Clinical Aspects of Hyponatremia & Hypernatremia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Hyponatremia and Hypernatremia MICHAEL M
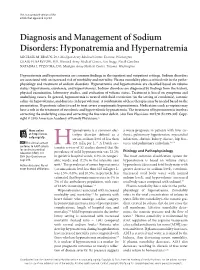
This is a corrected version of the article that appeared in print. Diagnosis and Management of Sodium Disorders: Hyponatremia and Hypernatremia MICHAEL M. BRAUN, DO, Madigan Army Medical Center, Tacoma, Washington CRAIG H. BARSTOW, MD, Womack Army Medical Center, Fort Bragg, North Carolina NATASHA J. PYZOCHA, DO, Madigan Army Medical Center, Tacoma, Washington Hyponatremia and hypernatremia are common findings in the inpatient and outpatient settings. Sodium disorders are associated with an increased risk of morbidity and mortality. Plasma osmolality plays a critical role in the patho- physiology and treatment of sodium disorders. Hyponatremia and hypernatremia are classified based on volume status (hypovolemia, euvolemia, and hypervolemia). Sodium disorders are diagnosed by findings from the history, physical examination, laboratory studies, and evaluation of volume status. Treatment is based on symptoms and underlying causes. In general, hyponatremia is treated with fluid restriction (in the setting of euvolemia), isotonic saline (in hypovolemia), and diuresis (in hypervolemia). A combination of these therapies may be needed based on the presentation. Hypertonic saline is used to treat severe symptomatic hyponatremia. Medications such as vaptans may have a role in the treatment of euvolemic and hypervolemic hyponatremia. The treatment of hypernatremia involves correcting the underlying cause and correcting the free water deficit. Am( Fam Physician. 2015;91(5):299-307. Copy- right © 2015 American Academy of Family Physicians.) More online yponatremia is a common elec- a worse prognosis in patients with liver cir- at http://www. trolyte disorder defined as a rhosis, pulmonary hypertension, myocardial aafp.org/afp. serum sodium level of less than infarction, chronic kidney disease, hip frac- CME This clinical content 135 mEq per L.1-3 A Dutch sys- tures, and pulmonary embolism.1,8-10 conforms to AAFP criteria Htematic review of 53 studies showed that the for continuing medical Etiology and Pathophysiology education (CME). -

Antibiotic Assay Medium No. 3 (Assay Broth) Is Used for Microbiological Assay of Antibiotics. M042
HiMedia Laboratories Technical Data Antibiotic Assay Medium No. 3 (Assay Broth) is used for M042 microbiological assay of antibiotics. Antibiotic Assay Medium No. 3 (Assay Broth) is used for microbiological assay of antibiotics. Composition** Ingredients Gms / Litre Peptic digest of animal tissue (Peptone) 5.000 Beef extract 1.500 Yeast extract 1.500 Dextrose 1.000 Sodium chloride 3.500 Dipotassium phosphate 3.680 Potassium dihydrogen phosphate 1.320 Final pH ( at 25°C) 7.0±0.2 **Formula adjusted, standardized to suit performance parameters Directions Suspend 17.5 grams in 1000 ml distilled water. Heat if necessary to dissolve the medium completely. Sterilize by autoclaving at 15 lbs pressure (121°C) for 15 minutes. Advice:Recommended for the Microbiological assay of Amikacin, Bacitracin, Capreomycin, Chlortetracycline,Chloramphenicol,Cycloserine,Demeclocycline,Dihydrostreptomycin, Doxycycline, Gentamicin, Gramicidin, Kanamycin, Methacycline, Neomycin, Novobiocin, Oxytetracycline, Rolitetracycline, Streptomycin, Tetracycline, Tobramycin, Trolendomycin and Tylosin according to official methods . Principle And Interpretation Antibiotic Assay Medium is used in the performance of antibiotic assays. Grove and Randall have elucidated those antibiotic assays and media in their comprehensive treatise on antibiotic assays (1). Antibiotic Assay Medium No. 3 (Assay Broth) is used in the microbiological assay of different antibiotics in pharmaceutical and food products by the turbidimetric method. Ripperre et al reported that turbidimetric methods for determining the potency of antibiotics are inherently more accurate and more precise than agar diffusion procedures (2). Turbidimetric antibiotic assay is based on the change or inhibition of growth of a test microorganims in a liquid medium containing a uniform concentration of an antibiotic. After incubation of the test organism in the working dilutions of the antibiotics, the amount of growth is determined by measuring the light transmittance using spectrophotometer. -

