Returning to School
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Lingfield and Area Community News Edition
Spring 2018 Number 206 Spring in SE Surrey In this edition: Opposition to “garden village” plans grow News on the station crossing Do we need CCTV in Lingfield? Community News is distributed free to Lingfield, Crowhurst, Dormansland, Dormans Park, Felcourt and parts of Newchapel, Haxted, Horne, and Baldwins Hill [email protected] 316405 www.mpg-maintenance.com WINDOW AND LOCKSMITH DOOR REPAIRS PROPERTY DOUBLE GLAZING MAINTENANCE SHUTTERS BI-FOLD DOORS 2 Community News Team Contact E: mail@communitynewslingfield.co.uk A: c/o Lingfield & Dormansland Community Centre, High St, Lingfield, RH7 6AB W: www.communitynewslingfield.co.uk Editorial Manager / Chairman Edward Pearcey 07828 993 376 Editorial David Allonby 01342 832 514 Treasurer Michael Pocock 01342 832 685 Advertising Edward Pearcey 07828 993 376 Graham Marks 01342 832 529 Secretary Gillian Pocock 01342 832 685 Distribution Grace Porter 01342 833 841 Production Cox and Co Creative 01342 836 564 The next edition of Community News is the Summer publication. The deadline for submissions is 29th March 2018 Please send submissions to the email or postal address above. Community News is a non-profit making free newspaper published four times each year. The views expressed are not necessarily those of the editorial team. Donations, although always welcome, do not guarantee publication of material submitted by the donor. Please note that all material sent is forwarded at the contributor's own risk. Whilst every care is taken with material, Community News cannot be held responsible for any loss or damage incurred. The editors reserve the right to edit material (reduce the length of an article) and rewrite or otherwise modify it if they deem it necessary. -

PROPOSED PANS for 2008 for COMMUNITY And
APPENDIX 1 PROPOSED Admission numbers for Surrey County Council’s community and voluntary controlled schools 2016 This document sets out Surrey County Council’s proposed Published Admission Numbers (PAN) for community and voluntary controlled schools for September 2016. Where changes have been made text is in bold. 1. Primary schools School PAN ELMBRIDGE Bell Farm Primary 90 Claygate Primary 60 #Cranmere Primary 90 Grovelands Primary 60 #Hinchley Wood Primary 90 *Hurst Park Primary 60 Long Ditton Infant & Nursery 60 **Manby Lodge Infant 90 Oatlands 90 4+ 30 The Royal Kent C of E Primary 7+ 2 St Andrew’s Cof E Primary 4+ 52 7+ 8 St James C of E Primary 60 Thames Ditton Infant 90 Thames Ditton Junior 90 Walton Oak 60 # Agreed through statutory proposals to expand to a PAN of 90 from September 2016 * Agreed through statutory proposals to expand to a PAN of 60 from September 2015 **Agreed through statutory proposals to expand to a PAN of 90 from September 2015 EPSOM & EWELL Auriol Junior 90 Cuddington Community Primary 30 Epsom Primary 60 Ewell Grove Infant & Nursery 70 The Mead Infant 90 Meadow Primary 90 Southfield Park Primary 60 Stamford Green Primary 90 The Vale Primary 30 Wallace Fields Infant 60 Wallace Fields Junior 68 West Ewell Infant 120 GUILDFORD Ash Grange Primary 30 Guildford Grove Primary 60 Holly Lodge Primary 60 Merrow C of E (Cont) Infant 60 Onslow Infant 90 Pirbright Village Primary 60 Ripley Church of England Primary 28 St Mary’s C of E (VC) Infant 30 St Paul's Church of England Infant 30 Shalford Infant 30 Shawfield Primary -

Undergraduate Admissions by
Applications, Offers & Acceptances by UCAS Apply Centre 2019 UCAS Apply Centre School Name Postcode School Sector Applications Offers Acceptances 10002 Ysgol David Hughes LL59 5SS Maintained <3 <3 <3 10008 Redborne Upper School and Community College MK45 2NU Maintained 6 <3 <3 10011 Bedford Modern School MK41 7NT Independent 14 3 <3 10012 Bedford School MK40 2TU Independent 18 4 3 10018 Stratton Upper School, Bedfordshire SG18 8JB Maintained <3 <3 <3 10022 Queensbury Academy LU6 3BU Maintained <3 <3 <3 10024 Cedars Upper School, Bedfordshire LU7 2AE Maintained <3 <3 <3 10026 St Marylebone Church of England School W1U 5BA Maintained 10 3 3 10027 Luton VI Form College LU2 7EW Maintained 20 3 <3 10029 Abingdon School OX14 1DE Independent 25 6 5 10030 John Mason