Report on Estimation of Mortality Impacts of Particulate Air Pollution in London
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Thades. [Essex
10~4 SHO THADES. [ESSEX. SHOPKEEPEitS contmued. Rutledge T, o Beaconsfield road, Can~ Shaw John, Witton Wood. .lane,. Rickett William iWalter, I Hart par ning Town E , Frinton-on~Sea ade~ Ilford lane, Ilford Sach Frederick, Copford,. Colchester Sheffield William, gz Chapel street,. Riddell A. 20 Queen's rd, Plaistow E Sadler Herbert, W1:ittle, Chelmsford Stratford E Riddleston Harry,. Layer-de-la-Haye, SaAller Herbsrt · F~rederick William, Sheldxake Mrs-. Katet 30 JI[udson rd. Colchester 74 Northgate street, Colchester Canning Town E Ridgewell Miss Grace, London road, Sage Mrs.Herbert, 8 King st.PlaistwE Shelley G. Galleywcxxi Com. Chlmsfd . Copford, Colchester Sains George, High st. Southminster Shelley U. J. Rivenhall, Witbam Ridgewell Miss Ruth, Netley road, Salmon Joseph, Stebbing, Chelmsford Shelton Mrs. Alice M. 3 Morant rd~ Newbury park, Ilford Salmon M. I Castle st.Saffron Walden Colchester Ridoutt James, ;r Norfolk road, Salmon Mrs. M.Io8Clarence rd.Grays Shelton Harry, North bank, Farm Higham hill, Walthamstow NE Salmon Mrs.Rosetta, Thorpe-le-Soken hill, Waltham Abbey :Rigg E. W. Mount Pleasant, Halstead Salmon S. Post office, High Beech, Shamming E. A. II7 North st.Halstd Riley A. Spring St.Netteswell,Harlow Loughton Sherlock Mrs. Rose, 124 Smart's lane,. Riley Mrs. .Alice, 58 Beaconsfield rd. Samson Ernest, 2 West road, South Loughton Walthamstow NE Stifford, Grays ., · Shipley John, 67 Exmouth road, Riley Harris J. Brentwood road,Heath Sansum James, 15 Rivett street, Walthamsto1v N E Park, Romford Canning Town E Shank Mrs.L.II Beatrice t>t.Plaistw E Binge Mrs. Thomas, Tolleshunt Sapsford Charles, Chigwell Row Shonk Stephen, 2 Cary road, J.,ey- Major, Witham Sargent )'d:rs. -

Hackney Planning Watch Response to Proposed
Hackney Planning Watch Response to Hackney Council on the proposal for the establishment of a Neighbourhood Forum covering the wards of Springfield, New River, Lordship and Cazenove January 2013 1 Introduction: These are our objections to the submitted proposal to formally designate the four wards: Springfield, New River, Lordship and Cazenove as a ‘Neighbourhood Forum’. As we understand it a group describing itself as the ‘Stamford Hill Neighbourhood Forum’ is seeking designation of four wards in Hackney (Springfield, New River, Lordship and Cazenove) as a ‘Neighbourhood Forum’. Hackney Planning Watch wishes to object in the strongest possible terms to this proposal. Although it will be evident from the four wards listed, the area proposed by the ‘Stamford Hill’ Neighbourhood Forum covers a much wider area than Stamford Hill and does in fact include Stoke Newington, Clissold Park and Upper Clapton. Hackney Planning Watch has a long history as a community organisation in the area. It was established over 15 years ago as a community group composed of local residents concerned about planning issues in Hackney, particularly the unlawful construction and the failure of the Council to deal properly with enforcement. In the last year some of our members have attempted to help build a cross-community alliance in order to develop a genuine consensual approach to the difficult planning issues in the area. These include, as well as enforcement issues, the lack of effective management of open space, protection of the environment, particularly in relation to drainage and tree preservation, and inadequate social infrastructure to meet the needs of the population. -