Antibacterial Residue Excretion Via Urine As an Indicator for Therapeutical Treatment Choice and Farm Waste Treatment
antibiotics Article Antibacterial Residue Excretion via Urine as an Indicator for Therapeutical Treatment Choice and Farm Waste Treatment María Jesús Serrano 1, Diego García-Gonzalo 1 , Eunate Abilleira 2, Janire Elorduy 2, Olga Mitjana 1 , María Victoria Falceto 1, Alicia Laborda 1, Cristina Bonastre 1 , Luis Mata 3 , Santiago Condón 1 and Rafael Pagán 1,* 1 Instituto Agroalimentario de Aragón-IA2, Universidad de Zaragoza-CITA, 50013 Zaragoza, Spain; [email protected] (M.J.S.); [email protected] (D.G.-G.); [email protected] (O.M.); [email protected] (M.V.F.); [email protected] (A.L.); [email protected] (C.B.); [email protected] (S.C.) 2 Public Health Laboratory, Office of Public Health and Addictions, Ministry of Health of the Basque Government, 48160 Derio, Spain; [email protected] (E.A.); [email protected] (J.E.) 3 Department of R&D, ZEULAB S.L., 50197 Zaragoza, Spain; [email protected] * Correspondence: [email protected]; Tel.: +34-9-7676-2675 Abstract: Many of the infectious diseases that affect livestock have bacteria as etiological agents. Thus, therapy is based on antimicrobials that leave the animal’s tissues mainly via urine, reaching the environment through slurry and waste water. Once there, antimicrobial residues may lead to antibacterial resistance as well as toxicity for plants, animals, or humans. Hence, the objective was to describe the rate of antimicrobial excretion in urine in order to select the most appropriate molecule while reducing harmful effects. Thus, 62 pigs were treated with sulfamethoxypyridazine, Citation: Serrano, M.J.; oxytetracycline, and enrofloxacin. Urine was collected through the withdrawal period and analysed García-Gonzalo, D.; Abilleira, E.; via LC-MS/MS. -

Demeclocycline
PATIENT & CAREGIVER EDUCATION Demeclocycline This information from Lexicomp® explains what you need to know about this medication, including what it’s used for, how to take it, its side effects, and when to call your healthcare provider. What is this drug used for? It is used to treat bacterial infections. It may be given to you for other reasons. Talk with the doctor. What do I need to tell my doctor BEFORE I take this drug? If you have an allergy to demeclocycline or any other part of this drug. If you are allergic to this drug; any part of this drug; or any other drugs, foods, or substances. Tell your doctor about the allergy and what signs you had. If you are taking penicillin. If you are breast-feeding or plan to breast-feed. This is not a list of all drugs or health problems that interact with this drug. Tell your doctor and pharmacist about all of your drugs Demeclocycline 1/8 (prescription or OTC, natural products, vitamins) and health problems. You must check to make sure that it is safe for you to take this drug with all of your drugs and health problems. Do not start, stop, or change the dose of any drug without checking with your doctor. What are some things I need to know or do while I take this drug? Tell all of your health care providers that you take this drug. This includes your doctors, nurses, pharmacists, and dentists. Avoid driving and doing other tasks or actions that call for you to be alert until you see how this drug affects you. -

Hyperchloremia – Why and How
Document downloaded from http://www.elsevier.es, day 23/05/2017. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. n e f r o l o g i a 2 0 1 6;3 6(4):347–353 Revista de la Sociedad Española de Nefrología www.revistanefrologia.com Brief review Hyperchloremia – Why and how Glenn T. Nagami Nephrology Section, Department of Medicine, VA Greater Los Angeles Healthcare System and David Geffen School of Medicine at UCLA, United States a r t i c l e i n f o a b s t r a c t Article history: Hyperchloremia is a common electrolyte disorder that is associated with a diverse group of Received 5 April 2016 clinical conditions. The kidney plays an important role in the regulation of chloride concen- Accepted 11 April 2016 tration through a variety of transporters that are present along the nephron. Nevertheless, Available online 3 June 2016 hyperchloremia can occur when water losses exceed sodium and chloride losses, when the capacity to handle excessive chloride is overwhelmed, or when the serum bicarbonate is low Keywords: with a concomitant rise in chloride as occurs with a normal anion gap metabolic acidosis Hyperchloremia or respiratory alkalosis. The varied nature of the underlying causes of the hyperchloremia Electrolyte disorder will, to a large extent, determine how to treat this electrolyte disturbance. Serum bicarbonate Published by Elsevier Espana,˜ S.L.U. on behalf of Sociedad Espanola˜ de Nefrologıa.´ This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/ licenses/by-nc-nd/4.0/). -

