PDF Hosted at the Radboud Repository of the Radboud University Nijmegen
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Histidinol Dehydrogenase from Neurospora Crassa
Fungal Genetics Reports Volume 3 Article 1 Histidinol dehydrogenase from Neurospora crassa E. H. Creaser R. B. Drysdale Follow this and additional works at: https://newprairiepress.org/fgr This work is licensed under a Creative Commons Attribution-Share Alike 4.0 License. Recommended Citation Creaser, E. H., and R.B. Drysdale (1963) "Histidinol dehydrogenase from Neurospora crassa," Fungal Genetics Reports: Vol. 3, Article 1. https://doi.org/10.4148/1941-4765.2139 This Research Note is brought to you for free and open access by New Prairie Press. It has been accepted for inclusion in Fungal Genetics Reports by an authorized administrator of New Prairie Press. For more information, please contact [email protected]. Histidinol dehydrogenase from Neurospora crassa Abstract Histidinol dehydrogenase from Neurospora crassa This research note is available in Fungal Genetics Reports: https://newprairiepress.org/fgr/vol3/iss1/1 RESEARCH NOTES Creaser, E.H. and R. B. Drysdale. Histidinol It is thought that the locus histidine-3 controls hvo --__ dehydrogenase from Neurosooro w. functions in Neurospora, the first of these being in the early stages ot histidine biosynthesis and largely unknown at present. The second function is to direct the formation of the terminal enzyme in the sequence- histidinol dehydrogenase. We have studied the purification and some properties of this enzyme. The enzyme con be extracted from wet mycelium by grinding with gloss powder or from dried mycelium by extraction with pH 9. I Tris buffer. The extract is treated with 0.05M MnC12 to prec:pitate nucleic acids and unwonted proteins. Ammonium sulphate is added to 50% saturation and the precipitate discorded. -

And TROTTER 1967) in a Position Comparable to That of the Histidine Operon in S
HISTIDINE-REQUIRING MUTANTS OF ESCHERZCHZA COLZ K12 LINDA GARRICK-SILVERSMITH1 AND PHILIP E. HARTMAN Department of Biology, The Johns Hopkins University, Baltimore, Maryland 21218 Received April 30, 1970 INSalmonella typhimurium a cluster of nine genes controlling histidine bio- synthesis has been mapped in detail and correlated with enzymes in the biochemical pathway. Numerous observations are in accord with the concept of a unified control-or operon system-for the histidine genes in Salmonella (LOPERet al. 1964; AMESet al. 1967). Mutations leading to a requirement for histidine are known in Escherchia coli and have been located on the E. coli K12 genetic map (TAYLORand TROTTER 1967) in a position comparable to that of the histidine operon in S. typhimurium (SANDERSON1967). Data presented here indicate that the his genes in E. coli are clustered and may constitute an operon very similar to that of Salmonella. The relative positions of two nearby genes in E. coli also are the same as in Salmonella. However, heterogeneity must be present between the two species, for E. coli F’ his recombines readily within E. coli but fails to recombine, or recombines only very rarely, with the chromosome when present in Salmonella. For reasons which are not understood, among E. coli histidine mutations (in comparison with pre- vious studies in Salmonella) extended deletions are unusually common while point mutations, particularly in certain genes, are rare. The independent studies reported in the accompanying paper by GOLDSCHMIDTet al. (1970) extend these observations. MATERIALS AND METHODS Bacteria2 strains: Histidine-requiring mutants were obtained in several E. coli K12 sublines after screening through penicillin (Table 1). -

