Distribution of Most-At-Risk Population Groups and Their Perceptions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -

Report and Opinion 2017;9(7) 60
Report and Opinion 2017;9(7) http://www.sciencepub.net/report Community Based Knowledge, Attitude And Practice Of Rabies In Injibara Town And Its Surroundings, Awi Zone, Amhara Regional State, North-Western Ethiopia Yigardush Wassihune1, Melese Yenew1, Ayalew Niguse2 1 College of Veterinary Medicine, Jigjiga University, P.O. Box.1020, Jigjiga, Ethiopia. 2Lecturer at Jigjiga university, College of Veterinary Medicine, Jigjiga University, P.O. Box.1020, Jigjiga, Ethiopia. [email protected] Abstract: Rabies is a viral disease of all warm blooded animals, which causes acute fatal encephalitis, with almost 100% case fatality rate. It is caused by rabies virus (genus Lyssa virus) which is mainly transmitted by rabid animal bites. This disease occurs in more than 150 countries and territories and about 55,000 people die of rabies every year, mostly in developing world despite that it is preventable disease by vaccination. Ethiopia is highly endemic for rabies; yet, a nationwide data on rabies has not been gathered to reveal the actual magnitude of the problem and public awareness levels. With a conviction that a handful of works on public knowledge, attitude and practice (KAP) in rabies be done to plan, execute any control and/or eradication programs, this study was conducted in Injibara town and its surroundings from November, 2015 to April, 2016 to assess the knowledge, attitudes and practices (KAP) on rabies and related factors. The design was: ccommunity-based retrospective, quantitative study design to assess the KAP on rabies and related factors. The entire three kebeles of the town and its surrounding rural kebeles were considered in the study. -

Modeling Malaria Cases Associated with Environmental Risk Factors in Ethiopia Using Geographically Weighted Regression
MODELING MALARIA CASES ASSOCIATED WITH ENVIRONMENTAL RISK FACTORS IN ETHIOPIA USING GEOGRAPHICALLY WEIGHTED REGRESSION Berhanu Berga Dadi i MODELING MALARIA CASES ASSOCIATED WITH ENVIRONMENTAL RISK FACTORS IN ETHIOPIA USING THE GEOGRAPHICALLY WEIGHTED REGRESSION MODEL, 2015-2016 Dissertation supervised by Dr.Jorge Mateu Mahiques,PhD Professor, Department of Mathematics University of Jaume I Castellon, Spain Ana Cristina Costa, PhD Professor, Nova Information Management School University of Nova Lisbon, Portugal Pablo Juan Verdoy, PhD Professor, Department of Mathematics University of Jaume I Castellon, Spain March 2020 ii DECLARATION OF ORIGINALITY I declare that the work described in this document is my own and not from someone else. All the assistance I have received from other people is duly acknowledged, and all the sources (published or not published) referenced. This work has not been previously evaluated or submitted to the University of Jaume I Castellon, Spain, or elsewhere. Castellon, 30th Feburaury 2020 Berhanu Berga Dadi iii Acknowledgments Before and above anything, I want to thank our Lord Jesus Christ, Son of GOD, for his blessing and protection to all of us to live. I want to thank also all consortium of Erasmus Mundus Master's program in Geospatial Technologies for their financial and material support during all period of my study. Grateful acknowledgment expressed to Supervisors: Prof.Dr.Jorge Mateu Mahiques, Universitat Jaume I(UJI), Prof.Dr.Ana Cristina Costa, Universidade NOVA de Lisboa, and Prof.Dr.Pablo Juan Verdoy, Universitat Jaume I(UJI) for their immense support, outstanding guidance, encouragement and helpful comments throughout my thesis work. Finally, but not least, I would like to thank my lovely wife, Workababa Bekele, and beloved daughter Loise Berhanu and son Nethan Berhanu for their patience, inspiration, and understanding during the entire period of my study. -
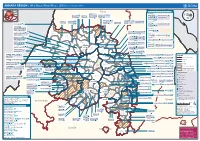
AMHARA REGION : Who Does What Where (3W) (As of 13 February 2013)
AMHARA REGION : Who Does What Where (3W) (as of 13 February 2013) Tigray Tigray Interventions/Projects at Woreda Level Afar Amhara ERCS: Lay Gayint: Beneshangul Gumu / Dire Dawa Plan Int.: Addis Ababa Hareri Save the fk Save the Save the df d/k/ CARE:f k Save the Children:f Gambela Save the Oromia Children: Children:f Children: Somali FHI: Welthungerhilfe: SNNPR j j Children:l lf/k / Oxfam GB:af ACF: ACF: Save the Save the af/k af/k Save the df Save the Save the Tach Gayint: Children:f Children: Children:fj Children:l Children: l FHI:l/k MSF Holand:f/ ! kj CARE: k Save the Children:f ! FHI:lf/k Oxfam GB: a Tselemt Save the Childrenf: j Addi Dessie Zuria: WVE: Arekay dlfk Tsegede ! Beyeda Concern:î l/ Mirab ! Concern:/ Welthungerhilfe:k Save the Children: Armacho f/k Debark Save the Children:fj Kelela: Welthungerhilfe: ! / Tach Abergele CRS: ak Save the Children:fj ! Armacho ! FHI: Save the l/k Save thef Dabat Janamora Legambo: Children:dfkj Children: ! Plan Int.:d/ j WVE: Concern: GOAL: Save the Children: dlfk Sahla k/ a / f ! ! Save the ! Lay Metema North Ziquala Children:fkj Armacho Wegera ACF: Save the Children: Tenta: ! k f Gonder ! Wag WVE: Plan Int.: / Concern: Save the dlfk Himra d k/ a WVE: ! Children: f Sekota GOAL: dlf Save the Children: Concern: Save the / ! Save: f/k Chilga ! a/ j East Children:f West ! Belesa FHI:l Save the Children:/ /k ! Gonder Belesa Dehana ! CRS: Welthungerhilfe:/ Dembia Zuria ! î Save thedf Gaz GOAL: Children: Quara ! / j CARE: WVE: Gibla ! l ! Save the Children: Welthungerhilfe: k d k/ Takusa dlfj k -

