Serum Sodium Concentration [Na+] Less Than 135 Meq/L. INCIDENCE
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Hyponatremia and Hypernatremia MICHAEL M
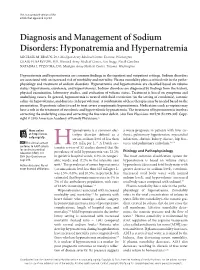
This is a corrected version of the article that appeared in print. Diagnosis and Management of Sodium Disorders: Hyponatremia and Hypernatremia MICHAEL M. BRAUN, DO, Madigan Army Medical Center, Tacoma, Washington CRAIG H. BARSTOW, MD, Womack Army Medical Center, Fort Bragg, North Carolina NATASHA J. PYZOCHA, DO, Madigan Army Medical Center, Tacoma, Washington Hyponatremia and hypernatremia are common findings in the inpatient and outpatient settings. Sodium disorders are associated with an increased risk of morbidity and mortality. Plasma osmolality plays a critical role in the patho- physiology and treatment of sodium disorders. Hyponatremia and hypernatremia are classified based on volume status (hypovolemia, euvolemia, and hypervolemia). Sodium disorders are diagnosed by findings from the history, physical examination, laboratory studies, and evaluation of volume status. Treatment is based on symptoms and underlying causes. In general, hyponatremia is treated with fluid restriction (in the setting of euvolemia), isotonic saline (in hypovolemia), and diuresis (in hypervolemia). A combination of these therapies may be needed based on the presentation. Hypertonic saline is used to treat severe symptomatic hyponatremia. Medications such as vaptans may have a role in the treatment of euvolemic and hypervolemic hyponatremia. The treatment of hypernatremia involves correcting the underlying cause and correcting the free water deficit. Am( Fam Physician. 2015;91(5):299-307. Copy- right © 2015 American Academy of Family Physicians.) More online yponatremia is a common elec- a worse prognosis in patients with liver cir- at http://www. trolyte disorder defined as a rhosis, pulmonary hypertension, myocardial aafp.org/afp. serum sodium level of less than infarction, chronic kidney disease, hip frac- CME This clinical content 135 mEq per L.1-3 A Dutch sys- tures, and pulmonary embolism.1,8-10 conforms to AAFP criteria Htematic review of 53 studies showed that the for continuing medical Etiology and Pathophysiology education (CME). -

Electrolyte and Acid-Base Disorders Triggered by Aminoglycoside Or Colistin Therapy: a Systematic Review
antibiotics Review Electrolyte and Acid-Base Disorders Triggered by Aminoglycoside or Colistin Therapy: A Systematic Review Martin Scoglio 1,* , Gabriel Bronz 1, Pietro O. Rinoldi 1,2, Pietro B. Faré 3,Céline Betti 1,2, Mario G. Bianchetti 1, Giacomo D. Simonetti 1,2, Viola Gennaro 1, Samuele Renzi 4, Sebastiano A. G. Lava 5 and Gregorio P. Milani 2,6,7 1 Faculty of Biomedicine, Università della Svizzera Italiana, 6900 Lugano, Switzerland; [email protected] (G.B.); [email protected] (P.O.R.); [email protected] (C.B.); [email protected] (M.G.B.); [email protected] (G.D.S.); [email protected] (V.G.) 2 Department of Pediatrics, Pediatric Institute of Southern Switzerland, Ospedale San Giovanni, Ente Ospedaliero Cantonale, 6500 Bellinzona, Switzerland; [email protected] 3 Department of Internal Medicine, Ospedale La Carità, Ente Ospedaliero Cantonale, 6600 Locarno, Switzerland; [email protected] 4 Division of Hematology and Oncology, The Hospital for Sick Children, Toronto, ON M5G 1X8, Canada; [email protected] 5 Pediatric Cardiology Unit, Department of Pediatrics, Centre Hospitalier Universitaire Vaudois, and University of Lausanne, 1011 Lausanne, Switzerland; [email protected] 6 Pediatric Unit, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, 20122 Milan, Italy 7 Department of Clinical Sciences and Community Health, Università degli Studi di Milano, 20122 Milan, Italy * Correspondence: [email protected] Citation: Scoglio, M.; Bronz, G.; Abstract: Aminoglycoside or colistin therapy may alter the renal tubular function without decreasing Rinoldi, P.O.; Faré, P.B.; Betti, C.; the glomerular filtration rate. This association has never been extensively investigated. -

Is There a Relationship Between COVID-19 and Hyponatremia?
