G Incapacitation in Aerobatic Pilots: a Flight Hazard
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ff 89/6 Copy
$3 vol libre • free flight 6/89 Dec - Jan POTPOURRI SAC was informed by Sport Canada on the 10th of July that we are not eligible for funding for 1989-90 and until further notice. Thus we are now totally on our own. The average yearly grant from 1979 to 1988 in 1989 dollars was $14,000, or $16 per person. Perhaps it’s a good thing as planning in an atmosphere of doubt is not conducive to good health and efficient use of funds. The cutback was not unexpected and steps were taken early on to ease the effects of this loss of revenue. Imaginative planning in our small store and a good response from our members through the use of the “Soaring Stuff” inserts resulted in in- creased sales. We will also receive higher than projected invest- ment income essentially due to careful cash management and short-term interest rates, which have remained higher for longer than generally expected. In addition, a small gain in projected receipts from an unexpected increase in membership – now at 1423 – which is the first time since 1982 that we have passed 1400. Total expenditures should come in well below budget projection, primarily as a result of scaling back meetings and travel expenditures. On balance it seems fair to say that a combination of some tight fistedness on the expenditure side and a bit of luck on the revenue side will leave SAC in a financially stronger position than was expected at the beginning of the season, despite the cutting off of govern- ment funding. -

CHIPPY Restoringdarin LACRONE
FEBRUARY 2016 TM Restoring CHIPPY RestoringDARIN LACRONE Winning a Bronze Lindy at Oshkosh by Mark Meredith In naval aviation we called Super Chipmunk right cheek cowl- But we skipped TFOA report- it Things Falling Off Air- ing is now in a Maryland farmer’s ing. Embarrassed by my negligence craft. We had a program for it, field, somewhere over yonder. The in losing a big piece of an airplane of course, with formatted official cowling departed while rolling up- that everyone told me not to buy, reporting under the header TFOA. right from a half-Cuban, tumbling my brother, Chris, and I flew home Too often it was reporting lit- down over our heads. It missed the at low power, landed, and high- tle blue practice bombs that went tail and my brother, exposed in the tailed it for the hangar. I had maybe astray (oops), or canopies that front cockpit, but pretty much ru- 20 hours in the logbook including blew off at 40,000 feet and became ined a golden fall afternoon of gen- the ferry home from Florida, all of someone’s backyard greenhouse. tleman aerobatics. So began my it flown with trepidation because But that was then and this is now: education as the new owner of a this was clearly a project plane. Who should I report this to? My very tired air show bird. The intent had been to fly it some, www.iac.org 5 Above, Chipmunk BF370 began life in the RAF (1951-55), attached to the Chipmunk BF370 left the RAF for No. -

2007 Chapter Officers
OUR ROOTS: AEROBATICS IN THE ‘60’s With the onset of cold weather and the lack of chapter news, I will take liberties with this installment to share some of our heritage. I first participated in formal aerobatic competition in 1968. At that time US competition was sanctioned by the ACA (Aerobatic Club of America) and was divided into three competition categories: Primary, Advanced and Unlimited. After three wins, Primary contestants were required to move up. In 1968 I was married with two boys and earning a whopping $820 a month as a chemistry instructor. I competed that year in Primary with a stock 65 hp J3 Cub. The ’68 Primary sequence was well designed and accommodated good energy management: Spin Loop Immelman 45 down snap Half Cuban Barrel Roll Hammerhead Slow Roll Reverse Half Cuban Four Point Roll Those of us without inverted fuel often experienced loss of power during