Neighbourhoods in England Rated E for Green Space, Friends of The
Neighbourhoods in England rated E for Green Space, Friends of the Earth, September 2020 Neighbourhood_Name Local_authority Marsh Barn & Widewater Adur Wick & Toddington Arun Littlehampton West and River Arun Bognor Regis Central Arun Kirkby Central Ashfield Washford & Stanhope Ashford Becontree Heath Barking and Dagenham Becontree West Barking and Dagenham Barking Central Barking and Dagenham Goresbrook & Scrattons Farm Barking and Dagenham Creekmouth & Barking Riverside Barking and Dagenham Gascoigne Estate & Roding Riverside Barking and Dagenham Becontree North Barking and Dagenham New Barnet West Barnet Woodside Park Barnet Edgware Central Barnet North Finchley Barnet Colney Hatch Barnet Grahame Park Barnet East Finchley Barnet Colindale Barnet Hendon Central Barnet Golders Green North Barnet Brent Cross & Staples Corner Barnet Cudworth Village Barnsley Abbotsmead & Salthouse Barrow-in-Furness Barrow Central Barrow-in-Furness Basildon Central & Pipps Hill Basildon Laindon Central Basildon Eversley Basildon Barstable Basildon Popley Basingstoke and Deane Winklebury & Rooksdown Basingstoke and Deane Oldfield Park West Bath and North East Somerset Odd Down Bath and North East Somerset Harpur Bedford Castle & Kingsway Bedford Queens Park Bedford Kempston West & South Bedford South Thamesmead Bexley Belvedere & Lessness Heath Bexley Erith East Bexley Lesnes Abbey Bexley Slade Green & Crayford Marshes Bexley Lesney Farm & Colyers East Bexley Old Oscott Birmingham Perry Beeches East Birmingham Castle Vale Birmingham Birchfield East Birmingham -

50Th Anniversary: Experiencing History(S) (PDF, 2.01MB)
asf_england_druck_1 22.07.11 10:01 Seite 1 Experiencing History(s) 50 Years of Action Reconciliation Service for Peace in the UK asf_england_druck_1 22.07.11 10:01 Seite 2 Published by: Action Reconciliation Service for Peace St Margaret's House, 21 Old Ford Road, London E2 9PL United Kingdom Telephone: (44)-0-20-8880 7526 Fax: (44)-0-20-8981 9944 E-Mail: [email protected] Website: www.asf-ev.de/uk Editors: Magda Schmukalla, Heike Kleffner, Andrea Koch Special thanks to Daniel Lewis for proof-reading, Al Gilens for his contributions and Karl Grünberg for photo editing. Photo credits: ASF-Archives p. 5, 6, 7, 8, 9, 10, 11, 12, 23, 26, 29, 34, 36, 37, 38, 40; International Youth Center in Dachau p. 30; Immanuel Bartz p. 14; Agnieszka Bieniek p. 4; Al Gilens p. 17, 22; Maria Kozlowska p. 28; Manuel Holtmann p. 25; Lena Mangold p. 41; Roy Scriver p. 33; Saskia Spahn p. 20 Title: ARSP volunteer Lena Mangold and Marie Simmonds; Lena Mangold Graphics and Design: Anna-Maria Roch Printed by: Westkreuz Druckerei Ahrens, Berlin 500 copies, London 2011 Donations: If you would like to make a donation, you can do so by cheque (payable to UK Friends of ARSP) or by credit card. UK Friends of ARSP is a registered charity, number 1118078. Donations account: UK Friends of ARSP: Sort Code: 08 92 99 Account No: 65222386 Thank you very much! 2 asf_england_druck_1 22.07.11 10:01 Seite 3 Table of Contents Introduction 4 by Dr. Elisabeth Raiser Working Beyond Ethnic and Cultural Differences 6 Voices of Project Partners Five Decades of ARSP in the UK: Turbulent Times 8 by Andrea Koch Reflecting History 12 by Dr. -
![(Essex.] East Ham. 80 Post Office](https://docslib.b-cdn.net/cover/5536/essex-east-ham-80-post-office-445536.webp)