School, Abingdon OX14 1JB Maintained 4 <3 <3 10031 Our Lady's Abingdon Trustees Ltd OX14 3PS Independent 4 <3 <3 10032 Radley College OX14 2HR Independent 15 3 3 10033 St Helen & St Katharine OX14 1BE Independent 17 10 6 10034 Heathfield School, Berkshire SL5 8BQ Independent 3 <3 <3 10039 St Marys School, Ascot SL5 9JF Independent 10 <3 <3 10041 Ranelagh School RG12 9DA Maintained 8 <3 <3 10044 Edgbarrow School RG45 7HZ Maintained <3 <3 <3 10045 Wellington College, Crowthorne RG45 7PU Independent 38 14 12 10046 Didcot Sixth Form OX11 7AJ Maintained <3 <3 <3 10048 Faringdon Community College SN7 7LB Maintained 5 <3 <3 10050 Desborough College SL6 2QB Maintained <3 <3 <3 10051 Newlands Girls' School SL6 5JB Maintained <3 <3 <3 10053 Oxford Sixth Form College OX1 4HT Independent 3 <3 -

Microsoft Schools
Microsoft Schools Region Country State Company APAC Vietnam THCS THẠCH XÁ APAC Korea GoYang Global High School APAC Indonesia SMPN 12 Yogyakarta APAC Indonesia Sekolah Pelita Harapan Intertiol APAC Bangladesh Bangladesh St. Joseph School APAC Malaysia SMK. LAJAU APAC Bangladesh Dhaka National Anti-Bullying Network APAC Bangladesh Basail government primary school APAC Bangladesh Mogaltula High School APAC Nepal Bagmati BernHardt MTI School APAC Bangladesh Bangladesh Letu mondol high school APAC Bangladesh Dhaka Residential Model College APAC Thailand Sarakhampittayakhom School English Program APAC Bangladesh N/A Gabtali Govt. Girls' High School, Bogra APAC Philippines Compostela Valley Atty. Orlando S. Rimando National High School APAC Bangladesh MOHONPUR GOVT COLLEGE, MOHONPUR, RAJSHAHI APAC Indonesia SMAN 4 Muaro Jambi APAC Indonesia MA NURUL UMMAH LAMBELU APAC Bangladesh Uttar Kulaura High School APAC Malaysia Melaka SMK Ade Putra APAC Indonesia Jawa Barat Sukabumi Study Center APAC Indonesia Sekolah Insan Cendekia Madani APAC Malaysia SEKOLAH KEBANGSAAN TAMAN BUKIT INDAH APAC Bangladesh Lakhaidanga Secondary School APAC Philippines RIZAL STI Education Services Group, Inc. APAC Korea Gyeonggi-do Gwacheon High School APAC Philippines Asia Pacific College APAC Philippines Rizal Institute of Computer Studies APAC Philippines N/A Washington International School APAC Philippines La Consolacion University Philippines APAC Korea 포항제철지곡초등학교 APAC Thailand uthaiwitthayakhom school APAC Philippines Philippines Isabel National Comprehensive School APAC Philippines Metro Manila Pugad Lawin High School APAC Sri Lanka Western Province Wise International School - Sri Lanka APAC Bangladesh Faridpur Govt. Girls' High School, Faridpur 7800 APAC New Zealand N/A Cornerstone Christian School Microsoft Schools APAC Philippines St. Mary's College, Quezon City APAC Indonesia N/A SMA N 1 Blora APAC Vietnam Vinschool Thành phố Hồ Chí APAC Vietnam Minh THCS - THPT HOA SEN APAC Korea . -

Gcse Grades up Again at Local Schools
CATERHAM AUTO CataxLtd REPAIRS Est. 1946 All Mechanical & Body Repairs Caterham’s longest established taxi Servicing, MOTs company Minis a Speciality CATERHAM OFFICE Roffes Lane, Caterham Surrey CR3 5PT 01883 345151 01883 348748 www.caterhamtaxis.com No. 73 September 2012 CIRCULATION: 22,000 ESTABLISHED 2006 FREE GCSE GRADES UP AGAIN AT LOCAL SCHOOLS The GCSE results for de A*-C grades including English go into stem cell research; Stafford School, Warlingham and Maths. I find it fascinating!” Secondary School, The Oasis Lydia Gatward, Robert This year the school cele- Academy and Caterham Clark, Kayleigh Gillings and brated especially good re- School are all higher than Rachel Harper were among sults, with an 11% increase last year, despite the na- those who performed excep- in the number of students tional trend for slightly lower tionally well, achieving 14 or who gained GCSE Maths. grades this year. more GCSEs, with the ma- Caroline Longhurst, Head- The anxious wait for stu- jority being A*/A grades. teacher, commented: “Our dents ended on Thursday Lydia Gatward from Chaldon results this year show an 23rd August when the re- was thrilled to achieve 16 improvement on the per- sults were published. passes, including 3 A*s and centage of students leaving At de Stafford School in 9 As. school with 5 or more A*-C Caterham the school continued Lydia said: “I am going to go grades including English its upward trend, with 55% of on to study the Sciences at and maths which is a key students achieving five or more Reigate College. I want to indicator of a school’s per- formance.” Happy de Stafford students with their GCSE results, from Continued on pages 8-9 left, Lydia Gatward from Chaldon, Atudsa Habibian from with more GSCE good Caterham Valley, Connor Cooper from Old Coulsdon and news from other local George Gasson from Old Coulsdon. -