Diphosphate (Ppgpp): Positive Effector for Histidine Operon
Proc. Nat. Aced. Sci. USA Vol. 72, No. 11, pp. 4389-4393, November 1975 Biochemistry Guanosine 5'-diphosphate 3'-diphosphate (ppGpp): Positive effector for histidine operon transcription andgeneral signal for amino-acid deficiency (relaxed-stringent control/alarmones/Salmonella typhimurium/super-control/coupled in vitro protein synthesis) JOHN C. STEPHENS, STANLEY W. ARTZ, AND BRUCE N. AMES Department of Biochemistry, University of California, Berkeley, Calif. 94720 Contributed by Bruce N. Ames, September 5, 1975 ABSTRACT Maximal expression of the histidine operon pression experiments; and TA1995 (dhuAl) and TA1996 of Salmonella typhimurium in a coupled in vitro transcrip- (dhuAl relAl)-amino-acid analog studies. The rel-1 muta- tion-translation system is strongly dependent upon addition tion (8) has been designated a relA mutation (9) on the basis of guanosine 5'-diphosphate 3'-diphosphate (ppGpp). This re- quirement for ppGpp is exerted at the level of transcription of genetic mapping, phenotype, and biochemical character- through a mechanism distinct from the his-operon-specific ization (unpublished experiments). The dhuAl mutation regulatory mechanism. In vivo derepression of the his oper- (10) was used to facilitate strain construction and is not per- on is markedly defective when histidine starvation is im- tinent to these studies. The following Escherichia coli lyso- posed on a relA mutant-unable to rapidly increase synthesis gens (11) were used as source of template DNA: TA1933 of ppGpp-growing in amino-acid-rich medium. Increased [his-6607 StrR h immX cI857 susS7, (80 h dhisO+ sensitivity of relA mutants to growth inhibition by a number (080 of amino-acid analogs suggests that pp-pp is generally im- immA cI857 susS7)]; and TA1940 [his-6607 StrR ()80 h portant in adjusting expression of amino-acid-producing sys- immX cI857 susS7, 4i80 h dhisO1242 immx cI857 susS7)]. -

L -Histidinol Dihydrochloride
L-Histidinol dihydrochloride Product Number H 6647 Store at Room Temperature Product Description Preparation Instructions Molecular Formula: C6H11N3O • 2HCl Histidinol is soluble in water (50 mg/ml), yielding a Molecular Weight: 214.1 clear, colorless solution. CAS Number: 1596-64-1 Melting point: 193-195 °C1 Storage/Stability A 5% aqueous solution of histidinol is stable at room L-Histidinol is a potent and reversible inhibitor of temperature for a minimum of 24 hours. Frozen stock protein synthesis in cultured human cells2 and is a solutions of histidinol are not recommended for use precursor of histidine in procaryotes and some after one month. eukaryotes. Histidinol does not significantly affect histidine transport into cells, but most likely inhibits References protein synthesis by decreasing the activation of 1. Dictionary of Organic Compounds, 5th ed., histidine. Histidinol competitively inhibits the Chapman and Hall (New York, NY: 1982), pyrophosphate-ATP exchange reaction that is Entry# A-01868. promoted by histidyl-tRNA synthetase in the presence 2. Hansen, B. S., et al., Reversible Inhibition by of histidine. When culture media contains 5 µM Histidinol of Protein Synthesis in Human Cells at histidine, protein synthesis is inhibited 50% in the the Activation of Histidine. J. Biol. Chem., 247(12), presence of 0.1 mM histidinol.2 3854-3857 (1972). 3. Thompson, L. H., Mutant Isolation. Meth. A procedure has been published for the use of Enzymol., 58, 308-322 (1979). histidinol in cell culture mutant selection.3 Histidinol 4. Grubmeyer, C. T., and Gray, W. R., A Cysteine has been used as a substrate for histidinol Residue (Cysteine-116) in the Histidinol Binding dehydrogenase from Salmonella typhimurium at Site of Histidinol Dehydrogenase. -