medicina Review Is There a Relationship between COVID-19 and Hyponatremia? Gina Gheorghe 1,2,†, Madalina Ilie 1,2, Simona Bungau 3,† , Anca Mihaela Pantea Stoian 4 , Nicolae Bacalbasa 5 and Camelia Cristina Diaconu 6,7,* 1 Department of Gastroenterology, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania; [email protected] (G.G.); [email protected] (M.I.) 2 Department of Gastroenterology, Clinical Emergency Hospital of Bucharest, 105402 Bucharest, Romania 3 Department of Pharmacy, Faculty of Medicine and Pharmacy, University of Oradea, 410028 Oradea, Romania; [email protected] 4 Department of Diabetes, Nutrition and Metabolic Diseases, “Carol Davila” University of Medicine and Pharmacy, 020475 Bucharest, Romania; [email protected] 5 Department of Visceral Surgery, Center of Excellence in Translational Medicine, Fundeni Clinical Institute, 022328 Bucharest, Romania; [email protected] 6 Department of Internal Medicine, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania 7 Department of Internal Medicine, Clinical Emergency Hospital of Bucharest, 105402 Bucharest, Romania * Correspondence: [email protected]; Tel.: +40-0726-377-300 † This author has equal contribution to the paper as the first author. Abstract: Nowadays, humanity faces one of the most serious health crises, the severe acute respi- ratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. The severity of coronavirus disease 2019 (COVID-19) pandemic is related to the high rate of interhuman transmission of the virus, variability of clinical presentation, and the absence of specific therapeutic methods. COVID-19 can manifest with non-specific symptoms and signs, especially among the elderly. In some cases, the clinical manifestations of hyponatremia may be the first to appear. -

The Prognostic Effects of Hyponatremia and Hyperchloremia on Postoperative NSCLC Patients
Current Problems in Cancer 43 (2019) 402–410 Contents lists available at ScienceDirect Current Problems in Cancer journal homepage: www.elsevier.com/locate/cpcancer The prognostic effects of hyponatremia and hyperchloremia on postoperative NSCLC patients Wei Li a,b,1, Xiaowei Chen a,1, Liguang Wang a,c, Yu Wang a, ∗ Cuicui Huang a, Guanghui Wang a,d, Jiajun Du a,d, a Institute of Oncology, Shandong Provincial Hospital Affiliated to Shandong University, Jinan, PR China b Department of Thoracic Surgery, Shandong Juxian People’s Hospital, Rizhao, PR China c Department of Oncology, Shandong Provincial Hospital Affiliated to Shandong University, Jinan, PR China d Department of Thoracic Surgery, Shandong Provincial Hospital Affiliated to Shandong University, Jinan, PR China a b s t r a c t Electrolytic disorders are common in lung cancer patients. But the association between serum electrolytes levels and survival in patients undergoing lung cancer resections for non–small-cell lung cancer (NSCLC) has been poorly inves- tigated. A retrospective study was conducted on consecutive postoperative NSCLC patients. Pearson’s test was used to determine the association between serum sodium and chlorine levels and clinical characteristics, and cox regression and Kaplan-Meier model were applied to analyze risk factors on overall survival. We found that hyponatremia was an independent prognostic factor associated with poor prognosis in NSCLC patients undergoing complete resection (log-rank test, P = 0.004). In addition, we found that hyperchloremia predicted a poor clinical outcome in patients with non-anion-gap (log-rank test, P = 0.011), whereas it predicted a favorable clinical outcome in patients with high- anion-gap (log-rank test, P = 0.002). -
Hypercalcemia and Hyponatremia