What Is School Direct?
What is School Direct? School Direct is a programme whereby schools recruit trainees directly and select them to train and work within their partnership schools. Schools, therefore, have more control over the quality of training, which is provided, and how it is delivered. We guarantee an interview for any relevant post in a partnership school for those who are successful on the programme with us. What are the routes? There are two routes into School Direct: Salaried and non-salaried. The salaried route is aimed at graduates with at least 3 years work experience and is an employment-based route into teaching. The non-salaried route is open to all graduates funded by bursaries and tuition fees paid by the graduate through the student loan scheme. Our School Direct programmes will lead you to gaining a PGCE in conjunction with our partnership universities. Who is in our partnership? The Warwick School (www.warwick.surrey.sch.uk) Reigate College (http://www.reigate.ac.uk/) Royal Alexandra and Albert School (http://www.raa-school.co.uk/) Oxted School (http://www.oxtedschool.co.uk) The Ashcombe School (Lead School) (http://www.ashcombe.surrey.sch.uk/index.shtml) University of Sussex (http://www.sussex.ac.uk/education) University of Brighton (http://about.brighton.ac.uk/education/) We have a very successful and long-standing tradition of working with these schools and universities and have been fortunate enough to offer permanent employment to most of our school direct trainees in the past 7 years. What kind of training can we offer you? The model for training that we will follow will primarily focus on training in the classroom as well as having regular focused training days delivered by outstanding practitioners. -
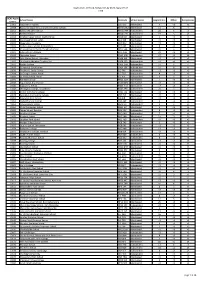
DRAFT Nearest Schools
APPENDIX 3 DRAFT Academies and foundation, trust and voluntary aided schools that will be considered in the assessment of nearest school and out of county schools that will not be considered in the assessment of nearest school - 2017/18 admissions 1. Academies and foundation, trust and voluntary aided schools in Surrey that will be considered in the assessment of nearest school when applying the admission arrangements for community and voluntary controlled schools are set out below. Community and voluntary controlled schools which convert to academy status and new free schools which open after these arrangements have been determined will be added to this list by default. a) Infant & primary schools – Reception intake Elmbridge Spelthorne (continued) Burhill Community Infant School Littleton C of E Infant School Chandlers Field Primary School Saxon Primary School Cobham Free School Springfield Primary School The Orchard School Stanwell Fields CofE Primary School St Matthew’s C of E Infant School St Nicholas C of E Primary School Epsom & Ewell Surrey Heath Cuddington Croft Primary School Bisley C of E Primary School Riverview C of E Primary School Cross Farm Infant School St Martin’s C of E Infant School The Grove Primary School Guildford Lakeside Primary School Boxgrove Primary Lightwater Village School Burpham Foundation Primary School Mytchett Primary School Chilworth C of E Infant School Sandringham School Clandon C of E Infant School St Lawrence C of E Primary School Peaslake School Tandridge Pewley Down Infant School Burstow Primary -

Youth Showcase Awards 2020