(Essex.] East Ham. 80 Post Office
' (ESSEX.] EAST HAM. 80 POST OFFICE Surrogate for granting Licences of Marriage• ~for Baptut Chapel, North Rtreet ; Rev. W m .elements, ministr proving Wills, Rev. Charles Burney, M.A. Vicarage Baptist (Particular) Chapel, High st.; ministers various PuBLIC ScHooLs :- Independent Chapel, Parson's lane; Rev. John Reynolds, Free Grammar, High street; James Flavell, master miniQter; Rev. Joseph Waite, assistant minister St. Andrew'1 National, High street; John Bryon, Independent Chapel, Higb st.; Rev.Benj.Johnson,ministr master; Miss Mary Ann Earthy, mistress Friends' Meeting House, Colchester road National, Greenstead green; John Isaac, master; Miss PosTING HousEs:- Elizabeth Evens, mistress ' George,' Charles Nunn, Market bill Trinity National, Chapel street; Frederick M nrton, 'White Hart,' William Moye, High street master; Mrs. Emma Murton, mistress 'Bull,' John Elsdon, Bridue street Br-itish, Clipt hedges; William Stratton, master; Miss CoAcH TO BRAINTREE STATION.-The Eagle, evPry Elizabeth Freeman, mistress mornin~r & afternoon, sunday excepted, from the' White Infant, Clipt hedges; Miss Sarah Grey, mistress Hart,' Hi~h street PLACES OP WORSHIP:- CARRIERS TO:- St. ilndrew's Church, High street; Rev. Charles Burney, LONDON-William Howard's waggon, from Brid!le foot, M.A. vic11r; Rev. Fredk. Henry Gray,:s.A.. curate; Rev. to the 'Bull,' Aldgate, monday, tue:,day, thursday & friday Robert Helme, B.A. assistant curate COLCHESTER-Francis Mansfield, from his honsP, Trinity Holy Trinity Church, Chapel street; Rev. Duncan Fraser, street, tuesday, thursday & saturday; returns same days M.A. incumbent; Rev. Charles Cobb, l'tl.A.. curate BRAINTREE-Henry Cresswell, every day, & through to St. James's Church, Greenstead green; Rev. William London on friday Billopp, M.A. -

CHATHAM HISTORICAL SOCIETY Medway Chronicle 'Keeping Medway's History Alive'
Number 17 – Spring 2021 CHATHAM HISTORICAL SOCIETY Medway Chronicle 'Keeping Medway's History Alive' ▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬▬ Medway's Jewish Community ● Walter Brisac Chatham Town FC ● A “Custer Avenger” 1 CHATHAM HISTORICAL SOCIETY meets at St Stephen©s Church, Maidstone Road, Chatham, ME4 6JE on the second Wednesday of each month except January and August. Doors open at 7:15pm and the meeting starts at 7:30pm. News and information about Chatham Historical Society is available on the website: http://chathamhistoricalsoc.chessck.co.uk Officers of the committee President Vacancy Chairman Len Feist Hon Secretary Catharina Clement Hon Treasurer Barry Meade MEDWAY CHRONICLE is published by Chatham Historical Society. Editor Christopher Dardry Contributors as credited throughout the magazine. Views expressed by contributors do not necessarily represent the opinions of the Society. Copyright remains with the authors. The Editor welcomes articles for inclusion in future issues of the Medway Chronicle. Please submit text and images in electronic form by email to [email protected] or on paper to the editor at any of the society©s meetings. (The editor prefers email.) The Medway Chronicle is produced with the financial support of MEDWAY COUNCIL. Front cover: Chatham Town FC. Winners of the 1935-36 Kent Amateur League. 2 Index Victor Chidgey...............................................................................................................................................4 The beginnings of the Medway Jewish community.......................................................................................5 -