Hypercalcemia and Hyponatremia Santosh Reddy MD FACP Assistant Professor Scott & White/Texas A&M Etiology of Hypercalcemia Hypercalcemia results when the entry of calcium into the circulation exceeds the excretion of calcium into the urine or deposition in bone. Sources of calcium are most commonly the bone or the gastrointestinal tract Etiology Hypercalcemia is a relatively common clinical problem. Elevation in the physiologically important ionized (or free) calcium concentration. However, 40 to 45 percent of the calcium in serum is bound to protein, principally albumin; , increased protein binding causes elevation in the serum total calcium. Increased bone resorption Primary and secondary hyperparathyroidism Malignancy Hyperthyroidism Other - Paget's disease, estrogens or antiestrogens in metastatic breast cancer, hypervitaminosis A, retinoic acid Increased intestinal calcium absorption Increased calcium intake Renal failure (often with vitamin D supplementation) Milk-alkali syndrome Hypervitaminosis D Enhanced intake of vitamin D or metabolites Chronic granulomatous diseases (eg, sarcoidosis) Malignant lymphoma Acromegaly Pseudocalcemia Hyperalbuminemia 1) severe dehydration 2) multiple myeloma who have a calcium- binding paraprotein. This phenomenon is called pseudohypercalcemia (or factitious hypercalcemia) Other causes Familial hypocalciuric hypercalcemia Chronic lithium intake Thiazide diuretics Pheochromocytoma Adrenal insufficiency Rhabdomyolysis and acute renal failure Theophylline toxicity Immobilization -

Neurologic Complications of Electrolyte Disturbances and Acid–Base Balance
Handbook of Clinical Neurology, Vol. 119 (3rd series) Neurologic Aspects of Systemic Disease Part I Jose Biller and Jose M. Ferro, Editors © 2014 Elsevier B.V. All rights reserved Chapter 23 Neurologic complications of electrolyte disturbances and acid–base balance ALBERTO J. ESPAY* James J. and Joan A. Gardner Center for Parkinson’s Disease and Movement Disorders, Department of Neurology, UC Neuroscience Institute, University of Cincinnati, Cincinnati, OH, USA INTRODUCTION hyperglycemia or mannitol intake, when plasma osmolal- ity is high (hypertonic) due to the presence of either of The complex interplay between respiratory and renal these osmotically active substances (Weisberg, 1989; function is at the center of the electrolytic and acid-based Lippi and Aloe, 2010). True or hypotonic hyponatremia environment in which the central and peripheral nervous is always due to a relative excess of water compared to systems function. Neurological manifestations are sodium, and can occur in the setting of hypovolemia, accompaniments of all electrolytic and acid–base distur- euvolemia, and hypervolemia (Table 23.2), invariably bances once certain thresholds are reached (Riggs, reflecting an abnormal relationship between water and 2002). This chapter reviews the major changes resulting sodium, whereby the former is retained at a rate faster alterations in the plasma concentration of sodium, from than the latter (Milionis et al., 2002). Homeostatic mech- potassium, calcium, magnesium, and phosphorus as well anisms protecting against changes in volume and sodium as from acidemia and alkalemia (Table 23.1). concentration include sympathetic activity, the renin– angiotensin–aldosterone system, which cause resorption HYPONATREMIA of sodium by the kidneys, and the hypothalamic arginine vasopressin, also known as antidiuretic hormone (ADH), History and terminology which prompts resorption of water (Eiskjaer et al., 1991). -

Disorders of Sodium and Water Balance