the Immelman and appreciated the subsequent 45 down line in order to restart our engines. Contests in ’68 were held at Monroe, LA; Vandalia, IL; Ottumwa, IA; Rockford (Harvard) IL and the Nationals at Oak Grove airport, Fort Worth, TX. One of the pleasures of this era was the wide variety of competing aircraft. They included a lively mix of both monoplanes (clipped Cub and T-Craft, Luscombe, Ryan PT-22 and STA, Citabria, Stitts Playboy, Cassutt Racer, Chipmunk, Dart, and Zlin) and biplanes (Smith Miniplane, EAA Biplane, Pitts Special, PJ-260, Stampe, Bucker Jungmeister and Jungmann, Great Lakes, Wacos, and Stearman). Many of these early airplanes were modified to enhance their strength, control systems and to implement inverted power. -
VA Vol 9 No 6 Jun 1981
STRAIGHT AND LEVEL By Brad Thomas President Antique/Classic Division By the end of June, summer has officially arrived and many fly-ins will have occurred. In making vaca tion plans undoubtedly Oshkosh will be included by most of us. This June issue of The VINTAGE AIRPLANE also lists the Antique/Classic Division officers and direc tors who are running for reelection this year. This past January a nominating committee was appointed, with Morton Lester named as Chairman, and he reports the following have been nominated for the positions indi cated: who might be interested but do not know of our existence. Jack Winthrop, Vice President As a reminder, the purposes of the Antique/Classic E. E. "Buck" Hilbert, Treasurer Division are printed below: Claude L. Gray, Jr., Director 1. To encourage, aid and engage in research, including Dale A. Gustafson, Director that of a scientific nature, for the improvement and John R. Turgyan, Director better understanding of aviation. Ronald Fritz, Director 2. To encourage and aid the retention and restoration A resume of each nominee is also incl uded in this of antique, historical and classic aircraft. issue. Ballots will be mailed to members under separate 3. To establish a library devoted to the history of avia cover in June. Each candidate named above is duly tion and to the construction, repair, restoration, main qualified to serve the Division and each is a dedicated tenance and preservation of aircraft, particularly an supporter of the entire EAA movement. tique, historical and classic aircraft and engines. Included with each ballot in the June mailing will 4. -
Circular Administration
Advisory US.Depanment 01 Tronsporlolion Federal Aviation Circular Administration Subject: A HAZARD IN AEROBATICS: Date: 2/28/84 At No: 91-61 EFFECTS OF G-FORCES ON PILOTS Initiated by: AFO- 800 ; Change: AAM-500; AAC-100 1. PURPOSE. Because aerobatic flying subjects pilots to gravitational effects (G's) that can impair their ability to safely operate the aircraft, pilots who engage in aerobatics, or those who would take up such activity, should understand G's and some of their physiological effects. This circular provides background information on G's, their effect on the human body, and their role in safe flying. Suggestions are offered for avoiding problems caused by accelerations encountered in aerobatic maneuvers. 2. BACKGROUND. Aerobatic flying demands the best of both aircraft and pilot. The aircraft must be highly maneuverable, yet tolerant of G-loads. The pilot must possess skill and physiological stamina. He or she must be daring, yet mindful of the aircraft's limitations as well as his or her own. Federal Aviation Administration (FAA) Advisory Circular No. 91-48, "Acrobatics-Precision Flying with a Purpose," dated June 29, 1977, discusses some of the airworthiness and operational aspects of aerobatics, but does not consider biomedical factors. The most important of these biomedical factors is the pilot's response to accelerations (or G-loading). The major physiological effects of G-loaaing vary from reduced vision to loss of consciousness. The pilot who understands these effects will be better able to cope with them so that he or she can continue the sport of aerobatic flying. J. -