The Effects of Lime on Acid Properties of Soil and on Faba Bean Yield in Banja District
American Scientific Research Journal for Engineering, Technology, and Sciences (ASRJETS) ISSN (Print) 2313-4410, ISSN (Online) 2313-4402 © Global Society of Scientific Research and Researchers http://asrjetsjournal.org/ 1. The Effects of Lime on Acid Properties of Soil and on Faba Bean Yield in Banja District. The Case of Sankit Lideta, Awi Zone Amhara Regional State, Ethiopia Ayalew Muluye Melsew* Begimeder College of Teachers Education, Po.Box-20, Debra Tabor, Ethiopia Email : [email protected] Abstracts This study was conducted in the known acid soil area of Ethiopia Awi zone which is found in the Amhara regional state. Five levels of lime introduced (0, 1150kg/ha, 2300kg/ha, 3450kg/ha, 4600kg/ha) on the faba bean productivity in the acidic soils. This experiment was arranged in a factorial experiment using randomized complete block design (RCBD) with three replications and 39 .13kg/ha Urea and100kg/ha TSP had been used as the source of N and P, respectively. Crop data such as plant height, biomass yield and grain yield , 50% flowering ,50% maturity,95% maturity, number of pods/plant ,number of seeds /pod ,number of seeds /plant ,lodging ,stand count at emerge and harvest collected and analyzed using SAS Software version 9. The result of this study indicated that 4600kg/ha, lime brought significantly higher result than the control. As lime level increased from the 0 to 4600kg/ha, grain yield, 50% flowering, biomass yield, number of pods /plant, number of seeds/plant increased. However, as lime level increased the number of seeds/ pod, stand count at emerges, stand count at harvest, 50%maturity, 95%maturity did not bring significant change. -