Disorders of Sodium and Water Balance Theresa R. Harring, MD*, Nathan S. Deal, MD, Dick C. Kuo, MD* KEYWORDS Dysnatremia Water balance Hyponatremia Hypernatremia Fluids for resuscitation KEY POINTS Correct hypovolemia before correcting sodium imbalance by giving patients boluses of isotonic intravenous fluids; reassess serum sodium after volume status normalized. Serum and urine electrolytes and osmolalities in patients with dysnatremias in conjunction with clinical volume assessment are especially helpful to guide management. If an unstable patient is hyponatremic, give 2 mL/kg of 3% normal saline (NS) up to 100 mL over 10 minutes; this may be repeated once if the patient continues to be unstable. If unstable hypernatremic patient, give NS with goal to decrease serum sodium by 8 to 15 mEq/L over 8 hours. Correct stable dysnatremias no faster than 8 mEq/L to 12 mEq/L over the first 24 hours. INTRODUCTION Irregularities of sodium and water balance most often occur simultaneously and are some of the most common electrolyte abnormalities encountered by emergency med- icine physicians. Approximately 10% of all patients admitted from the emergency department suffer from hyponatremia and 2% suffer from hypernatremia.1 Because of the close nature of sodium and water balance, and the relatively rigid limits placed on the central nervous system by the skull, it is not surprising that most symptoms related to disorders of sodium and water imbalance are neurologic and can, therefore, be devastating. Several important concepts are crucial to the understanding of these disorders, the least of which include body fluid compartments, regulation of osmo- lality, and the need for rapid identification and appropriate management. -

Evaluating and Managing Electrolyte Disbalances in the Outpatient Setting Disclosure
EVALUATING AND MANAGING ELECTROLYTE DISBALANCES IN THE OUTPATIENT SETTING DISCLOSURE There are no conflicts of interest Homeostasis • Potassium • Water Evaluation and Management of Electrolyte TO BE DISCUSSED Disbalances • Hyperkalemia • Hypokalemia • Hypernatremia • Hyponatremia Summary DISORDERS OF POTASSIUM BALANCE: HYPERKALEMIA AND HYPOKALEMIA POTASSIUM HOMEOSTASIS • Aldosterone • High Na+ delivery to distal tubule Increase (diuretics) Renal K+ • High urine flow (osmotic diuresis) Excretion • High serum K+ level • Delivery bicarbonate to distal tubule • Absence, or very low aldosterone • Low Na+ delivery to the distal Decrease tubule Renal K+ • Low urine flow Excretion • Low serum K+ level • Kidney Injury MORTALITY IN DYSKALEMIA Collins et al Am J Nephrol 2017;46:213- 221 HYPERKALEMIA MY PATIENT HAS HYPERKALEMIA, WHAT SHOULD I DO? H&P and Check other medication causes •Changes? Treat review •Send home •Symptoms? Treat •Metabolic acidosis •Obstruction •Hyperosmolarity •K+ increasing meds •CKD Pseudohyperkale EKG and BMP mia CAUSES OF HYPERKALEMIA Increased potassium release from Reduced urinary potassium excretion cells • Pseudohyperkalemia • Acute and chronic kidney disease • Fist clenching • Reduced aldosterone secretion or • Tourniquet use response to aldosterone • Metabolic acidosis • Reduced distal sodium and water • Insulin deficiency, hyperglycemia, delivery and hyperosmolality • Drugs • Increased tissue catabolism • Drugs • Hyperkalemic Periodic Palasysis Biff Palmer A Physiologic-Based Approach to the Evaluation of a Patient -

Fluid & Electrolyte Disorders