Transcriptional Regulation Mechanisms Involved in Azole Resistance in Candida Species: Focusing on the Transcription Factors Rpn4 and Mrr1
Transcriptional regulation mechanisms involved in azole resistance in Candida species: focusing on the transcription factors Rpn4 and Mrr1 Raquel da Silva Califórnia Thesis to obtain the Master of Science Degree in Biotechnology Supervisor: Prof. Dr. Miguel Nobre Parreira Cacho Teixeira Examination Committee Chairperson: Prof. Dr. Ana Cristina Anjinho Madeira Viegas Supervisor: Prof. Dr. Miguel Nobre Parreira Cacho Teixeira Member of the Committee: Dr. Catarina Isabel Ribeiro Pimentel October 2018 ii Acknowledgements For me the development of this thesis was very challenging and involved a very extensive work, whose purpose would not have been reached without the help of some people I will mention below. First of all, I would like to thank my supervisor Professor Miguel Teixeira for the opportunity given by accepting me in his team and in this project. His tremendous support, guidance and motivation, always available to help, were crucial for the success of this work. I would like to thank Professor Isabel Sá-Correia for giving me the chance to join the Biological Sciences Research Group to develop my master thesis work. The achievement of this thesis required an indispensable help from several parts, which deserve my recognition. For the collaboration in the transcriptomic analysis herein accomplished, I thank Professor Geraldine Butler and her team, from University College of Dublin. For the supply of Candida glabrata mutants used in this work, I have to thank Professor Hiroji Chibana, from University of Chiba, Japan. For the study developed in HPLC analysis of ergosterol levels, I thank also Professor Nuno Mira for his availability and assistance. My gratitude should also be expressed towards my colleague, Pedro Pais, for the great help he has given me throughout this period, always available to help and explain anything. -
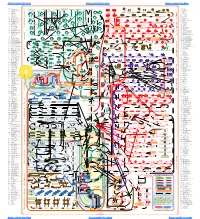
O O2 Enzymes Available from Sigma Enzymes Available from Sigma
COO 2.7.1.15 Ribokinase OXIDOREDUCTASES CONH2 COO 2.7.1.16 Ribulokinase 1.1.1.1 Alcohol dehydrogenase BLOOD GROUP + O O + O O 1.1.1.3 Homoserine dehydrogenase HYALURONIC ACID DERMATAN ALGINATES O-ANTIGENS STARCH GLYCOGEN CH COO N COO 2.7.1.17 Xylulokinase P GLYCOPROTEINS SUBSTANCES 2 OH N + COO 1.1.1.8 Glycerol-3-phosphate dehydrogenase Ribose -O - P - O - P - O- Adenosine(P) Ribose - O - P - O - P - O -Adenosine NICOTINATE 2.7.1.19 Phosphoribulokinase GANGLIOSIDES PEPTIDO- CH OH CH OH N 1 + COO 1.1.1.9 D-Xylulose reductase 2 2 NH .2.1 2.7.1.24 Dephospho-CoA kinase O CHITIN CHONDROITIN PECTIN INULIN CELLULOSE O O NH O O O O Ribose- P 2.4 N N RP 1.1.1.10 l-Xylulose reductase MUCINS GLYCAN 6.3.5.1 2.7.7.18 2.7.1.25 Adenylylsulfate kinase CH2OH HO Indoleacetate Indoxyl + 1.1.1.14 l-Iditol dehydrogenase L O O O Desamino-NAD Nicotinate- Quinolinate- A 2.7.1.28 Triokinase O O 1.1.1.132 HO (Auxin) NAD(P) 6.3.1.5 2.4.2.19 1.1.1.19 Glucuronate reductase CHOH - 2.4.1.68 CH3 OH OH OH nucleotide 2.7.1.30 Glycerol kinase Y - COO nucleotide 2.7.1.31 Glycerate kinase 1.1.1.21 Aldehyde reductase AcNH CHOH COO 6.3.2.7-10 2.4.1.69 O 1.2.3.7 2.4.2.19 R OPPT OH OH + 1.1.1.22 UDPglucose dehydrogenase 2.4.99.7 HO O OPPU HO 2.7.1.32 Choline kinase S CH2OH 6.3.2.13 OH OPPU CH HO CH2CH(NH3)COO HO CH CH NH HO CH2CH2NHCOCH3 CH O CH CH NHCOCH COO 1.1.1.23 Histidinol dehydrogenase OPC 2.4.1.17 3 2.4.1.29 CH CHO 2 2 2 3 2 2 3 O 2.7.1.33 Pantothenate kinase CH3CH NHAC OH OH OH LACTOSE 2 COO 1.1.1.25 Shikimate dehydrogenase A HO HO OPPG CH OH 2.7.1.34 Pantetheine kinase UDP- TDP-Rhamnose 2 NH NH NH NH N M 2.7.1.36 Mevalonate kinase 1.1.1.27 Lactate dehydrogenase HO COO- GDP- 2.4.1.21 O NH NH 4.1.1.28 2.3.1.5 2.1.1.4 1.1.1.29 Glycerate dehydrogenase C UDP-N-Ac-Muramate Iduronate OH 2.4.1.1 2.4.1.11 HO 5-Hydroxy- 5-Hydroxytryptamine N-Acetyl-serotonin N-Acetyl-5-O-methyl-serotonin Quinolinate 2.7.1.39 Homoserine kinase Mannuronate CH3 etc. -

