk 27 Hackett Blvd., Monday-Friday St Margarets Center 518-591-3300 Reception Desk Albany Albany, 12208 8:00 AM-4 PM St Peter's Nursing and Rehabilitation 301 Hackett Blvd., Monday-Friday 518-525-7600 Reception Desk Albany Center Albany, 12208 10:00 AM-3 PM Teresian House Nursing Home Co 200 Washington Ave Ext., Front Entrance, Infrom 518-456-2000 8 AM-3 PM Albany Inc Albany 12203 Switchboard Operator Monday-Friday 140 West Main St., Cuba Memorial Hospital Inc Snf 585-968-2000 8 AM-4 PM Hospital Lobby Cuba 14727 Allegany Highland Park Rehabilitation -
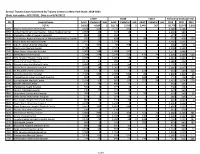
Annual Trauma Cases Submitted by Trauma Centers in New York State
Annual Trauma Cases Submitted by Trauma Centers in New York State: 2018-2021 (Date last update: 8/17/2021, Data as of 8/3/2021) Y2019 Y2020 Y2021 TOTALS by Discharge Year PFI Hospital Name Adult Pediatric Unk Adult Pediatric Unk Adult Pediatric Unk 2019 2020 2021 TOTAL 54,562 4,209 1 50,176 3,793 3 5,443 367 - 58,772 53,972 5,810 0001 Albany Medical Center Hospital 3,168 320 . 3,772 392 . 3,488 4,164 - 0058 United Health Services Hospital - Wilson Medical Center 1,067 23 . 934 13 . 1,090 947 - 0135 Champlain Valley Physicians Hospital 465 12 . 314 2 . 477 316 - 0180 Mid Hudson Regional Hospital of Westchester Medical Center 745 22 . 428 . 98 2 767 428 100 0181 Vassar Brothers Medical Center 1,141 15 . 1,029 2 . 1,156 1,031 - 0208 John R. Oishei Children's Hospital 64 335 . 68 258 2 4 399 326 6 0210 Erie County Medical Center 2,598 1 . 2,525 . 2,599 2,525 - 0245 Stony Brook University Hospital 2,003 168 . 1,686 162 . 2,171 1,848 - 0413 Strong Memorial Hospital 2,244 254 . 2,246 223 470 74 2,498 2,469 544 0511 NYU Langone Hospital-Long Island 1,288 77 . 1,305 56 26 8 1,365 1,361 34 0527 Mount Sinai South Nassau 1,171 17 . 989 4 . 1,188 993 - 0528 Nassau University Medical Center 1,384 34 . 1,187 25 . 1,418 1,212 - 0541 North Shore University Hospital 2,150 16 . 1,907 10 . -
Division of Community and Population Health Report
Division of Community and Population Health Report Table of Contents Expanding Our Reach to Help More Neighbors 1 Community and Population Health Leadership 2 About NewYork-Presbyterian 3 Division of Community and Population Health: Our Mission 4 Clinical Services: Ambulatory Care Network 6 Ambulatory Care Network Nursing 11 Telehealth 13 Community Health Programs 14 ANCHOR (Addressing the Needs of the Community Through Holistic, Organizational Relationships) 15 Behavioral Health Clinical Services (Outpatient) 16 Building Bridges, Knowledge and Health Coalition 18 Center for Community Health and Education 19 CCHE: Family Planning Program and Young Men’s Clinic 20 CCHE: School-Based Health Center Program 21 CCHE: Uptown Hub 22 Center for Community Health Navigation 24 Centering Pregnancy Program and The Carnegie Hall Lullaby Project 26 Collaborator Network Workforce Development and Training 27 Choosing Healthy & Active Lifestyles for Kids™ (CHALK) 28 Compass 30 Community-Based Sexual Health 31 Cultural Competency and Health Literacy Workgroup 35 Health & Housing 36 Health for Life 37 Health Home 38 Healthy City Kids 39 Lang Youth Medical Program 40 Manhattan Cancer Services Program 41 NewYork-Presbyterian Performing Provider System Impact Grants 42 Outreach Program 43 Reach Out and Read Program 44 The Family PEACE (Preventing Early Adverse Childhood Experiences) Trauma Treatment Center 45 Turn 2 Us (T2U) 46 Waiting Room As a Literacy & Learning Environment (WALLE) 47 Women, Infants, and Children Program (WIC) 48 Workforce Development and -