FLUID & ELECTROLYTE DISORDERS 11/2/18 Don Beckstead M.D. 63WYCH Disclosures • I have nothing to disclose • This talk is intended to cover adult electrolyte issues 2 63WYCH GOALS AND OBJECTIVES • Identify causes of common electrolyte abnormalities found in primary care office patients. • Discuss signs and symptoms found in patients who have common electrolyte abnormalities. • Become comfortable with treatment modalities that can be used to correct common electrolyte abnormalities. 3 63WYCH 1 ELECTROLYTES • We will cover: –High and low sodium –High and low potassium –High and low calcium –High and low magnesium 4 63WYCH SOME BASIC PRINCIPLES • Kidneys prioritize fluid and electrolyte balance at the possible expense of acid‐base balance. • Normally functioning kidneys have a great capacity to handle increased or decreased intake of most electrolytes. • Most electrolyte abnormalities found are in asymptomatic patients. • Sodium abnormalities are usually actually water abnormalities 5 Text 63WYCH to 828-216-8114 BASIC METABOLIC PROFILE . Sodium (Na+ ) 136‐150 . Chloride (Cl‐) 100‐110 . Bicarbonate (CO2) 22‐28 . Potassium (K+) 3.6‐5.0 . BUN (blood urea nitrogen) 5‐18 . Creatinine 0.6 ‐ 1.3 . Anion Gap (Na+‐ {Cl‐ + CO2}) = ~ 12 . Calcium (Ca++) 8.5 – 10.3 . Magnesium (Mg++) 1.5 ‐ 2.3 6 2 SODIUM 7 63WYCH HYPONATREMIA CAUSES • Suppressed ADH – CKD – Polydipsia • Increased ADH – CHF – Cirrhosis – Thiazide diuretics – SIADH – Pregnancy/hypothyroidism/adrenal insufficiency 8 63WYCH HYPONATREMIA w/ HIGH/NL OSMO • Hyperlipidemia • Hyperproteinemia • Mannitol administration • Hyperglycemia • CRF (BUN ineffective osmol) 9 63WYCH 3 HYPONATREMIA SYMPTOMS • Usually none • If not pseudohyponatremia (+ low osmolality), then symptoms are usually related to development of cerebral edema – Nausea/vomiting – Malaise/lethargy – Headache – Seizures/coma/respiratory arrest 10 63WYCH HYPONATREMIA WORK‐UP • Urine osmol. -

The Hypercalcemia of Adrenal Insufficiency
THE HYPERCALCEMIA OF ADRENAL INSUFFICIENCY Mackenzie Walser, … , Brian H. B. Robinson, John W. Duckett Jr. J Clin Invest. 1963;42(4):456-465. https://doi.org/10.1172/JCI104734. Research Article Find the latest version: https://jci.me/104734/pdf Journal of Clinical Investigation Vol. 42, No. 4, 1963 THE HYPERCALCEMIA OF ADRENAL INSUFFICIENCY * By MACKENZIE WALSER, BRIAN H. B. ROBINSON,t AND JOHN W. DUCKETT, JR.t (From the Department of Pharinacology and Experimental Therapeutics and the Departmnent of Medicine, The Johns Hopkins University School of Medicine and The Johns Hopkins Hospital, Baltimore, Md.) (Submitted for publication October 3, 1962; accepted December 6, 1962) An interrelationship between the adrenal glands cium in this condition appear to have been re- and calcium metabolism was demonstrated in 1911 ported. Increased parathyroid gland activity dur- by Guleke (1), who showed that adrenalectomy ing adrenal insufficiency was suggested by the re- ameliorates tetany in parathyroidectomized ani- ported finding of parathyroid hyperplasia in mals. This observation has been repeatedly con- adrenalectomized animals (23). Against this firmed (2). view is the occurrence of hypercalcemia in adre- Hypercalcemia after adrenalectomy was first nalectomized parathyroidectomized dogs (22), as demonstrated in 1924 by Kisch (3) in rabbits, and well as the antagonistic effects of cortisone and soon thereafter by other workers in dogs (4-8), parathyroid extract mentioned above. cats (5, 9), and in patients with Addison's disease Adrenal steroids block the excessive intestinal (10-12). An early report (13) of hypercalcemia absorption of calcium in sarcoidosis (24) and tend in adrenalectomized rats was based upon dubious to inhibit the active transport of calcium by the methods of analysis; later reports indicate that isolated gut (25). -

Cerebral Salt Wasting Syndrome: Review ⁎ M