Stearman Aerobatics
( SFA'OUIFI" OCIOBEF1990 3 AEROBATICS U.S.NAVY Fep ntedlbm: U.S.NAVY PRIMARY FLIGHT TFAINING MANUAL 1 Juy, I945 NAVALAIF TRAINING COMMAND CHIEFOF NAVALAIB PRIMAFYIFAINING o sFA 'OUrFrr'. @TOAEB1990 5 AEROBATICS Import it Regsrdl6 oI sherhd o! not . part.llar manelver lsdecrib€d in th€ lollowlngp!s.i you aE to prc. Youare now !e.dy lor rhar shse in yrlr tEinlnsas a Nav.l dc. only thosemaneuveB d€m6nst6i.d .nd p@scdbedby Aviarlor rowad {hlch you have been lookins loMad wlrh you LndrucrorIn rh2 oda preserr€dby ih€ syllabus keenanricLp,rion, p€rhars nor unmix€dwih 5omeI€€tinqs ot AII .ercb.ric d|l be comDl.r..l !r lad 2,0lr0 f€€r missrvlns.Uk€ manybclore you, 9ou are piobably wondelhg sherhff or nor you can \ak€ i1" ai dre same6me |rboilng Tl ! L nor h.nated .ldtud€ trt .cr!.I .ldtude uider rhedelusionrhanh?maitolasood pilor b hcsktllh aeob.hca $e aE,e'. ol .ou6e. is rhai you qtn be .bl. to "rake ",bu|h? querion$ltbe lnethsornoryouon "h-ue I Yourel€ry b€ll lr sh@ld b. lan.ned snugly.bur mr b Ll" T@ rony c.d?a helore ylo hde (fie ro Ei.t in C r.se, rsh& d ro inrerl€e s h yor les @€m€nis. Ah. simplybea u.e rheyrs'e tanied aky" birthdr entolnenr ol ch4* rh€ shouldq h.66 aerob.rt and r d6n€ ro bercm€ aerbaric expds Tiey 2 Be €@ nor akn in l@kjns lor dhq airEft in your nesleded rh€ prc.kion ert iirrodlc€d i. -

National Transportation Safety Board Aviation Accident Final Report
National Transportation Safety Board Aviation Accident Final Report Location: RANCHO MURIETA, CA Accident Number: LAX88FA015 Date & Time: 10/15/1987, 1528 PDT Registration: N121FJ Aircraft: DASSAULT-BREGUET DA 10 Aircraft Damage: Destroyed Defining Event: Injuries: 3 Fatal Flight Conducted Under: Part 91: General Aviation - Positioning Analysis THE ACFT FLEW TO THE ARPT FOR A SALES DEMO FLT. THE CREW BOARDED THE ACFT AND TAXIED OUT FOR DEP. WITNESSES, INCLUDING TWO PLTS WITH AEROBATIC EXP, WATCHED THE ACFT DEP, MAKE A LEFT TRAFFIC PATTERN AND DO A LOW FLY-BY DOWN THE RWY. AT THE DEP END OF THE RWY, THE ACFT PITCHED UP INTO A STEEP CLIMB. AT 600 FT AGL, THE ACFT ENTERED A LEFT AILERON ROLL, WHICH THE WITNESSES SAID WAS 'SMOOTH, COORDINATED AND WITH THE NOSE ON THE POINT.' AT THE INVERTED POINT OF THE ROLL, THE ROLL CHANGED FROM AN AILERON TO A BARREL ROLL. ONE PILOT WITNESS SAID THAT IT APPEARED THE 'CREW LOST IT AT THE TOP' AND THAT THE CREW 'HELD THE BACK PRESSURE TOO LONG AT THE TOP.' AT THE 270 DEG POINT OF THE ROLL, THE ACFT WAS SEEN TO 'FALL OUT' OR 'DISH OUT' OF THE ROLL; IT RECOVERED TO WINGS LEVEL FLT AT ABOUT 100 FT AGL IN A VERY NOSE HIGH ATTITUDE SETTLING INTO THE GROUND WITH A HIGH VERTICAL DESCENT RATE. NO PREIMPACT ENG OR CONTROL SYSTEM MALFUNCTIONS WERE FOUND. Probable Cause and Findings The National Transportation Safety Board determines the probable cause(s) of this accident to be: IN FLIGHT LOSS OF CONTROL BY THE PILOT FLYING WHILE PERFORMING AN INTENTIONAL LOW LEVEL AEROBATIC MANEUVER. -
Sportsman Sequence but Sequence
SPORT MARCH 2011 OFFICIALFICIAL MAGAZINEMA NENE ofof thet INTERNATIONALN TION AEROBATIC CLUB • First Japanese How to Fly the Contest SPORTSMAN •Cheap Acro SEQUENCE Drive one. 2011 Ford Mustang All Legend, No Compromise The Privilege of Partnership The legendary 5.0L V8 returns to the Mustang GT, delivering 412 HP EAA members are eligible for special pricing on Ford Motor Company and 26 MPG. The 3.7L V6 boasts 305 HP and 31 MPG – new standards vehicles through Ford’s Partner Recognition Program. To learn more in the class! on this exclusive opportunity for EAA members to save on a new Ford vehicle, please visit www.eaa.org/ford. State-of-the-art technology includes: Twin-Independent Variable Cam Timing (Ti-VCT), SYNC in-car connectivity, and AdvanceTrac electronic stability control. VEHICLE PURCHASE PLAN OFFICIAL MAGAZINE of the INTERNATIONAL AEROBATIC CLUB Vol. 40 No.3 March 2011 A PUBLICATION OF THE INTERNATIONAL AEROBATIC CLUB CONTENTS “Somebody said, “Well, they met a black bear when they were making the corner markers. Maybe it’s true. ” Yuichi Tagaki FEATURES 06 Flying the 2011 Sportsman Known John Morrisey 18 Full Circle Dave Watson 22 Cheap Acro Will Tyron 28 Japan’s First Contest Cutting acro out of the jungle Yuichi Takagi COLUMNS 03 / President’s Page Doug Bartlett DEPARTMENTS 02 / Letter From the Editor 04 / Sun ‘n Fun Speakers 26 / 2010 Regional Results THE COVER 30 / Contest Calendar and Advertisers Index Photo by Laurie Zaleski. 