A Guide to Innovative, Quality Long Term Care Options in New York
A Guide to Innovative, Quality e Long Term Care c Options in New York r u o S e r 555 WEST 57TH STREET a NEW YORK, NY 10019 212.258.5330 P 212.258.5331 F WWW.CCLC.ORG C CareSource A Guide to Innovative, Quality Long Term Care Options in New York CCLC Staff Contacts: About CCLC The Continuing Care Leadership Coalition (CCLC) is a membership Scott C. Amrhein 212.506.5409 and advocacy organization representing more than 100 of the President nation’s most innovative and comprehensive not-for-profit and public long term care organizations in the New York metropolitan Roxanne G.Tena-Nelson 212.506.5412 area and beyond. CCLC’s establishment in 2003 as an affiliate of the Vice President Greater New York Hospital Association (GNYHA) highlights the growing importance of continuing care services in today’s health Desmond D’Sa 212.506.5458 care marketplace. Associate Vice President of Finance and Reimbursement CCLC’s purpose is to shape, through advocacy, research, and education, Kelly L. Donohue an environment that supports the delivery of, and access to, contin- Director of Communications 212.506.5424 uing care services of the highest quality and to provide State and national leadership in advancing effective continuing care policies Jenifer H. Fergusson and practices through the collective experience, vision, and effort Events Planner 212.506.5426 of our members. LaSheandra Hunter 212.506.5429 The members of CCLC provide mission-driven services across the Operations Assistant continuum of care to people of all ages throughout the New York metropolitan area and beyond. -

Health Systems and Hospitals
FS000006046 121st Street Family Health Center CS000434510 121st. Street Hc CS000434511 35th Street Hc FS000001385 35th Street Health Center CS000000267 3rd Avenue Pediatrics CS000000284 43rd Street Family Practice CS000434512 53rd Street Hc CS000140193 54 Main Street Medical Practice Pc RX000020261 58th Street Pharmacy, Inc., Town Drug And Surgical CS000000410 609 Fulton Pediatrics Pc CS000000405 61st St Family Health Center CS000436719 786 Medical Pc FS000010161 850 Grand St Campus High School CS000000425 8th Avenue Medical Office CS000000498 93 17 Medical Office Pc CS000187023 @phillips Ambulatory Care Center CS000430681 A & E Ob Gyn Pc FS000000534 A Holly Patterson Extended Care Facility FS000006802 A Merryland Health Center CS000437620 A Plus Medical Care CS000438635 A To Z Pediatrics, Pc CS000438636 A&d; Medical, Pc CS000000633 Aaron B Grotas Md CS000000634 Aaron Daluiski Md CS000000995 Aaron David Ob/gyn CS000000658 Aaron E Walfish Md CS000000665 Aaron N Manson Md CS000434513 Aaron Woodall, Md CB000000002 Abbott House As of: September 7, 2021 Page 1 MH000018730 Abbott House, Inc. CS000000788 Abbydek CS000000795 Abbydek Family Medical Practice CS000434158 Abbydek Family Medical Practice CS000000800 Abbydek Family Medical Practice CS000000867 Abdul A Khuwaja Md CS000436229 Abdul-haki Issah, Md, Pc CS000000986 Abk Neurological Associates FS000004471 Able Health Care Service Inc CS000001174 Abu M Haque M.d CS000438945 Academic Health Care Center FS000000941 Acadia Center For Nursing And Rehabilitation CS000001348 Access Community Health -

1 a Letter from Hospital Providers
A Letter from Hospital Providers Regarding COVID-19 and Homelessness in New York City April 15, 2020 Dear Mayor Bill de Blasio, Governor Andrew Cuomo, NYC Department of Social Services Commissioner Steven Banks, New York City Emergency Management Commissioner Deanne Criswell, City Council Speaker Corey Johnson, and City Council Member Stephen Levin: We are frontline workers—physicians, nurses, social workers, and others—from hospitals across New York City writing to express our concerns and recommendations specific to the thousands of New Yorkers who are homeless during the COVID-19 pandemic. These individuals cannot stay home, because they have no home. They are at high risk for contracting and dying from COVID-19. Homeless New Yorkers are our patients and our neighbors. We commend you for steps you have taken to protect them and to preserve the capacity of our hospitals, such as creating isolation sites for people experiencing homelessness who have symptoms of COVID-19 and developing protocols to keep people with only mild symptoms out of emergency departments. Many of us have expressed our concerns publicly and privately, and are appreciative that several of these concerns have been addressed. We remain troubled, however, at the slow and still inadequate response to protect homeless New Yorkers. As of April 12, there were already 421 homeless New Yorkers known to be infected with COVID-19 and 23 had died from the disease. Black and Latinx New Yorkers are disproportionately affected by homelessness and incarceration (itself associated with both homelessness and risk of exposure to coronavirus), layering health inequity upon health inequity. -