Housing, Credit and Brexit
Housing, Credit and Brexit Ben Ansell∗ Abstract Dozens of articles have been drafted attempting to explain the narrow vic- tory for the Leave campaign in Britain’s EU referendum in June 2016. Yet, hitherto, and despite a general interest in ‘Left Behind’ commentary, few writ- ers have drawn attention to the connection between the Brexit vote and the distribution of British housing costs. This memo examines the connection be- tween house prices and both aggregate voting during the EU referendum and individual vote intention beforehand. I find a very strong connection at the local authority, ward, and individual level between house prices and support for the Remain campaign, one that even holds up within regions and local authorities. Preliminary analysis suggests that housing values reflect long-run social differences that are just as manifest in attitudes to immigration as Brexit. Local ‘ecologies of unease’ (Reeves and Gimpel, 2012) appear a crucial force behind Brexit. This is a short memo on housing, credit and Brexit to be presented at the University of Wisconsin, Madison, April 2017. ∗Professor of Comparative Democratic Institutions, Nuffield College, University of Oxford. [email protected]. My acknowledgements and thanks go to Jane Gingrich for the provision of local economic and housing data. 1 1 Introduction If there is one saving grace of Brexit for the British higher education system it is a boom of Brexit studies that began pouring forth as the dust settled on June 24th 2016. Most scholars have coalesced around an understanding of Brexit that to some extent mirrors that implicit in Theresa May’s quasi hard Brexit strategy - Brexit was caused by both economic and cultural forces, with opposition to the European Union based on concerns about immigration and of declining cultural and social status rather than economic deprivation or actual migration levels per se (Kaufmann, 2016). -

JEWISH CIVILIAN DEATHS DURING WORLD WAR II Excluding Those Deaths Registered in the Metropolitan Borough of Stepney
JEWISH CIVILIAN DEATHS DURING WORLD WAR II excluding those deaths registered in the Metropolitan Borough of Stepney Compiled by Harold Pollins This list may not be used elsewhere without consent. ©Harold Pollins For a full description of the contents of this list please see the description on the list of datasets Harold Pollins acknowledges the tremendous assistance of Harvey Kaplan who collated the Glasgow deaths Date of Additional Information Surname Given Name Place of Residence Place of Death Age Spouse Name Father's Name Mother's Name Death Comments and Notes 34 Twyford Avenue, AARONBERG Esther Acton 18‐Oct‐40 40 Ralph 34 Twyford Avenue, AARONBERG Ralph Acton 18‐Oct‐40 35 Esther 39 Maitland House, Bishop's Way, Bethnal Bethnal Green Tube AARONS Betty Diane Green Shelter 03‐Mar‐43 14 Arnold In shelter accident BROOKSTONE Israel 41 Teesdale Street Tube shelter 03‐Mar‐43 66 Sarah In shelter accident in shelter accident. Light Rescue Service. Son of Mr and Mrs B Lazarus of 157 Bethnal LAZARUS Morris 205 Roman Road Tube shelter 03‐Mar‐43 43 Rosy Green Road 55 Cleveland Way, Mile MYERS Jeffrey End Tube shelter 03‐Mar‐43 6 Isaac Sophie in shelter accident 55 Cleveland Way, Mile MYERS Sophie End Tube shelter 03‐Mar‐43 40 Isaac Charterhouse Clinic, Thamesmouth, Westcliff‐ Weymouth St, Obituary Jewish Chronicle ABRAHAMS Alphonse Nathaniel on‐Sea Marylebone 17‐Sep‐40 65 Evelyn May 15.11.1940 page 6 98 Lewis Trust Buildings, injured 4 January 1945 at ABRAHAMS Benjamin Dalston Lane, Hackney German Hospital 08‐Jan‐45 56 Leah Forest Road Library 96 Tottenham Court Polish National. -

