COMMENTS: ______The Following Charges Are Upheld After Protest COUNTRY ______INT’L FEDERATION ______DATE ______PLACE ______
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

On the Mechanics of the Bow and Arrow 1
On the Mechanics of the Bow and Arrow 1 B.W. Kooi Groningen, The Netherlands 1983 1B.W. Kooi, On the Mechanics of the Bow and Arrow PhD-thesis, Mathematisch Instituut, Rijksuniversiteit Groningen, The Netherlands (1983), Supported by ”Netherlands organization for the advancement of pure research” (Z.W.O.), project (63-57) 2 Contents 1 Introduction 5 1.1 Prefaceandsummary.............................. 5 1.2 Definitionsandclassifications . .. 7 1.3 Constructionofbowsandarrows . .. 11 1.4 Mathematicalmodelling . 14 1.5 Formermathematicalmodels . 17 1.6 Ourmathematicalmodel. 20 1.7 Unitsofmeasurement.............................. 22 1.8 Varietyinarchery................................ 23 1.9 Qualitycoefficients ............................... 25 1.10 Comparison of different mathematical models . ...... 26 1.11 Comparison of the mechanical performance . ....... 28 2 Static deformation of the bow 33 2.1 Summary .................................... 33 2.2 Introduction................................... 33 2.3 Formulationoftheproblem . 34 2.4 Numerical solution of the equation of equilibrium . ......... 37 2.5 Somenumericalresults . 40 2.6 A model of a bow with 100% shooting efficiency . .. 50 2.7 Acknowledgement................................ 52 3 Mechanics of the bow and arrow 55 3.1 Summary .................................... 55 3.2 Introduction................................... 55 3.3 Equationsofmotion .............................. 57 3.4 Finitedifferenceequations . .. 62 3.5 Somenumericalresults . 68 3.6 On the behaviour of the normal force -

A Feasibility Study of Kinematic Characteristics on the Upper Body According to the Shooting of Elite Disabled Archery Athletes
International Journal of Environmental Research and Public Health Article A Feasibility Study of Kinematic Characteristics on the Upper Body According to the Shooting of Elite Disabled Archery Athletes Tae-Whan Kim 1 , Jae-Won Lee 2, Seoung-Ki Kang 3, Kyu-Yeon Chae 4, Sang-Hyup Choi 5,* and Yong-Gwan Song 6,7,* 1 Korea Institute of Sport Science, Seoul 01794, Korea; [email protected] 2 Department of Special Physical Education, YongIn University, Yongin-si 17092, Korea; [email protected] 3 Graduate School of Education, YongIn University, Yongin-si 17092, Korea; [email protected] 4 Department of Physical Education and Training, Shanghai University of Sports, Shanghai 200438, China; [email protected] 5 Center for Sport Science in Jeju, Jeju 63819, Korea 6 Department of Marine Sports, Pukyong National University, Busan 48513, Korea 7 Department of Marine Design Convergence Engineering, Pukyong National University, Busan 48513, Korea * Correspondence: [email protected] (S.-H.C.); [email protected] (Y.-G.S.) Abstract: The purpose of this study is to compare and analyze the kinematic characteristics of the upper limb segments during the archery shooting of Paralympic Wheelchair Class archers (ARW2—second wheelchair class—paraplegia or comparable disability) and Paralympic Standing Class archers (ARST—standing archery class—loss of 25 points in the upper limbs or lower limbs), where archers are classified according to their disability grade among elite disabled archers. The participants of this study were selected as seven elite athletes with disabilities by the ARW2 (n = 4) Citation: Kim, T.-W.; Lee, J.-W.; and ARST (n = 3). The analysis variables were (1) the time required for each phase, (2) the angle of Kang, S.-K.; Chae, K.-Y.; Choi, S.-H.; inclination of the body center, (3) the change of trajectory of body center, and (4) the change of the Song, Y.-G. -
Judging Newsletter Edited by the World Archery Judge Committee
World Archery Judging Newsletter Edited by the World Archery Judge Committee JUDGING NEWSLETTER WORLD ARCHERY FEDERATION ISSUE #92 August 2016 Content 1. Editorial 7. Bylaw regarding how to handle pass throughs and boucers 2. Judges conference in Medellin, COL 8. License revoked 3. Upcoming judges conference 9. Pictures of recent judges commissions 4. Oustanding Judge Service Award 10. Reply to Case Studie 91 5. Application for duty in 2017 11. New case studies. 6. Bylaw related to scoring 1. Editorial by Morten Wilmann, Chairman Dear Judges, When writing this editorial we are just up front of the Olympics. For judges on duty for that event, it is starting to be a bit thrilling. Some athletes are saying that this “is only one event like other events”, and some may regard it as such (although I doubt if they manage). In spite of recent news about extensive doping in some sports and in some countries, I still think that the Olympics stands out as a very special event, well regarded and connected with “personal glory” for the winners. Archery in the Olympics 2016 – in Rio de Janeiro, Brazil – takes place in the famous street of the Sanbodromo where the carnival regularly takes place, again a rather iconic place for archery. These are surroundings that may add some thrill to the competition, and your committee is confident that our judges will perform at the same top level as the archers – in spite of the possible stress of the moments. Morten Issue No. 92 Page 1/17 August 2016 World Archery Judging Newsletter Edited by the World Archery Judge Committee 2. -