A New Look at Our History: Part I
1 1 MOUNT SINAI QUEENS 0 2 r e b m e v o inside N A New Look at Our History: Part I In this issue of Inside Queens, we tell the story of our Hospital’s very beginnings up through the 1930s. We will continue the story from the postwar years to the present in the December issue. Up until 2010, the accepted thinking was that our history dated to 1910. Based on that date, we thought we reached our centennial as a hospital. In fact, research shows that Mount Sinai Queens can trace its history back almost 120 years to 1892, when Astoria was hailed as “one of New York’s fairest suburbs,” a magnet for the wealthy and successful. It was nearly 20 years earlier than we first thought, in 1892, that the Hospital was founded by a group of Astoria philanthropists, led by Mrs. Frank E. Hagemeyer and included Mrs. Blackwell, Riker and Rapelye—a who’s who of the elite in northwestern Queens. The original Astoria Hospital opened in a former private residence leased by William Steinway of the Steinway piano family, and was CONTINUED ON PAGE 2 The original hospital, today’s Annex Look Focus On: Emergency Department inside Whether patients walk in or arrive by ambulance, the Emergency Department (ED) sees a wide range Joining the Medical Staff: of emergency cases—stroke, cardiac, broken bones, Melissa S. Lee, MD infections, asthma and those needing stitches, the Take a Bow list is long. “What we do hasn’t changed over the years,” says Deborah Dean, MD, Acting Interim Great American Smokeout Director, shown here to the right, second from the September Employee of right. -

Dental Clinics in NYS That Accept Medicaid
Dental Clinics in NYS that accept Medicaid LONG ISLAND, NY Family Health Centers Long Island FQHC 1600 Steward Avenue Westbury NY 11590 Suite 300 516-296-3742 Dental Center Locations: Elmont, Freeport, Roosevelt. Damian Family Health-Long Island City Family Health Center 34-11 Vernon Blvd. Long Island City, NY 11106 347-630-8401 New Life Community Health Center free or charitable clinic (NAFC) 82-10 Queens Blvd Elmhurst, NY 11373 718-565-9844 Charles Evans Center 857 South Oyster Bay Road Bethpage NY 11714 516-622-8888 Charles Evans Center 305 Oser Ave, Hauppauge NY 11788 631-524-5290 Maxine S. Postal Tri-Community Health Center Dental HRH Care Community Health 1080 Sunrise Highway Amityville, NY 11701 631-716-9026 Elsie Owens Health Center Dental at Coram HRHCare Community Health 82 Middle Country road Coram, NY11727 631-320-2220 Health Center at Riverhead HRHCare Community Health 300 Center Drive South, Riverhead, NY 11901 631-574-2580 HRHCare Kraus Family Health Center at Southampton 330 Meeting House Lane Southampton, NY 11968 631-268-1008 Center at Beacon Dental HRH Care Community Health 6 Henry Street Beacon, NY 12508 845-831-0400 Health Center at Brentwood Dental HRH Community Health 1869 Brentwood Road Brentwood NY 11717 631-994-2900 The Floating Hospital: Queensbridge Health Center 10-29 41st Avenue Long Island City, NY 11101 718-361-6266 The Floating Hospital: Astoria Health Center 8-13 Astoria Blvd, Astoria, NY 11102 718-545-0934 Advantage Care Dental Brookville Location 189 Wheatley Road Brookville, NY 11545 516-686-4400 Advantage -

Prep-AP Providers
PrEP-AP Providers County Provider & Address Phone ALBANY Albany Medical Center Hospital 1 Clara Barton Drive 518-262-4439 Albany, NY 12208 Albany Medical Center Hospital 22 New Scotland Ave 518-262-4439 Albany, NY 12208 Byrd E. Cleveland, MD Albany Medical College 518-262-4439 1 Clara Barton Drive Albany, NY 12208 Cynthia H. Miller, MD Albany Medical College 518-262-4043 1 Clara Barton Drive Albany, NY 12208 Cynthia H. Miller, MD Albany Medical College 518-262-9600 47 New Scotland Avenue Albany, NY 12208 David A. Ray, MD AMC HIV Clinic 518-262-4439 1 Clara Barton Drive Albany, NY 12208 Debra Tristram, MD AMC Pediatric Infectious Diseases 518-262-6888 47 New Scotland Avenue Albany, NY 12208 Heidi L. Finkle, NP Albany Medical College - - 22 New Scotland Avenue, 3rd Floor Albany, NY 12208 John A Bellizzi, MD Albany Medical College 518-262-4043 1 Clara Barton Drive Albany, NY 12208 Marcus E. Friedrich, MD Albany Medical College 518-262-4043 1 Clara Barton Drive Albany, NY 12208 Shelley A. Gilroy, MD Albany Medical College 518-264-4439 1 Clara Barton Drive Albany, NY 12208 8/5/2021 9:45:15 AM ALBANY Whitney M Young Health Center 10 Dewitt Street 518-463-3882 FL 1 Albany, NY 12207 Whitney M Young Health Center 1804 Second Avenue 518-833-6900 Suite B Watervliet, NY 12189 Whitney M. Young Health Center 920 Lark Drive 518-463-6824 Albany, NY 12207 BRONX BronxCare Dr MLK JR Health Center 1265 Franklin Avenue 718-901-8988 Bronx, NY 10456 BronxCare Hospital Center Bronxcare Health System 718-992-7669 1650 Grand Concourse Bronx, NY 10457 BronxCare Hospital Center Controller's Office 718-992-7669 1276 Fulton Avenue Bronx, NY 10456 Community Health Project Inc. -