Chapter 22 Daatsʼíin, a Newly Identified Undocumented Language of Western Ethiopia: a Preliminary Examination Colleen Ahland SIL International
Chapter 22 Daatsʼíin, a newly identified undocumented language of western Ethiopia: A preliminary examination Colleen Ahland SIL International Daatsʼíin is a heretofore unknown language spoken in western Ethiopia near the border with the Republic of Sudan. The Daatsʼíin people live in both Ethiopia and the Republic of Sudan but only those in Ethiopia still speak the Daatsʼíin language. The speakers of Daatsʼíin may number around 1,000 but may be as few as 300-500. This paper provides the first-ever overview of basic aspects of Daatsʼíin phonology, morphology and syntax. The overview documents that Daatsʼíin is structurally similar to the nearby Gumuz languages (of possible Nilo-Saharan affiliation) in many respects, including vocabulary, bound pronominals with a distinct tone for S versus A arguments, and incorporated nouns. However, there are a few differences, mainly in structure and certain tense-aspect categories of the verb word. 1 Introduction Daatsʼíin is the autonym of a people group living in western Ethiopia and the southern part of the Republic of Sudan. The Daats’íin in Sudan have lost their traditional language but those in Ethiopia still speak it. Up until 2013, the language and people group were unknown to researchers and not included in the Ethiopian Census. I traveled to the area in 2014 in order to investigate the language and confirmed that Daatsʼíin (ISO dtn) is distinct from but closely related to Gumuz (ISO guk). I estimate that the Daatsʼíin likely number less than 1000 and that their language may be in danger of dying due to their population size and the heavy influence of Arabic and Amharic in the area. -

Assessing on the Geotechnical Problems Which Causes for the Road Failure from Gilgel Beles to Bahir Dar Road Segment Habtamu Washe Mite 1, Maschal Tilahun Zenebe 2
International Journal of Scientific & Engineering Research Volume 11, Issue 10, October-2020 714 ISSN 2229-5518 Assessing on the Geotechnical Problems Which Causes for the Road Failure from Gilgel Beles to Bahir Dar Road Segment Habtamu Washe Mite 1, Maschal Tilahun Zenebe 2, 1 Department of Civil Engineering, College of Engineering, Assosa University, Assosa, Ethiopia E-Mail – [email protected] 2 Department of Water Resource and Irrigation Engineering, College of Engineering, Assosa University, Assosa, Ethiopia ABSTRACT Geotechnical problems such as problematic soils (expansive soil, organic soil, natural collapsible soils, etc.), problematic rock (shale, weathered limestone), soil slope instability and rock slope instability or rock fall (landslide) which damaged civil engineering structures, such as roads, buildings, dams, railway, and other related structures in Ethiopia. The research was conducted by identifying the geotechnical problems and its effects on road segments in the north west part of Ethiopia, specifically along Gilgel Belles – Bahir Dar road segments. Gilgel Beles – Bahirdar road segment which passes on the hilly and mountainous terrain are characterized by variable topographical, geological, hydrological and land-use condition. The most appendant geotechnical problems that found in the road segments were slope instability, sink holes, road cracks, compressibility of soils. It was identified the causes and effects of the geotechnical problems on the road’s alignment condition. Slope instability(landslide), expansive soil, and drainage problems have been a common problem along the Gilgel Beles – Bahir Dar road, especially during the rainy seasons particularly Chagni -Mandura road section. A detailed slope stability analysis and understanding the causes for independent slope sections was helpful to find a better remedial measure, because different slope sections may have different mode of failure, and may involve different engineering material. -

Ethiopia: Amhara Region Administrative Map (As of 05 Jan 2015)
Ethiopia: Amhara region administrative map (as of 05 Jan 2015) ! ! ! ! ! ! ! ! ! ! Abrha jara ! Tselemt !Adi Arikay Town ! Addi Arekay ! Zarima Town !Kerakr ! ! T!IGRAY Tsegede ! ! Mirab Armacho Beyeda ! Debark ! Debarq Town ! Dil Yibza Town ! ! Weken Town Abergele Tach Armacho ! Sanja Town Mekane Berhan Town ! Dabat DabatTown ! Metema Town ! Janamora ! Masero Denb Town ! Sahla ! Kokit Town Gedebge Town SUDAN ! ! Wegera ! Genda Wuha Town Ziquala ! Amba Giorges Town Tsitsika Town ! ! ! ! Metema Lay ArmachoTikil Dingay Town ! Wag Himra North Gonder ! Sekota Sekota ! Shinfa Tomn Negade Bahr ! ! Gondar Chilga Aukel Ketema ! ! Ayimba Town East Belesa Seraba ! Hamusit ! ! West Belesa ! ! ARIBAYA TOWN Gonder Zuria ! Koladiba Town AMED WERK TOWN ! Dehana ! Dagoma ! Dembia Maksegnit ! Gwehala ! ! Chuahit Town ! ! ! Salya Town Gaz Gibla ! Infranz Gorgora Town ! ! Quara Gelegu Town Takusa Dalga Town ! ! Ebenat Kobo Town Adis Zemen Town Bugna ! ! ! Ambo Meda TownEbinat ! ! Yafiga Town Kobo ! Gidan Libo Kemkem ! Esey Debr Lake Tana Lalibela Town Gomenge ! Lasta ! Muja Town Robit ! ! ! Dengel Ber Gobye Town Shahura ! ! ! Wereta Town Kulmesk Town Alfa ! Amedber Town ! ! KUNIZILA TOWN ! Debre Tabor North Wollo ! Hara Town Fogera Lay Gayint Weldiya ! Farta ! Gasay! Town Meket ! Hamusit Ketrma ! ! Filahit Town Guba Lafto ! AFAR South Gonder Sal!i Town Nefas mewicha Town ! ! Fendiqa Town Zege Town Anibesema Jawi ! ! ! MersaTown Semen Achefer ! Arib Gebeya YISMALA TOWN ! Este Town Arb Gegeya Town Kon Town ! ! ! ! Wegel tena Town Habru ! Fendka Town Dera -