Voice Mole Valley Youth Showcase Awards 2020 Virtual Awards Event Programme #mvyouthawards Mole Valley Youth Voice Members Rebecca Cleary (Leader) Mary Nevins (Chairman) Noah Cripps (Vice Chairman) Emma Friend Daniel Evans Ruby Barrett Diana Adams-Fuller If you are interested in joining Youth Voice, we are always keen for new members, email us at [email protected] We invite you to follow our Youth Voice social media sites Twitter | Facebook | Instagram: @mvyouthvoice Mole Valley Youth Voice encourage that members of the audience share and promote the live stream of this event on their own social media accounts. We are extremely proud of all our nominees. Line Up Welcome and Introduction by Rebecca Cleary, Youth Voice Leader Music Award presented by Ethan Hodges, ‘X Factor the Band’ semi-finalist Dance Award presented by Helena Pardey-Yaralli, professional dancer of the Italia Conti Arts Centre Drama Award presented by Diana Adams-Fuller, Youth Voice Member Artist Award presented by Claudia Cartwright, Arts and Community Officer at Mole Valley District Council Sporting Achievement Award presented by Ruby Barrett, Youth Voice Member Chef Award presented by Daniel Evans, Youth Voice Member Team Award presented by Emma Friend, Youth Voice Member Volunteer Award presented by Councillor Mary Huggins, Chairman of Mole Valley District Council Outstanding Achievement Award presented by Danesh Amin, Director at Cocoa Island, Chairman of South Surrey Young Enterprise Close by Mole Valley Youth Voice Music Award For displaying musical ability in any instrument or voice. Oscar Belfrage Bordoli - The Priory School A brilliant trumpet player who has dedicated time to performances in and out of school whilst currently on-track to get his Grade 8 Trumpet qualification. -

Oxted, Surrey. a Rare Opportunity to Purchase a Well Presented 1950'S Four Bedroom Detached House on a Sought After Road in Central Oxted
Oxted, Surrey. A rare opportunity to purchase a well presented 1950's four bedroom detached house on a sought after road in central Oxted. A good sized westerly facing garden backing on to pretty woodland. Highlights include solid wooden flooring, open fireplace and attractive lead light double glazed windows. - Four double bedrooms - Two bathrooms - Two reception rooms - Central location - Driveway and garage - Large garden - Utility room - EPC C - 1991 SQF - Council Tax band G REIGATE 1-3 High Street Reigate RH2 9AA 01737 246246 [email protected] OXTED 72 Station Road East Oxted RH8 0PG 01883 717272 [email protected] LINGFIELD 27 High Street Lingfield RH7 6AA 01342 837783 [email protected] LETTINGS & MANAGEMENT Julie Sullivan 01883 717272 LAND & NEW HOMES Wendi Leech 01737 246246 EQUESTRIAN & COUNTRY Paul Dixon FCMI Assoc.RICS FNAEA FNAVA 01342 837783 DIRECTORS Robert V Leech Wendi Leech ASSOCIATE DIRECTOR Richard Goman Robert Leech Estate Agents Ltd Incorporated in England Registered No.8704789 CONTENTS 1. School standards 3. Local authority council tax 5. Your Green Guide 2. What’s nearby 4. Get to know your neighbours 6. Sounds like a plan Welcome to the Neighbourhood It’s all here. Everything you want to know about your potential new home…and more besides. We’ve brought together the latest information from reliable official sources, to answer all your questions on where you’re looking to live. Want to know about schools? You’ll find performance results for nurseries, infant, junior and secondary schools in the area. Looking for your local pub or nearest swimming pool? Details of all your local amenities are in the next few pages. -
2014 Admissions Cycle
Applications, Offers & Acceptances by UCAS Apply Centre 2014 UCAS Apply School Name Postcode School Sector Applications Offers Acceptances Centre 10002 Ysgol David Hughes LL59 5SS Maintained 4 <3 <3 10008 Redborne Upper School and Community College MK45 2NU Maintained 11 5 4 10011 Bedford Modern School MK41 7NT Independent 20 5 3 10012 Bedford School MK40 2TU Independent 19 3 <3 10018 Stratton Upper School, Bedfordshire SG18 8JB Maintained 3 <3 <3 10020 Manshead School, Luton LU1 4BB Maintained <3 <3 <3 10022 Queensbury Academy LU6 3BU Maintained <3 <3 <3 10024 Cedars Upper School, Bedfordshire LU7 2AE Maintained 4 <3 <3 10026 St Marylebone Church of England School W1U 5BA Maintained 20 6 5 10027 Luton VI Form College LU2 7EW Maintained 21 <3 <3 10029 Abingdon School OX14 1DE Independent 27 13 13 10030 John Mason School, Abingdon OX14 1JB Maintained <3 <3 <3 10031 Our Lady's Abingdon Trustees Ltd OX14 3PS Independent <3 <3 <3 10032 Radley College OX14 2HR Independent 10 4 4 10033 St Helen & St Katharine OX14 1BE Independent 14 8 8 10036 The Marist Senior School SL5 7PS Independent <3 <3 <3 10038 St Georges School, Ascot SL5 7DZ Independent 4 <3 <3 10039 St Marys School, Ascot SL5 9JF Independent 6 3 3 10041 Ranelagh School RG12 9DA Maintained 7 <3 <3 10043 Ysgol Gyfun Bro Myrddin SA32 8DN Maintained <3 <3 <3 10044 Edgbarrow School RG45 7HZ Maintained <3 <3 <3 10045 Wellington College, Crowthorne RG45 7PU Independent 20 6 6 10046 Didcot Sixth Form College OX11 7AJ Maintained <3 <3 <3 10048 Faringdon Community College SN7 7LB Maintained -