An Infant with Chronic Hypernatremia
European Journal of Endocrinology (2006) 155 S141–S144 ISSN 0804-4643 An infant with chronic hypernatremia M L Marcovecchio Department of Paediatrics, University of Chieti, Via dei Vestini 5, 66100 Chieti, Italy (Correspondence should be addressed to M L Marcovecchio; Email: [email protected]) Abstract A 4-month-old boy was presented with failure to thrive, refusal to feed, delayed motor development, truncal hypotonia, and head lag. His plasma osmolality and sodium were significantly high, while his urine osmolality was inappropriately low and did not increase after desmopressin administration. Despite his hyperosmolality, he presented with a lack of thirst and became clearly polyuric and polydipsic only at the age of 2 years. Initial treatment with indomethacin was ineffective, while the combination of hydrochlorothiazide and amiloride was effective and well tolerated. European Journal of Endocrinology 155 S141–S144 Introduction (61 ml/kg) respectively. Other investigations including thyroid and adrenal function were normal. He was Chronic hypernatremia in young patients is generally refusing oral fluids despite being hypernatremic. the result of alterations in the mechanisms controlling A cranial magnetic resonance imaging scan excluded fluid balance (1). Excessive water loss, as in diabetes structural abnormalities in the hypophysis, hypo- insipidus, or an inadequate fluid intake, as in adipsic thalamus and surrounding area. There was no response hypernatremia, may be the underlying cause. The to 0.3 mg 1-desamino-8-D-arginine-vasopressin (DDAVP) differential diagnosis between these conditions is given intravenously (osmolality pre- 374 mosmol/kg; important in order to choose the appropriate treatment. post- 371 mosmol/kg). This suggested a tubular defect However, pitfalls in the diagnosis are often related to an causing nephrogenic diabetes insipidus (NDI). -

Electrolyte and Acid-Base Disorders Triggered by Aminoglycoside Or Colistin Therapy: a Systematic Review
antibiotics Review Electrolyte and Acid-Base Disorders Triggered by Aminoglycoside or Colistin Therapy: A Systematic Review Martin Scoglio 1,* , Gabriel Bronz 1, Pietro O. Rinoldi 1,2, Pietro B. Faré 3,Céline Betti 1,2, Mario G. Bianchetti 1, Giacomo D. Simonetti 1,2, Viola Gennaro 1, Samuele Renzi 4, Sebastiano A. G. Lava 5 and Gregorio P. Milani 2,6,7 1 Faculty of Biomedicine, Università della Svizzera Italiana, 6900 Lugano, Switzerland; [email protected] (G.B.); [email protected] (P.O.R.); [email protected] (C.B.); [email protected] (M.G.B.); [email protected] (G.D.S.); [email protected] (V.G.) 2 Department of Pediatrics, Pediatric Institute of Southern Switzerland, Ospedale San Giovanni, Ente Ospedaliero Cantonale, 6500 Bellinzona, Switzerland; [email protected] 3 Department of Internal Medicine, Ospedale La Carità, Ente Ospedaliero Cantonale, 6600 Locarno, Switzerland; [email protected] 4 Division of Hematology and Oncology, The Hospital for Sick Children, Toronto, ON M5G 1X8, Canada; [email protected] 5 Pediatric Cardiology Unit, Department of Pediatrics, Centre Hospitalier Universitaire Vaudois, and University of Lausanne, 1011 Lausanne, Switzerland; [email protected] 6 Pediatric Unit, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, 20122 Milan, Italy 7 Department of Clinical Sciences and Community Health, Università degli Studi di Milano, 20122 Milan, Italy * Correspondence: [email protected] Citation: Scoglio, M.; Bronz, G.; Abstract: Aminoglycoside or colistin therapy may alter the renal tubular function without decreasing Rinoldi, P.O.; Faré, P.B.; Betti, C.; the glomerular filtration rate. This association has never been extensively investigated. -
TETRACYCLINES and CHLORAMPHENICOL Protein Synthesis
ANTIMICROBIALS INHIBITING PROTEIN SYNTHESIS AMINOGLYCOSIDES MACROLIDES TETRACYCLINES AND CHLORAMPHENICOL Protein synthesis Aminoglycosides 1. Aminoglycosides are group of natural and semi -synthetic antibiotics. They have polybasic amino groups linked glycosidically to two or more aminosugar like: sterptidine, 2-deoxy streptamine, glucosamine 2. Aminoglycosides which are derived from: Streptomyces genus are named with the suffix –mycin. While those which are derived from Micromonospora are named with the suffix –micin. Classification of Aminoglycosides 1. Systemic aminogycosides Streptomycin (Streptomyces griseus) Gentamicin (Micromonospora purpurea) Kanamycin (S. kanamyceticus) Tobramycin (S. tenebrarius) Amikacin (Semisynthetic derivative of Kanamycin) Sisomicin (Micromonospora inyoensis) Netilmicin (Semisynthetic derivative of Sisomicin) 2. Topical aminoglycosides Neomycin (S. fradiae) Framycetin (S. lavendulae) Pharmacology of Streptomycin NH H2N NH HO OH Streptidine OH NH H2N O O NH CHO L-Streptose CH3 OH O HO O HO NHCH3 N-Methyl-L- Glucosamine OH Streptomycin Biological Source It is a oldest aminoglycoside antibiotic obtained from Streptomyces griseus. Antibacterial spectrum 1. It is mostly active against gram negative bacteria like H. ducreyi, Brucella, Yersinia pestis, Francisella tularensis, Nocardia,etc. 2. It is also used against M.tuberculosis 3. Few strains of E.coli, V. cholerae, H. influenzae , Enterococci etc. are sensitive at higher concentration. Mechanism of action Aminoglycosides bind to the 16S rRNA of the 30S subunit and inhibit protein synthesis. 1. Transport of aminoglycoside through cell wall and cytoplasmic membrane. a) Diffuse across cell wall of gram negative bacteria by porin channels. b) Transport across cell membrane by carrier mediated process liked with electron transport chain 2. Binding to ribosome resulting in inhibition of protein synthesis A. -