31 / FlyMart and Classifieds PHOTOGRAPHY COURTESY YUICHI TAGAKI REGGIE PAULK COMMENTARY / EDITOR’S LOG OFFICIAL MAGAZINE of the INTERNATIONAL AEROBATIC CLUB PUBLISHER: Doug Bartlett IAC MANAGER: Trish Deimer EDITOR: Reggie Paulk SENIOR ART DIRECTOR: Phil Norton DIRECTOR OF PUBLICATIONS: Mary Jones COPY EDITOR: Colleen Walsh CONTRIBUTING AUTHORS: Doug Bartlett John Morrissey Reggie Paulk Yuichi Tagaki Will Tyron Dave Watson IAC CORRESPONDENCE International Aerobatic Club, P.O. -
DCS: Su-27 Flanker Flight Manual
[SU-27] DCS DCS: Su-27 Flanker Eagle Dynamics i Flight Manual DCS [SU-27] DCS: Su-27 for DCS World The Su-27, NATO codename Flanker, is one of the pillars of modern-day Russian combat aviation. Built to counter the American F-15 Eagle, the Flanker is a twin-engine, supersonic, highly manoeuvrable air superiority fighter. The Flanker is equally capable of engaging targets well beyond visual range as it is in a dogfight given its amazing slow speed and high angle attack manoeuvrability. Using its radar and stealthy infrared search and track system, the Flanker can employ a wide array of radar and infrared guided missiles. The Flanker also includes a helmet-mounted sight that allows you to simply look at a target to lock it up! In addition to its powerful air-to-air capabilities, the Flanker can also be armed with bombs and unguided rockets to fulfil a secondary ground attack role. Su-27 for DCS World focuses on ease of use without complicated cockpit interaction, significantly reducing the learning curve. As such, Su-27 for DCS World features keyboard and joystick cockpit commands with a focus on the most mission critical of cockpit systems. General discussion forum: http://forums.eagle.ru ii [SU-27] DCS Table of Contents INTRODUCTION ........................................................................................................... VI SU-27 HISTORY ............................................................................................................. 2 ADVANCED FRONTLINE FIGHTER PROGRAMME ......................................................................... -
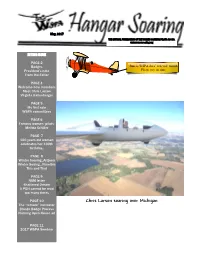
Chris Larson Soaring Over Michigan the “Remote” Instructor Bronze Badge Process Nutmeg Open House Ad
May, 2017 THE OFFICIAL PUBLICATION OF THE WOMEN SOARING PILOTS ASSOC. www.womensoaring.org IN THIS ISSUE PAGE 2 Badges June is WSPA dues’ renewal month President’s note Please pay on time From the Editor PAGE 4 Welcome new members Meet Chris Larson Virginia Gallenberger PAGE 5 My first solo WSPA committees PAGE 6 Famous women pilots: Melitta Schiller PAGE 7 100 years old woman celebrates her 100th birthday.. PAGE 8 Winter Soaring..Arizona Winter Soaing...Namibia This and That PAGE 9 NSM letter Shattered Dream A POH cannot be read too many times PAGE 10 Chris Larson soaring over Michigan The “remote” instructor Bronze Badge Process Nutmeg Open House ad PAGE 11 2017 WSPA Seminar page 2 May 2017 THE WOMEN SOARING PILOTS Badges ASSOCIATION (WSPA) WAS (reported through May 2017 A Badge FOUNDED IN 1986 AND IS Coleen Cameron, CO AFFILIATED WITH THE SOARING C Badge Maryam Ali, VA SOCIETY OF AMERICA Coleen Cameron, CO BOARD B Badge Mary Rust ,President Coleen Cameron, CO From the Editor 26630 Garret Ryan Ct. Recently, I got an e-mail from one of our members inquir- Hermet, CA 92544-6733 President’s Note ing why we need separate Charlotte Taylor, Vice President women contests or listing women Your newly elected WSPA Board Mem- 4206 JuniataSt. records separately. This also falls bers are off to a great start working on a St. Louis, MO 63116 into the category ‘why are there variety of projects! Though we have been so few women in aviation and in working on line together for 4 months, Joan Burn, Secretary soaring especially?’ WSPA and many of us have not met each other face 212 Marian Ct. -