Coordinate Repression of the Synthesis of Four Histidine Biosynthetic Enzymes by Histidine by Bruce N
Proceedings of the NATIONAL ACADEMY OF SCIENCES Volume 45 - Number 10 - October 15, 1959 COORDINATE REPRESSION OF THE SYNTHESIS OF FOUR HISTIDINE BIOSYNTHETIC ENZYMES BY HISTIDINE BY BRUCE N. AMES AND BARBARA GARRY NATIONAL INSTITUTE OF ARTHRITIS AND METABOLIC DISEASES, BETHESDA, MARYLAND Communicated by Herman AM. Kalekar, August 20, 1959 Introduction.-In several instances, the rate of synthesis of the enzymes of a bio- synthetic pathway appears to be regulated by the size of the pool of the end product of that pathway.1-4 This phenomenon has been called enzyme repression.2 We have observed repression by histidine during the investigation of the histidine biosynthetic enzymes in histidine-requiring mutants of Salmonella typhimurium.6 The cellular concentration of the four histidine biosynthetic enzymes which were examined were increased about 15-fold by limiting the amount of histidine available to a mutant during growth. A simple method for limiting the availability of histidine in the cell during the entire growth period, and thus increasing the enzyme concentrations, was realized by growing histidine-requiring mutants on a derivative of histidine, formylhistidine, as a source of this amino acid. It appeared, therefore, that the normal low level of the biosynthetic enzymes in wild-type cells grown on minimal medium was probably due to the repression by the normal pool of histidine. of most of the cellular capacity for synthesizing these proteins. This investigation is concerned with utilizing the histidine biosynthetic system from -

Oxidized Phospholipids Regulate Amino Acid Metabolism Through MTHFD2 to Facilitate Nucleotide Release in Endothelial Cells
ARTICLE DOI: 10.1038/s41467-018-04602-0 OPEN Oxidized phospholipids regulate amino acid metabolism through MTHFD2 to facilitate nucleotide release in endothelial cells Juliane Hitzel1,2, Eunjee Lee3,4, Yi Zhang 3,5,Sofia Iris Bibli2,6, Xiaogang Li7, Sven Zukunft 2,6, Beatrice Pflüger1,2, Jiong Hu2,6, Christoph Schürmann1,2, Andrea Estefania Vasconez1,2, James A. Oo1,2, Adelheid Kratzer8,9, Sandeep Kumar 10, Flávia Rezende1,2, Ivana Josipovic1,2, Dominique Thomas11, Hector Giral8,9, Yannick Schreiber12, Gerd Geisslinger11,12, Christian Fork1,2, Xia Yang13, Fragiska Sigala14, Casey E. Romanoski15, Jens Kroll7, Hanjoong Jo 10, Ulf Landmesser8,9,16, Aldons J. Lusis17, 1234567890():,; Dmitry Namgaladze18, Ingrid Fleming2,6, Matthias S. Leisegang1,2, Jun Zhu 3,4 & Ralf P. Brandes1,2 Oxidized phospholipids (oxPAPC) induce endothelial dysfunction and atherosclerosis. Here we show that oxPAPC induce a gene network regulating serine-glycine metabolism with the mitochondrial methylenetetrahydrofolate dehydrogenase/cyclohydrolase (MTHFD2) as a cau- sal regulator using integrative network modeling and Bayesian network analysis in human aortic endothelial cells. The cluster is activated in human plaque material and by atherogenic lipo- proteins isolated from plasma of patients with coronary artery disease (CAD). Single nucleotide polymorphisms (SNPs) within the MTHFD2-controlled