European Journal of Internal Medicine 19 (2008) 249–254 www.elsevier.com/locate/ejim Review article Cerebral salt wasting syndrome: Review ⁎ M. Cerdà-Esteve a, , E. Cuadrado-Godia b, J.J. Chillaron a, C. Pont-Sunyer b, G. Cucurella b, M. Fernández a, A. Goday a, J.F. Cano-Pérez a, A. Rodríguez-Campello b, J. Roquer b a Endocrinology Department, Hospital Universitari del Mar, Universitat Autònoma de Barcelona, Barcelona, Spain b Neurology Department, Hospital Universitari del Mar, Universitat Autònoma de Barcelona, Barcelona, Spain Received 24 January 2007; received in revised form 4 June 2007; accepted 29 June 2007 Available online 7 March 2008 Abstract Hyponatremia is the most frequent electrolyte disorder in critically neurological patients. Cerebral salt wasting syndrome (CSW) is defined as a renal loss of sodium during intracranial disease leading to hyponatremia and a decrease in extracellular fluid volume. The pathogenesis of this disorder is still not completely understood. Sympathetic responses as well as some natriuretic factors play a role in this syndrome. Distinction between SIADH and CSW might be difficult. The essential point is the volemic state. It is necessary to rule out other intermediate causes. Treatment requires volume replacement and maintenance of a positive salt balance. Mineral corticoids may be useful in complicated cases. © 2008 European Federation of Internal Medicine. Published by Elsevier B.V. All rights reserved. Keywords: Cerebral; Salt; Wasting; Hyponatremia; Inappropriate ADH syndrome 1. Introduction 2. Epidemiology Cerebral salt wasting syndrome (CSW) is defined as a Hyponatremia is the most common electrolyte finding in renal loss of sodium during intracranial disorders leading to hospitalized patients; its frequency; however, depends on hyponatremia and a decrease in extracellular fluid volume. -

Metabolic Alkalosis with Multiple Salt Unbalance: an Atypical Onset of Cystic Fibrosis in a Child
www.jpnim.com Open Access eISSN: 2281-0692 Journal of Pediatric and Neonatal Individualized Medicine 2018;7(1):e070105 doi: 10.7363/070105 Received: 2017 Aug 25; revised: 2017 Sept 18; accepted: 2017 Oct 18; published online: 2017 Dec 01 Case report Metabolic alkalosis with multiple salt unbalance: an atypical onset of cystic fibrosis in a child Dimitri Poddighe1,2, Lucia Castelli1, Elena Virginia Comi1, Ilaria Brambilla2, Paola Bruni1 1Department of Pediatrics, ASST Melegnano e Martesana, Vizzolo Predabissi (MI), Italy 2Department of Pediatrics, Università degli Studi di Pavia, Pavia, Italy Abstract Dehydration with multiple salt abnormalities is frequently encountered in the paediatric emergency department, during acute illnesses complicated by loss of body fluids. Metabolic alkalosis is not a common finding in dehydrated children. The presence of unusual electrolyte unbalance, such as metabolic alkalosis, hyponatremia, hypochloremia and hypokalemia, without evidence of renal tubular defects, is named as pseudo-Bartter syndrome. It can occur in several clinical settings and, in infancy, it is described as a potential complication of cystic fibrosis. We report a case of pseudo-Bartter syndrome representing the onset of cystic fibrosis in childhood. Keywords Pseudo-Bartter syndrome, metabolic alkalosis, hyponatremia, cystic fibrosis, child. Corresponding author Dr. Dimitri Poddighe, M.D., Department of Pediatrics, Azienda Ospedaliera di Melegnano, via Pandina 1, 20070 Vizzolo Predabissi (MI), Italy; phone: 0039-347-7241851; email: [email protected]. How to cite Poddighe D, Castelli L, Comi EV, Brambilla I, Bruni P. Metabolic alkalosis with multiple salt unbalance: an atypical onset of cystic fibrosis in a child. J Pediatr Neonat Individual Med. 2018;7(1):e070105.