Journal of Critical Reviews SOCIAL CONDITIONS of SHINASHA TRIALS in NORTHWESTERN ETHIOPIA
Journal of Critical Reviews ISSN- 2394-5125 Vol 7, Issue 9, 2020 SOCIAL CONDITIONS OF SHINASHA TRIALS IN NORTHWESTERN ETHIOPIA 1Abebe Ano Alula, 2Arjun Rao Kuthadi (Ph.D.) 1Ph.D. candidate in Department of History, College of Social Sciences and Art Osmania University, Hyderabad, India 2Professor of History ,Supervisor, Department of History, College of Social Sciences and Art Osmania University, Hyderabad, India Received: 24.03.2020 Revised: 14.04.2020 Accepted: 22.05.2020 Abstract This article is primarily concerned to explore the social conditions of the Shinasha community in northwestern Ethiopia. Shinasha is some of the Indigenous groups with Ca. 60,587 population in Ethiopia, Africa continent, who are living Benishangul-Gumuz Regional State, near the Sudanese borderland. They have different social practices that distinguish them from others. They were part of the historical Gonga people who once lived on edges of the River Abay. Where were the early places of settlement of the Shinasha? What were the Social conditions, social changes and continuity in the Shinasha community? I address these questions by historically juxtaposing with social conditions and its dynamics with my interviews with the key informants and observations of changes in conditions of the Shinasha. This study highlights the geographic and background of the study area. The study tries to focus on the early settlement of the Shinasha and their conquest under imperial rule. It attempted to analyze the social organization of the Shinasha society. The significance of the paper is contributed to the understanding of the Social conditions and social changes and continuity of the Shinasha community in the historical outline. -

The Role of Community Radio for Integrated and Sustainable Development in Ethiopia: a Critical Review on the Holistic Approach D
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 10 December 2020 doi:10.20944/preprints202012.0260.v1 The Role of Community Radio for Integrated and Sustainable Development in Ethiopia: A Critical Review on the Holistic Approach Destaw Bayable Yemer Guna Tana Integrated Field Research & Development Center, Debre Tabor University, Ethiopia Email: [email protected] Abstract Community radios play a paramount role in the development of the community. Community radio stations have been highly engaged in addressing social, economic, cultural, educational, health, environmental, sanitation, and disaster issues effectively and strategically using local languages in context. Community radios are also used to express, and share indigenous views, thoughts, ideas, problems, and perspectives of local people. The purpose of this analysis is to explore the role of community radio for integrated and sustainable development in Ethiopia. It used a systematic narrative review. Nine research works and five assessments report were selected purposively and analyzed in a quantitative approach. Currently, in Ethiopia, there are 50 community radio stations that received broadcast licenses from Ethiopian Broadcast Authority with four types of licensing and broadcasting in 29 local languages. Community radio helps the community to identify their common goals, create holistic plans, monitor the progress of their developmental activities, and guide on sustainable development. It contributes to integrated and sustainable development in a collaborative and creative process that cultivates the social, economic, and political conditions needed for the community to succeed which aimed to improve and sustain the livelihoods of the community. However, the media can’t achieve its target goal to support the development activities and bring holistic development of the community. -