Haggerston to Hoxton Wild Walk
Get Hackney Healthy Hackney Wild Walks This is an interesting Haggerston to Hoxton: walk with lots to see! You can bring your scooter as there are no steps. It’s 2.1km if you take a giant snake, a stone circle the Overground back to the start or 2.6km if & a secret garden you walk. Start at Haggerston On a black silent night that a silver moon crowned, Station, you should see A snake emerged from the Underground. Stonebridge Gardens next A turquoise monster, it made hardly a sound, to the station. Go through As it slithered its way through Haggerston town. the gate to find a Down Kingsland Road it slowly unwound, surprising slithery sight. Til it went to sleep on a grassy mound. You can climb and clamber, jump up and down, On his coils coiled around this little playground. Haggerston Station STEAN STREET E8 London Borough of Hackney After the second bridge, take the ramp back up behind you onto Queensbridge Road. What do you think of the huge Shoreditch sign? Under the railway is a beautiful peace mural designed by local children – how many symbols can you see? SHOREDITCH You’ve already done 300m. Turn left and take the ramp on the right down onto the tow path. You will go under Ones, twos, threes and fours, two bridges – Can you count canoes, WHISTON watch out for paddles and oars? ROAD E2 cyclists! Ting! London Borough of Hackney Ting! Haggerston Park KINGSLAND Stone This stone circle Circle ROAD E2 Turn right London Borough of Hackney must have some up Appleby, a treat history, but now is in store! Alternate to us it’s just a return route up St Mary's Secret mystery! Kingsland Road Garden, let's go and explore. -

DOWNLOAD London.PDF • 5 MB
GORDON HILL HIGHLANDS 3.61 BRIMSDOWN ELSTREE & BOREHAMWOOD ENFIELD CHASE ENFIELD TOWN HIGH BARNET COCKFOSTERS NEW BARNET OAKWOOD SOUTHBURY SOUTHBURY DEBDEN 9.38 GRANGE PARK PONDERS END LOUGHTON GRANGE BUSH HILL PARK COCKFOSTERS PONDERS END 6.83 4.96 3.41 OAKLEIGH PARK EAST BARNET SOUTHGATE 4.03 4.01 JUBILEE CHINGFORD WINCHMORE HILL BUSH HILL PARK 6.06 SOUTHGATE 4.24 CHINGFORD GREEN TOTTERIDGE & WHETSTONE WINCHMORE HILL BRUNSWICK 2.84 6.03 4.21 ENDLEBURY 2.89 TOTTERIDGE OAKLEIGH EDMONTON GREEN LOWER EDMONTON 3.10 4.11 3.57 STANMORE PALMERS GREEN HASELBURY SOUTHGATE GREEN 5.94 CHIGWELL WOODSIDE PARK PALMERS GREEN 5.23 EDMONTON GREEN 3.77 ARNOS GROVE 10.64 LARKSWOOD RODING VALLEY EDGWARE SILVER STREET MILL HILL BROADWAY 4.76 MONKHAMS GRANGE HILL NEW SOUTHGATE VALLEY HATCH LANE UPPER EDMONTON ANGEL ROAD 8.04 4.16 4.41 MILL WOODHOUSE COPPETTS BOWES HATCH END 5.68 9.50 HILL MILL HILL EAST WEST FINCHLEY 5.12 4.41 HIGHAMS PARK CANONS PARK 6.07 WEST WOODFORD BRIDGE FINCHLEY BOUNOS BOWES PARK 3.69 5.14 GREENBOUNDS GREEN WHITE HART LANE NORTHUMBERLAND PARK HEADSTONE LANE BURNT OAK WOODSIDE WHITE HART LANE HAINAULT 8.01 9.77 HALE END FAIRLOP 4.59 7.72 7.74 NORTHUMBERLAND PARK AND BURNT OAK FINCHLEY CENTRAL HIGHAMS PARK 5.93 ALEXANDRA WOOD GREEN CHURCH END RODING HIGHAM HILL 4.58 FINCHLEY 4.75 ALEXANDRA PALACE CHAPEL END 3.13 4.40 COLINDALE EAST 5.38 FULLWELL CHURCH 5.25 FAIRLOP FINCHLEY BRUCE 5.11 4.01 NOEL PARK BRUCE GROVE HARROW & WEALDSTONE FORTIS GREEN GROVE TOTTENHAM HALE QUEENSBURY COLINDALE 4.48 19.66 PINNER 3.61 SOUTH WOODFORD HENDON WEST -