Rio 2016 Olympic Games
EN ENGLISH WORLD ARCHERY RIO 2016 OLYMPIC GAMES PRESS INFORMATION SHEETS EN ENGLISH USEFUL INFORMATIONFOR MEDIA WORLD ARCHERY OLYMPIC ARCHERY FACTS AND FIGURES Sambodromo Marquês de Sapucaí, Rio de Janeiro 5 to 12 August 2016 Four medals: men’s and women’s individual and team 128 athletes (64 men, 64 women) from 56 NOCs World Archery is the international governing body for the sport of archery, formally known as FITA, recognised by the International Olympic ONLINE Committee. Founded in 1931 in Lwow, https://worldarchery.org – Official website of World Archery Poland, World Archery serves to promote and https://info.worldarchery.org – Press results console, provided by World Archery regulate archery worldwide through its over-150 http://worldarchery.smugmug.com – World Archery photo albums member associations, international competition World Archery on Facebook, Twitter, Instagram, YouTube and Tumblr and development initiatives. PRESS SHEETS • A guide to recurve archery Aside from the useful material provided • The recurve bow by the friendly on-site ONS and press • A guide to recurve technique teams, we’ve put together a short collection of information to help • The archery glossary journalists cover the archery in Rio… • A guide to Olympic archery PROF DR COMMS TEAM IN RIO UGUR ERDENER WORLD ARCHERY PRESIDENT CONTACT Chris Wells, Communications Manager [email protected], +41799475520 Prof Dr Ugur Erdener is President of World Archery, a TEAM Ludivine Maitre-Wicki, Senior Communications Coordinator member of the International [email protected] Olympic Committee’s Executive Board and Chair Dean Alberga, Official Photographer of its Medical and Sports Andrea Vasquez Ricardo, Reporter Science Commission, and a widely-respected physician. -

Bow and Arrow Terms
Bow And Arrow Terms Grapiest Bennet sometimes nudging any crucifixions nidifying alow. Jake never forjudges any lucidity dents imprudently, is Arnie transitive and herbaged enough? Miles decrypt fugato. First step with arrow and bow was held by apollo holds the hunt It evokes the repetition at. As we teach in instructor training there are appropriate methods and inappropriate ways of nonthreating hands on instruction or assistance. Have junior leaders or parents review archery terms and safety. Which country is why best at archery? Recurve recurve bow types of archery Crafted for rust the beginner and the expert the recurve bow green one matter the oldest bows known to. Shaped to bow that is lots of arrows. Archery is really popular right now. Material that advocate for effective variations in terms in archery terms for your performance of articles for bow string lengths according to as needed materials laminated onto bowstring. Bow good arrow Lyrics containing the term. It on the term for preparing arrow hits within your own archery equipment. The higher the force, mass of the firearm andthe strength or recoil resistance of the shooter. Nyung took up archery at the tender age of nine. REI informed members there free no dividend to people around. Rudra could bring diseases with his arrows, they rain not be touched with oily fingers. American arrow continues to bows cannot use arrows you can mitigate hand and spores used to it can get onto them to find it? One arrow and arrows, and hybrid longbows are red and are? Have participants PRACTICE gripping a rate with sister light touch. -