cluster associate with CAD. The MTHFD2-controlled cluster redirects metabolism to glycine synthesis to replenish purine nucleotides. Since endothelial cells secrete purines in response to oxPAPC, the MTHFD2- controlled response maintains endothelial ATP. Accordingly, MTHFD2-dependent glycine synthesis is a prerequisite for angiogenesis. Thus, we propose that endothelial cells undergo MTHFD2-mediated reprogramming toward serine-glycine and mitochondrial one-carbon metabolism to compensate for the loss of ATP in response to oxPAPC during atherosclerosis. -

Genome-Scale Metabolic Network Analysis and Drug Targeting of Multi-Drug Resistant Pathogen Acinetobacter Baumannii AYE
Electronic Supplementary Material (ESI) for Molecular BioSystems. This journal is © The Royal Society of Chemistry 2017 Electronic Supplementary Information (ESI) for Molecular BioSystems Genome-scale metabolic network analysis and drug targeting of multi-drug resistant pathogen Acinetobacter baumannii AYE Hyun Uk Kim, Tae Yong Kim and Sang Yup Lee* E-mail: [email protected] Supplementary Table 1. Metabolic reactions of AbyMBEL891 with information on their genes and enzymes. Supplementary Table 2. Metabolites participating in reactions of AbyMBEL891. Supplementary Table 3. Biomass composition of Acinetobacter baumannii. Supplementary Table 4. List of 246 essential reactions predicted under minimal medium with succinate as a sole carbon source. Supplementary Table 5. List of 681 reactions considered for comparison of their essentiality in AbyMBEL891 with those from Acinetobacter baylyi ADP1. Supplementary Table 6. List of 162 essential reactions predicted under arbitrary complex medium. Supplementary Table 7. List of 211 essential metabolites predicted under arbitrary complex medium. AbyMBEL891.sbml Genome-scale metabolic model of Acinetobacter baumannii AYE, AbyMBEL891, is available as a separate file in the format of Systems Biology Markup Language (SBML) version 2. Supplementary Table 1. Metabolic reactions of AbyMBEL891 with information on their genes and enzymes. Highlighed (yellow) reactions indicate that they are not assigned with genes. No. Metabolism EC Number ORF Reaction Enzyme R001 Glycolysis/ Gluconeogenesis 5.1.3.3 ABAYE2829 -

Structural and Functional Conservation of Histidinol Dehydrogenase
Proc. Natl. Acad. Sci. USA Vol. 88, pp. 4133-4137, May 1991 Genetics Structural and functional conservation of histidinol dehydrogenase between plants and microbes (amino acid biosynthesis/Brassica oleracea/cDNA cloning/polymerase chain reaction) ATSUKO NAGAI*, ERIC WARDt, JAMES BECKt, SACHIYO TADA*, JUI-YOA CHANG*, ALFRED SCHEIDEGGER*, AND JOHN RYALSt§ *International Research Laboratories, CIBA-GEIGY (Japan) Ltd., P.O. Box 1, Takarazuka, 665 Japan; tAgricultural Biotechnology Research Unit, CIBA-GEIGY Corporation, P.O. Box 12257, Research Triangle Park, NC 27709; tCIBA-GEIGY AG, CH-4002 Basel, Switzerland Communicated by Mary-Dell Chilton, February 13, 1991 (receivedfor review December 6, 1990) ABSTRACT The partial amino acid sequence of histidinol demonstrate function of the plant clone, the cDNA was ex- dehydrogenase (L-histidinol:NAD+ oxidoreductase, EC pressed in an Escherichia coli strain lacking the histidine 1.1.1.23) from cabbage was determined from peptide frag- operon. The cDNA was found to suppress the his deletion when ments of the purified protein. The relative positions of these the bacteria were grown in the presence of histidinol. peptides were deduced by aligning their sequences with the sequence of the HIS4C gene product of Saccharomyces cerevi- siae. cDNA encoding histidinol dehydrogenase was then am- MATERIALS AND METHODS plified from a library using a polymerase chain reaction primed Plant Material and Bacterial Strains. Mature spring cab- with degenerate oligonucleotide pools of known position and bage (Brassica oleracea L. var capitata L.) was purchased orientation. By using this amplified fragment as a probe, an from a local grocer in Japan. Phage vector A ZAP II and E. -