Details by Ward
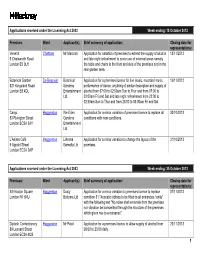
Applications received under the Licensing Act 2003 Week ending: 18 October 2013 Premises: Ward Applicant(s): Brief summary of application: Closing date for representations: Venerdi Chatham Mr Manconi Application for variation of premises to extend the supply of alcohol 12/11/2013 9 Chatsworth Road and late night refreshment to cover use of external areas namely London E5 0LH the table and chairs to the front and side of the premises and in the rear garden area. Botanical Garden De Beauvoir Botanical Application for a premises licence for live music, recorded music, 19/11/2013 321 Kingsland Road Gardens performance of dance, anything of similar description and supply of London E8 4DL Entertainment alcohol from 07:00 to 02:00am Sun to Thur and from 07:00 to Ltd 03:00am Fri and Sat and late night refreshment from 23:00 to 02:30am Sun to Thur and from 23:00 to 03:30am Fri and Sat Cargo Haggerston We Eden Application for a minor variation of premises licence to replace all 30/10/2013 83 Rivington Street Gardens conditions with new conditions. London EC2A 3AY Entertainment Ltd L’Anima Café Haggerston L'Anima Application for a minor variation to change the layout of the 31/10/2013 9 Appold Street Gemella Ltd premises. London EC2A 2AP Applications received under the Licensing Act 2003 Week ending: 25 October 2013 Premises: Ward Applicant(s): Brief summary of application: Closing date for representations: 8/9 Hoxton Square Haggerston Dusty Application for a minor variation to premises licence to replace 07/11/2013 London N1 6NU Bottoms Ltd condition 31 "Acoustic lobbies to be fitted to all entrances / exits" with the following text "No noise shall emanate from the premises nor vibration be transmitted through the structure of the premises which gives rise to a nuisance". -

Pharmaceutical Needs Assessment for Hammersmith & Fulham
θωερτψυιοπασδφγηϕκλζξχϖβν µθωε ρτψυιοπασδφγηϕκλζξχϖβνPharmaceutical Needsµθωερτ ψυιοπασδφγηϕκλζξχϖβνAssessment forµθωερτψυι οπασδφγηϕκλζξχϖβνµθωερτψυιοπ ασδφΠΠΠΗγηϕκλζξχϖβνHammersmithµ &θωερτψυ ιοπασδφγηϕκλζξχϖβνFulhamµ θωερτψυιοπ ασδφγηϕκτψυιοπασδφγηϕκλζξχϖβν µθωερτψυιοπασδφγηϕκλζξχϖβν2018 - 2021 µθ Compiled by Healthy Dialogues Ltd Table of Contents Executive Summary ............................................................................. 3 Chapter 1 – Introduction ....................................................................... 7 Role of Pharmacies ....................................................................................... 7 Purpose of the Pharmaceutical Needs Assessment ........................................... 7 Policy Background Relating to the PNA ........................................................... 8 Chapter 2 - Local Health and Wellbeing Priorities ................................ 10 Chapter 3 - The Pharmaceutical Needs Assessment Process .............. 12 Methodological considerations ...................................................................... 12 Governance and steering group .................................................................... 14 Regulatory consultation process and outcomes .............................................. 14 Additional Considerations regarding pharmacy funding .................................... 14 Chapter 4 - Health Needs and Population Changes .............................. 16 Population Characteristics and Projections ....................................................