Is There a Relationship Between COVID-19 and Hyponatremia?
medicina Review Is There a Relationship between COVID-19 and Hyponatremia? Gina Gheorghe 1,2,†, Madalina Ilie 1,2, Simona Bungau 3,† , Anca Mihaela Pantea Stoian 4 , Nicolae Bacalbasa 5 and Camelia Cristina Diaconu 6,7,* 1 Department of Gastroenterology, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania; [email protected] (G.G.); [email protected] (M.I.) 2 Department of Gastroenterology, Clinical Emergency Hospital of Bucharest, 105402 Bucharest, Romania 3 Department of Pharmacy, Faculty of Medicine and Pharmacy, University of Oradea, 410028 Oradea, Romania; [email protected] 4 Department of Diabetes, Nutrition and Metabolic Diseases, “Carol Davila” University of Medicine and Pharmacy, 020475 Bucharest, Romania; [email protected] 5 Department of Visceral Surgery, Center of Excellence in Translational Medicine, Fundeni Clinical Institute, 022328 Bucharest, Romania; [email protected] 6 Department of Internal Medicine, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania 7 Department of Internal Medicine, Clinical Emergency Hospital of Bucharest, 105402 Bucharest, Romania * Correspondence: [email protected]; Tel.: +40-0726-377-300 † This author has equal contribution to the paper as the first author. Abstract: Nowadays, humanity faces one of the most serious health crises, the severe acute respi- ratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. The severity of coronavirus disease 2019 (COVID-19) pandemic is related to the high rate of interhuman transmission of the virus, variability of clinical presentation, and the absence of specific therapeutic methods. COVID-19 can manifest with non-specific symptoms and signs, especially among the elderly. In some cases, the clinical manifestations of hyponatremia may be the first to appear. -

Demeclocycline in the Treatment of the Syndrome of Inappropriate Secretion of Antidiuretic Hormone
Thorax: first published as 10.1136/thx.34.3.324 on 1 June 1979. Downloaded from Thorax, 1979, 34, 324-327 Demeclocycline in the treatment of the syndrome of inappropriate secretion of antidiuretic hormone W H PERKS, E H WALTERS,' I P TAMS, AND K PROWSE From the Department of Respiratory Physiology, City General Hospital, Stoke-on-Trent, Staffordshire, UK ABSTRACT Fourteen patients with the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) have been treated with demethylchlortetracycline (demeclocycline) 1200 mg daily. In 12 patients the underlying lesion was malignant. The serum sodium returned to normal (> 135 mmol/l) in all patients after a mean of 8-6 days (SD+5-3 days). Blood urea rose significantly from the pretreatment level of 4-2±2-3 mmol/l to 10-1±5-1 mmol/l at ten days (p<0 001). The average maximum blood urea was 13-4-6-8 mmol/l. In four patients the urea rose above 20 mmol/l, and in two of these demecyocycline was discontinued because of this rise. The azotaemia could be attributed to a combination of increased urea production and a mild specific drug-induced nephrotoxicity. Discontinuation of demeclocycline in six patients led to a fall in serum sodium, in one case precipitously, and return of the urea towards normal levels. Demeclocycline appears therefore to be an effective maintenance treatment of SIADH, and the azotaemia that occurs is reversible and probably dose dependent. The syndrome of inappropriate secretion of anti- Methods http://thorax.bmj.com/ diuretic hormone (SIADH) has become increas- ingly recognised as a treatable cause of stupor and Fourteen patients with a diagnosis of SIADH confusion in patients with a wide variety of based on the criteria of De Troyer and Demanet diseases (De Troyer and Demanet, 1976). -