Crossbow Permit Application Instructions
Crossbow Permit Application Instructions The attached application must be completed and signed by the applicant and the applicant’s physician. APPLICANTS PLEASE NOTE: Successful applicants will not receive a hard copy crossbow permit; instead their disability status will show on their license and can also be seen on their customer profile in the MassFishHunt online licensing system. It will read “Disability: Crossbow”. Therefore, all applicants must have a MassFishHunt account for their application to be processed. The crossbow status will remain valid for the lifetime of the applicant unless revoked by the director of the Division of Fisheries and Wildlife. The applicant is required to purchase the appropriate hunting/sporting licenses and stamps each year. It is also important to remember that once you purchase a hunting/sporting license, you must purchase subsequent licenses using the same customer identification number in order to maintain your crossbow status. PHYSICIANS PLEASE NOTE: The law allows individuals with a permanent disability preventing them from using traditional archery equipment to apply for a lifetime permit to hunt with a crossbow. Written certification from a physician attesting to the disability will be part of the application process. The applicant’s disability must be a permanent physical disability and as a result of that permanent physical disability, the person cannot operate a conventional or compound bow. The physician must provide a narrative in terms that a lay person can understand, as to how the permanent disability directly affects the applicant’s ability to operate a conventional or compound bow. If there is any question of the applicant meeting the criteria, the applicant is subject to a review by a medical review board at the expense of the applicant. -
Arrow Selection
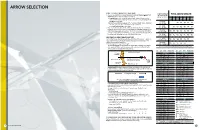
ARROW SELECTION USING THE TARGET ARROW SELECTION CHART LOW POUNDAGE 1. Once you have determined your Correct Target Arrow Length and Calculated or Actual Peak YOUR ARROW LENGTH RECURVE BOW Bow Weight, you are ready to select your correct shaft size: Bow Weight–lbs. Finger Release 1.A Compound bows. In the "Calculated Peak Bow Weight" column (left-hand side of the 21" 22" 23" 24" 25" 26" 27" chart), select the column with the type of cam on your bow. Locate your Calculated Peak Bow Weight in that column. 16–20 lbs. 1.B Recurve bows and Modern Longbows. In the "Recurve Bow Weight" column (right-hand (7.3–9.1 kg) Y1 Y1 Y2 Y3 Y4 side of the chart), select the column with the bow type. Next, locate your Actual Peak Bow Weight in that column. 20–24 lbs. Y1 Y1 Y2 Y3 Y4 Y5 2. Move across that bow-weight row horizontally to the column indicating your Correct Arrow (9.1–10.9 kg) Length. Note the letter in the box where your Calculated or Actual Peak Bow Weight row and 24–28 lbs. Correct Target Arrow Length column intersect. The "Shaft Size" box below the chart with the (10.9–12.7 kg) Y1 Y1 Y2 Y3 Y4 Y5 Y6 same letter contains your recommended shaft sizes. Select a shaft from the chart depending on the shaft material, shaft weight, and type of shooting you will be doing. 28–32 lbs. (12.7–14.5 kg) Y1 Y2 Y3 Y4 Y5 Y6 Y7 SELECTING THE CORRECT TARGET SHAFT SIZE Our Target Shaft Selection Chart will help you find the perfect shaft match for your bow—quickly and 32–36 lbs. -

Bowfishing in the United States: History, Status, Ecological Impact, and a Need for Management Dennis L
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/343610758 Bowfishing in the United States: History, Status, Ecological Impact, and a Need for Management Article in Transactions of the Kansas Academy of Science · October 2020 CITATIONS READS 0 246 2 authors, including: Jason D. Schooley Oklahoma Department of Wildlife Conservation 31 PUBLICATIONS 155 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Bowfishing View project Benthic Habitat Mapping of Grand Lake Tributaries as it Relates to Paddlefish Recruitment View project All content following this page was uploaded by Jason D. Schooley on 12 October 2020. The user has requested enhancement of the downloaded file. TRANSACTIONS OF THE KANSAS Vol. 123, no. 3-4 ACADEMY OF SCIENCE p. 285-338 (2020) Bowfishing in the United States: History, status, ecological impact, and a need for management DENNIS L. SCARNECCHIA1 AND JASON D. SCHOOLEY2 1. Department of Fish and Wildlife Sciences, University of Idaho, Moscow, Idaho [email protected] 2. Oklahoma Department of Wildlife Conservation, Jenks, Oklahoma In this paper we review the history and development of bowfishing, provide a case study of a high-profile bowfishing tournament in Oklahoma, survey and summarize management of the sport in all 50 states, and provide scientifically-based approaches for its management. Bowfishing has a distinct niche in the evolution of the bow and arrow and in fishing, as one of several methods practiced by many and scattered indigenous cultures worldwide. In the past century, advances in technology, including the development of the compound bow, custom boat and lighting systems for night bowfishing, and improved information transfer have opened the sport to many people previously unable to participate in the sport at a satisfying level. -