Name Graduation Year Current Status/Employment Lindsey Reese, MD
Name Graduation Year Current Status/Employment Lindsey Reese, MD 2011 Associate Vice Chair of Clinical Affairs, Assistant Professor, Indiana University School of Medicine, Indiana, IN Keith Sigel, MD 2011 Associate Professor, Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, NY Meenakshi Rana, MD 2011 Assistant Professor, Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, NY Nicole Bouvier, MD 2011 Associate Professor, Department of Medicine, Department of Microbiology, Icahn School of Medicine at Mount Sinai, New York, NY Alison Brodginski, DO 2011 Physician, Infectious Diseases Geisinger, Danville, PA Rupa Patel, MD 2011 Assistant Professor, Department of Medicine, Director, Global Health Scholars in Medicine Program, Washington University, St Louis, MO Luciano Kapelusznik, MD 2011 Infectious Disease Physician, Main Line Health, Bryn Mawr, PA Rachel Chasan, MD 2012 Assistant Professor, Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, NY David Banach, MD/MPH/MS 2012 Assistant Professor, Department of Medicine, Head of Infection Prevention, Hospital, Epidemiologist, University of Connecticut, Farmington, CT Melissa Gitman, MD/MPH 2012 Director, Clinical Microbiology Icahn School of Medicine at Mount Sinai, New York, NY Talia Swartz, MD/PhD 2013 Assistant Professor, Department of Medicine, Associate Director of the MD PhD Program, Icahn School of Medicine at Mount Sinai, New York, NY Catherine Smith, MD 2013 Physician, Infectious Diseases St. Vincent’s Healthcare, -

Affordable Health Care Options Community Health Centers
Affordable Health Care Options Community Health Centers Bronx Access Community Health Center Bronx Community Health Network, Family Care for the Homeless, Living Room Medical 1420 Ferris Place Health Center (FHC) Clinic Bronx, NY 10461 1 Fordham Plaza, 5th Floor 800 Barretto Street 718-730-1004 Bronx, NY 10458 Bronx, NY 10474 718-933-2400 347-269-4572 Betances Health Center 280 Henry Street Bronx Community Health Network, Marble Hill Care for the Homeless, Nelson Medical Clinic New York, NY 10002 Family Practice (MHFP) 1605-11 Nelson Avenue 212-227-8401 5525 Broadway Bronx, NY 10453 Bronx, New York 10463 347-269-4625 Brightpoint Health BOOM! Health 718-884-0279 226 East 144th Street Care for the Homeless, Part of the Solution Bronx, NY 10451 Bronx Community Health Network, Park Ave (P.O.T.S.) 855-681-8700 Health Center 2759 Webster Avenue 4196 Park Avenue Bronx, NY 10458 Brightpoint Health HUB Health Center Bronx, NY 10457-6009 347-269-4706 459 East 149th Street 718-466-1573 Bronx, NY 10455 Care for the Homeless, Susan's Place Medical 855-681-8700 Bronx Community Health Network, University Clinic Avenue Family Practice 1911-21 Jerome Avenue Brightpoint Health Westchester Sq Health 105 West 188th Street Bronx, NY 10453 Center Bronx, NY 10468 718-943-1341 2510 Westchester Avenue, Suite 202 718-563-0757 Bronx, NY 10461 Care for the Homeless, Willow Medical Clinic 855-681-8700 Bronx Community Health Network, Via Verde 190 Willow Ave Family Practice Bronx, NY 10454 Bronx Community Health Network, Castle Hill 730 Brook Avenue, Ground Floor