A Case of Hypocalciuric Hypercalcemia Accompanying Cystic Fibrosis
J Clin Res Pediatr Endocrinol 2015;7(Suppl 2):77-92 A Case of Hypocalciuric Hypercalcemia Accompanying Cystic Fibrosis Yaşar Şen, Sevil Arı Yuca, Fuat Buğrul Blood and urine tests were done in order to find the etiology of hypercalcemia (PTH: 65.5 pg/mL, 25-hydroxy vitamin Selçuk University Faculty of Medicine, Department of Pediatric D: 43.5 ng/mL, urine Ca/Cr ratio 0.19, urine Ca clearance Endorcinology, Konya, Turkey 0.004). In the CaSR gene mutation study, A986S and R990G polymorphisms were heterozygous. 1 month after hydration Introduction: Familial hypocalciuric hypercalcemia (FHH) and clinical state being back to normal, Ca levels were is an autosomal dominant disorder which occurs by an in normal range. In stressful situations, he experienced inactivating gene mutation in the calcium (Ca)-sensing hypernatremia and hypercalcemia together. receptor gene (CaSR). Prevalence is estimated at 1: 78000. Discussion: Polymorphisms may change protein function Ca regulates parathormone (PTH) secretion via CaSR on and capacity of one to repair its damaged DNA. Genetic parathyroid cells. Low levels of Ca increases PTH secretion. polymorphisms help us to define personal sensitivities to CaSR mutation that causes loss of function, leads to total some diseases. The most common CaSR polymorphisms or partial insensitivity of parathyroid cells to Ca’s inhibitory are A986S, R990G, Q1011E and A826T. Our patient effect. For this reason, in order to suppress Ca’s PTH had A986S and R990G mutations. Heterozygous CaSR secretory effect, the setpoint is raised. A higher blood Ca gene mutations generally cause mild disorders in clinic. level is needed to suppress the PTH secretion. -

RECEPTOR ANTAGONISTS Vasopressin V2 Receptor Antagonists
1 RECEPTOR ANTAGONISTS Vasopressin V2 receptor antagonists J G Verbalis 232 Building D, Division of Endocrinology and Metabolism, Georgetown University School of Medicine, 4000 Reservoir Road NW, Washington DC 20007, USA (Requests for offprints should be addressed toJGVerbalis; Email: [email protected]) Abstract Hyponatremia, whether due to the syndrome of inappropriate antidiuretic hormone secretion (SIADH) or disorders of water retention such as congestive heart failure and cirrhosis, is a very common problem encountered in the care of medical patients. To date, available treatment modalities for disorders of excess arginine vasopressin (AVP) secretion or action have been limited and suboptimal. The recent discovery and development of nonpeptide AVP V2 receptor antagonists represents a promising new treatment option to directly antagonize the effects of elevated plasma AVP concentrations at the level of the renal collecting ducts. By decreasing the water permeability of renal collecting tubules, excretion of retained water is promoted, thereby normalizing or improving hypo-osmolar hyponatremia. In this review, SIADH and other water retaining disorders are briefly discussed, after which the published preclinical and clinical studies of several nonpeptide AVP V2 receptor antagonists are summarized. The likely therapeutic indications and potential complications of these compounds are also described. Journal of Molecular Endocrinology (2002) 29, 1–9 Introduction heart failure (CHF) and cirrhosis with ascites. In these disorders, a relatively decreased intravascular Arginine vasopressin (AVP), the ‘antidiuretic volume and/or pressure leads to water retention as a hormone,’ is the major physiological regulator of result of both decreased distal delivery of glomerular renal free water excretion. Increased AVP secretion filtrate and secondarily elevated plasma AVP levels.