Selig-2014-Jofac-Fli
JOURNAL OF AIRCRAFT Vol. 51, No. 6, November–December 2014 Real-Time Flight Simulation of Highly Maneuverable Unmanned Aerial Vehicles Michael S. Selig∗ University of Illinois at Urbana–Champaign, Urbana, Illinois 61801 DOI: 10.2514/1.C032370 This paper focuses on full six degree-of-freedom aerodynamic modeling of small unmanned aerial vehicles at high angles of attack and high sideslip in maneuvers performed using large control surfaces at large deflections for aircraft with high thrust-to-weight ratios. Configurations, such as this, include many of the currently available propeller- driven radio-controlled model airplanes that have control surfaces as large as 50% chord, deflections as high as 50 deg, and thrust-to-weight ratios near 2∶1. Airplanes with these capabilities are extremely maneuverable and aerobatic, and modeling their aerodynamic behavior requires new thinking because using traditional stability- derivative methods is not practical with highly nonlinear aerodynamic behavior and coupling in the presence of high prop-wash effects. The method described outlines a component-based approach capable of modeling these extremely maneuverable small unmanned aerial vehicles in a full six degree-of-freedom real-time environment over the full 180 deg range in angle of attack and sideslip. Piloted flight-simulation results for four radio-controlled/unmanned- aerial-vehicle configurations having wingspans in the range from 826 mm (32.5 in.) to 2540 mm (100 in.) are presented to highlight the results of the high-angle aerodynamic modeling approach. Maneuvers simulated include tailslides, knife-edge flight, high-angle upright and inverted flight, rolling maneuvers at high angle, and an inverted spin of a biplane. -
PDF Version August September 2009
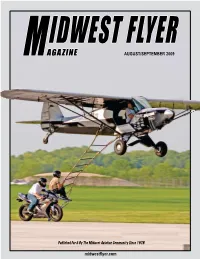
IDWEST FLYER M AGAZINE AUGUST/SEPTEMBER 2009 Published For & By The Midwest Aviation Community Since 1978 midwestflyer.com Cessna Sales Team Authorized Representative for: J.A. Aero Aircraft Sales IL, WI & Upper MI Caravan Sales for: 630-584-3200 IL, WI & MO W Largest Full-Service Cessna Dealer in Midwest W See the Entire Cessna Propeller Line – From SkyCatcher Thru Caravan W� Delivery Positions on New Cessna 350 & 400! Scott Fank – Email: [email protected] Aurora Airport (ARR) Dave Kay – Email: [email protected] 43W730 U.S. Rt 30 • Sugar Grove, IL 60554 Visit Us Online at (630) 549-2100 www.jaaero.com (630) 466-4374 Fax LookingLooking forfor thethe BestBest Service,Service, FacilitiesFacilities andand LocationLocation inin Chicago?Chicago? J.A. Air Center NOW OPEN! We’ve Got You Covered! Toll Free (877) 905-2247 Direct Highway Access to Chicago (Zero Stoplights to Downtown!) Local (630) 549-2100 W Award-Winning Avionics W Maintenance Unicom 122.95 W Aircraft Sales & Acquisition W Office/Hangar Rentals W FBO Services W Aircraft Detailing www.jaair.com• FBO Services W Charter Chicago / Aurora ARR H ONDAJET MIDWEST THE JET. REDEFINED. ENGINEERE D FOR PE RFORMANCE . DESIGNE D FOR DESIRE . BUILT FOR PE RFE CTION. EXPERIE NCE HONDAJE T. INTE RNATIONAL AIRP ORT, D E S MOINES , IOWA 50321 877.686.0028 • HONDAJETMIDWEST.COM © 2008 Honda Aircraft Company, Inc. MidwestHondaJet_Feb09.indd 1 1/12/09 5:07:52 PM Vol. 31. No. 5 ContentsContents Issn:0194-5068 ON THE COVER: Flying a Super Cub, Kyle Franklin of Neosho, Mo., attempts IDWEST FLYER a motorcycle-to-plane transfer of stuntman Andy Roso of Iowa City, Iowa, while Brandon AGAZINE AUGUST/SEPTEMBER 2009 Spain of Neosho, Mo., steadies the motorcycle.