Debre Markos-Gondar Road
The Federal Democratic Republic of Ethiopia Ethiopian Roads Authority , / International Development Association # I VoL.5 ENVIRONMENTAL IMPACT ANALYSIS OF THE FIVE Public Disclosure Authorized ROADS SELECTED FOR REHABILITATION AND/OR UPGRADING DEBRE MARKOS-GONDAR ROAD # J + & .~~~~~~~~i-.. v<,,. A.. Public Disclosure Authorized -r~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ - -':. a _- ..: r. -. * .. _, f_ £ *.. "''" Public Disclosure Authorized Final Report October 1997 [rJ PLANCENTERLTD Public Disclosure Authorized FYi Opastinsilta6, FIN-00520HELSINKI, FINLAND * LJ Phone+358 9 15641, Fax+358 9 145 150 EA Report for the Debre Markos-Gondar Road Final Report TABLE OF CONTENTS TABLE OF CONTENTS ........................... i ABBREVIATIONS AND ACRONYMS ........................... iv GENERALMAP OF THE AREA ........................... v EXECUTIVE SUMMARY ........................... vi I. INTRODUCTION 1 1.1 Background 1 1.2 Location of the StudyArea. 1 1.3 Objectiveof the Study. 1 1.4 Approachand Methodologyof the Study. 2 1.5 Contentsof the Report. 3 2. POLICY,LEGAL AND INSTITUTIONALFRAMEWORK ....... 4 2.1 Policy Framework..Framewor 4 2.2 Legal Framework..Framewor 6 2.3 InstitutionalFramework. .Framewor 8 2.4 Resettlement and Compensation .12 2.5 Public Consultation 15 3. DESCRIPTIONOF THE PROPOSEDROAD PROJECT........... 16 4. BASELINEDATA ............. ........................... 18 4.1 Descriptionof the Road.18 4.2 Physical Environment nvironmt. 20 4.2.1 Climate and hydrology ................. 20 4.2.2 Physiography ............ ....... 21 4.2.3 Topography and hydrography ............ 21 4.2.4 Geology ....... ............ 21 4.2.5 Soils and geomorphology ................ 21 4.3 BiologicalEnvironment......................... 22 4.3.1 Land use and land cover .22 4.3.2 Flora .22 4.3.3 Fauna .22 4.4 Human and Social Environent .23 4.4.1 Characteristics of the population living by/alongthe road ..................... -

Research Article Factors Affecting Utilization of Voluntary HIV Counseling and Testing Services Among Teachers in Awi Zone, Northwest Ethiopia
Hindawi AIDS Research and Treatment Volume 2017, Article ID 9034282, 9 pages https://doi.org/10.1155/2017/9034282 Research Article Factors Affecting Utilization of Voluntary HIV Counseling and Testing Services among Teachers in Awi Zone, Northwest Ethiopia Woudneh Gereme Desta,1 Mulusew Alemneh Sinishaw,2 and Kelemu Dessie Bizuneh3 1 Health Promotion and Disease Prevention Core Process, Amhara National Regional State Health Bureau, Bahir Dar, Ethiopia 2Clinical Chemistry, Amhara Public Health Institute, Bahir Dar, Ethiopia 3Public Health Emergency Management, Awi Zone Health Department, Injibara, Ethiopia Correspondence should be addressed to Mulusew Alemneh Sinishaw; [email protected] Received 29 November 2016; Revised 16 March 2017; Accepted 5 April 2017; Published 23 April 2017 Academic Editor: Soraya Seedat Copyright © 2017 Woudneh Gereme Desta et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. HIV/AIDS affects the basic educational sector which is the most productive segment of the population and vital to the creation of human capital. The loss of skilled and experienced teachers due to the problem is increasingly compromising the provision of quality education in most African countries. The study was proposed to determine the magnitude of VCT utilization and assess contributing factors that affect VCT service utilization among secondary school teachers in Awi Zone. A cross-sectional study design was conducted among 588 participants in 2014. Self-administered questionnaire was used to collect data. Data was analyzed using SPSS version 16, presented as frequencies and summary statistics, and tested for presence of significant association with odds ratio at 95% CI.