Lexie Is Crowned Caterham's New May Queen
CATERHAM AUTO CataxLtd REPAIRS Est. 1946 All Mechanical The Caterham and District &Body Repairs Caterham’s longest established taxi Servicing, MOTs company Minis a Speciality CATERHAM Roffes Lane, Caterham Surrey CR3 5PT 01883 345151 01883 348748 Delivered door to door in Caterham-on-the-Hill, Caterham Valley, Chaldon, Godstone, www.caterhamtaxis.com INDEKenleyP, NethernEe-on-the-HNill and OlDd CoulsdoEn. NT 12th ANNIVERSARY EDITION! No. 145 June 2018 ESTABLISHED 2006 FREE Lexie is crowned Cater ham’s new On Saturday 5th May, nine- The ancient tradition is yMear-old aLexyie C aQrdy uwas ebeinge kepn t alive and well in crowned this year’s Caterham Caterham by local girls who May Queen by last year’s May work their way up through Queen, ten-year-old Ruby Birch. the ranks each year to ulti - Lexie, a pupil at St. John’s mately become May Queen, CoE Primary School, enjoys where the age limit is 16. street dance, tap dance and At the crowning, Lexie was cheerleading, and loves uni - attended by her retinue - corns and mermaids! Elise Cardy (Prince); Shanay Lexie said: “I’m so happy that Creasey (Crown Bearer); Lily- I am Caterham May Queen. I May Appleby (Banner love wearing the beautiful Bearer); Alfie Appleby dress and pretty crown, and (Drummer Boy); Scarlett can’t wait to open the Cater - Arnold (Fairy) and Aaliya ham Carnival on 9th June.” Fletcher (Fairy). BOOK NOW FOR Lexie Cardy. Photo by Kelly Lexie with her retinue of attendants following the crowning. Cardy. Photo by Sonia Hunt. CHILDREN’S SUMMER HOLIDAY SWIMMING COURSES at Warlingham School, Tithepitshaw Lane, Warlingham, on: Caterham's only independent vet surgery 23rd-28th July, 20th-24th August 28th August – 1st September CATCH US AT THE STREET PARTY! For more information and to book, 17 ESSENDENE ROAD, e-mail: [email protected] CATERHAM, CR3 5PB or visit [email protected] www.aquariusswimming.co.uk vetonthehill.co.uk 01883 341306 "Helping your pets stay healthy and live their life to the full" Free Registration & consultation for all new clients at our Caterham Practice. -
Verbal Reasoning Guidelines
Contents Senior School Guidance ...................................................................................................................................................... 3 Communication .................................................................................................................................................................. 4 A Summary of the Key Events to Support Parents ............................................................................................................. 5 Choosing a Senior School .................................................................................................................................................... 6 Leavers’ Destinations 2001-2017 ....................................................................................................................................... 8 Senior Schools: Timetable for Tests/Entry 2017/18 ........................................................................................................... 9 Senior School Entrance ..................................................................................................................................................... 15 Scholarships and Awards Guidance .................................................................................................................................. 16 Scholarship Suitability and Award Criteria ....................................................................................................................... 17 Preparation for Senior