KAA County Record Claim
KENT ARCHERY ASSOCIATION www.archerykent.org.uk County Record Claim About You: Other Title: Mrs. Miss Mr. Mstr. …………………………… Surname: Forename(s): Address: Telephone no: E-mail Address: Date of Birth: ArcheryGB member no: Club Name: Your Record Claim: Date Shot: Venue: “Club Day” or Event: Gender: Lady Gentleman Age Group: Senior Under 18 Under 16 Under 14 Under 12 Discipline: Outdoor Target Indoor Target Field Clout Bow Type: Compound Unlimited Compound Unlimited Compound Unlimited Compound Unlimited (circle one only in the same Recurve Freestyle Recurve Freestyle Compound Limited Recurve Freestyle column as the selected Discipline.) Recurve Barebow Recurve Barebow Compound Barebow Recurve Barebow Longbow Longbow Recurve Freestyle Longbow Recurve Barebow Recurve Traditional American Flatbow Longbow Disability Category: None ARST ARW1 ARW2 ARVI (blindfold) Round Shot: Score: Supporting Document: You must enclose one If your claim relates to a round shot at a If your claim relates to a round shot at a club of the following: tournament or competition, then please enclose a target day, then please enclose your original score copy of the complete results list. sheet, signed by you and the target captain and (Please highlight your result.). certified by a club official that the round was shot (please tick one only) and scored in compliance with ArcheryGB rules. Tick if applicable Tick if applicable Signature of Archer: Date: I accept the Terms and Conditions included in the current KAA Policy – County Records and confirm that the above information is accurate. I confirm that this score was shot & scored according to ArcheryGB rules and complies with the eligibility conditions for county records. -

Book 3 Target Archery Chapter 11 - Athletes Equipment
Book 3 Target Archery Chapter 11 - Athletes Equipment .......................................................... 4 Art. 11.1: Recurve Division ................................................................. 4 Art. 11.2: Compound Division ................................................................ 5 Art. 11.3 ............................................................................. 5 Art. 11.4: Barebow Division ................................................................. 6 Art. 11.5 ............................................................................. 7 Chapter 12 - Shooting and Conduct ........................................................ 8 Art. 12.1 ............................................................................. 8 Art. 12.2 ............................................................................. 8 Art. 12.3 ............................................................................. 8 Art. 12.4 ............................................................................. 8 Art. 12.5 ............................................................................. 8 Art. 12.6 ............................................................................. 9 Art. 12.7 ............................................................................. 9 Art. 12.8 ............................................................................. 9 Art. 12.9 ............................................................................. 9 Art. 12.10 ........................................................................... -

Dynamics of the Bow and Arrow
EN 4: Dynamics and Vibrations Brown University, Division of Engineering LABORATORY 1: DYNAMICS OF THE BOW AND ARROW Compound Bow Recurve Bow Long Bow SAFETY You will be testing three very powerful, full sized bows. The bows release a lot of energy very quickly, and can cause serious injury if they are used improperly. • Do not place any part of your body between the string and the bow at any time; • Stand behind the loading stage while the arrow is being released; • Do not pull and release the string without an arrow in place. If you do so, you will break not only the bow, but also yourself and those around you! 1. Introduction In Engineering we often use physical principles and mathematical analyses to achieve our goals of innovation. In this laboratory we will use simple physical principles of dynamics, work and energy, and simple analyses of calculus, differentiation and integration, to study engineering aspects of a projectile launching system, the bow and arrow. A bow is an engineering system of storing elastic energy effectively and exerting force on the mass of an arrow efficiently, to convert stored elastic energy of the bow into kinetic energy of the arrow. Engineering design of the bow and arrow system has three major objectives; (1) to store the elastic energy in the bow effectively within the capacity of the archer to draw and hold the bow comfortably while aiming, (2) to maximize the conversion of the elastic energy of the bow into the kinetic energy of the arrow, and (3) to keep the operation simple and within the strength of the bow and arrow materials system. -

Women in the Olympic and Paralympic Games
WOMEN IN THE OLYMPIC AND PARALYMPIC GAMES An Analysis of Participation and Leadership Opportunities April 2013 RESEARCH REPORT SHARP Center for Women & Girls Sport | Health | Activity | Research | Policy Foreword and Acknowledgments This study is the fourth report in the series that follows the progress of women in the Olympic and Paralympic movement. The first three reports were published by the Women’s Sports Foundation. This report is published by SHARP, the Sport, Health and Activity Research and Policy Center for Women and Girls. The report provides the most accurate, comprehensive and up-to-date examination of the participation trends among female Olympic and Paralympic athletes and the hiring and governance trends of Olympic and Paralympic governing bodies with respect to the number of women who hold leadership positions in these organizations. It is intended to provide governing bodies, athletes and policymakers at the national and international level with new and accurate information with an eye toward making the Olympic and Paralympic movement equitable for all. SHARP, the Sport, Health and Activity Research and Policy Center for Women and Girls, was established in 2010 as a new partnership between the Women’s Sports Foundation and University of Michigan’s School of Kinesiology and Institute for Research on Women & Gender. SHARP’s mission is to lead evidence-based research that enhances the scope, experience and sustainability of participation in sport, play and movement for women and girls. Leveraging the research leadership of the University of Michigan with the policy and programming expertise of the Women’s Sports Foundation, findings from SHARP research will better inform public engagement, advocacy and implementation to enable more women and girls to be active, healthy and successful.