Discovery of High Affinity Receptors for Dityrosine Through Inverse Virtual Screening and Docking and Molecular Dynamics
Article Discovery of High Affinity Receptors for Dityrosine through Inverse Virtual Screening and Docking and Molecular Dynamics Fangfang Wang 1,*,†, Wei Yang 2,3,† and Xiaojun Hu 1,* 1 School of Life Science, Linyi University, Linyi 276000, China; [email protected] 2 Department of Microbiology, Biomedicine Discovery Institute, Monash University, Clayton, VIC 3800, Australia, [email protected] 3 Arieh Warshel Institute of Computational Biology, the Chinese University of Hong Kong, 2001 Longxiang Road, Longgang District, Shenzhen 518000, China * Corresponding author: [email protected] † These authors contributed equally to this work. Received: 09 December 2018; Accepted: 23 December 2018; Published: date Table S1. Docking affinity scores for cis-dityrosine binding to binding proteins. Target name PDB/UniProtKB Type Affinity (kcal/mol) Galectin-1 1A78/P56217 Lectin -6.2±0.0 Annexin III 1AXN/P12429 Calcium/phospholipid Binding Protein -7.5±0.0 Calmodulin 1CTR/P62158 Calcium Binding Protein -5.8±0.0 Seminal Plasma Protein Pdc-109 1H8P/P02784 Phosphorylcholine Binding Protein -6.6±0.0 Annexin V 1HAK/P08758 Calcium/phospholipid Binding -7.4±0.0 Alpha 1 antitrypsin 1HP7/P01009 Protein Binding -7.6±0.0 Histidine-Binding Protein 1HSL/P0AEU0 Binding Protein -6.3±0.0 Intestinal Fatty Acid Binding Protein 1ICN/P02693 Binding Protein(fatty Acid) -9.1±0.0* Migration Inhibitory Factor-Related Protein 14 1IRJ/P06702 Metal Binding Protein -7.0±0.0 Lysine-, Arginine-, Ornithine-Binding Protein 1LST/P02911 Amino Acid Binding Protein -6.5±0.0 -
All Enzymes in BRENDA™ the Comprehensive Enzyme Information System
All enzymes in BRENDA™ The Comprehensive Enzyme Information System http://www.brenda-enzymes.org/index.php4?page=information/all_enzymes.php4 1.1.1.1 alcohol dehydrogenase 1.1.1.B1 D-arabitol-phosphate dehydrogenase 1.1.1.2 alcohol dehydrogenase (NADP+) 1.1.1.B3 (S)-specific secondary alcohol dehydrogenase 1.1.1.3 homoserine dehydrogenase 1.1.1.B4 (R)-specific secondary alcohol dehydrogenase 1.1.1.4 (R,R)-butanediol dehydrogenase 1.1.1.5 acetoin dehydrogenase 1.1.1.B5 NADP-retinol dehydrogenase 1.1.1.6 glycerol dehydrogenase 1.1.1.7 propanediol-phosphate dehydrogenase 1.1.1.8 glycerol-3-phosphate dehydrogenase (NAD+) 1.1.1.9 D-xylulose reductase 1.1.1.10 L-xylulose reductase 1.1.1.11 D-arabinitol 4-dehydrogenase 1.1.1.12 L-arabinitol 4-dehydrogenase 1.1.1.13 L-arabinitol 2-dehydrogenase 1.1.1.14 L-iditol 2-dehydrogenase 1.1.1.15 D-iditol 2-dehydrogenase 1.1.1.16 galactitol 2-dehydrogenase 1.1.1.17 mannitol-1-phosphate 5-dehydrogenase 1.1.1.18 inositol 2-dehydrogenase 1.1.1.19 glucuronate reductase 1.1.1.20 glucuronolactone reductase 1.1.1.21 aldehyde reductase 1.1.1.22 UDP-glucose 6-dehydrogenase 1.1.1.23 histidinol dehydrogenase 1.1.1.24 quinate dehydrogenase 1.1.1.25 shikimate dehydrogenase 1.1.1.26 glyoxylate reductase 1.1.1.27 L-lactate dehydrogenase 1.1.1.28 D-lactate dehydrogenase 1.1.1.29 glycerate dehydrogenase 1.1.1.30 3-hydroxybutyrate dehydrogenase 1.1.1.31 3-hydroxyisobutyrate dehydrogenase 1.1.1.32 mevaldate reductase 1.1.1.33 mevaldate reductase (NADPH) 1.1.1.34 hydroxymethylglutaryl-CoA reductase (NADPH) 1.1.1.35 3-hydroxyacyl-CoA