Download PDF Annual Performance Report 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
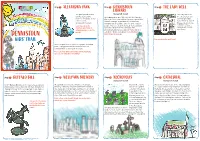
DENNISTOUN Stop 3 the LADY WELL LIBRARY the Park Opened in 1870 (Category B-Listed) the Lady Well Is on and Was Named After the Library Opened in 1905
Stop 1 ALEXANDRA PARK Stop 2 DENNISTOUN Stop 3 THE LADY WELL LIBRARY The park opened in 1870 (Category B-listed) The Lady Well is on and was named after The Library opened in 1905. It is called a Carnegie the site of an ancient Princess Alexandra. At the Library because it was built using money donated by well that provided entrance is the Andrew Carnegie, a man born in Scotland who water for the people of Cruikshank Fountain. moved to America and became one of the richest Glasgow before it was common to have Look closely at the people who ever lived. He donated money to build running water inside fountain, what kind of over 2000 libraries across the world. The your home. animal do you see on the Dennistoun Library has a special statue which is inside? called the “Dennistoun Angel”. Can you find it? DENNISTOUN Don’t forget to look up! KIDS’ TRAIL Can you draw the well here? Inside the park there is lots to see and do, including ponds, a playground and the beautiful Saracen Fountain which is over 12 metres tall! There are four different statues on the fountain, can you see what they’re holding? Stop 4 BUFFALO BILL Stop 5 WELLPARK BREWERY Stop 6 NECROPOLIS Stop 7 CATHEDRAL (Category A-listed) (Category A-listed) In 1891 Buffalo Bill, One of the most famous and well Wellpark Brewery was first known as the Drygate Glasgow Necropolis Glasgow Cathedral is one of the oldest buildings known figures of the American Old West, brought his Brewery, a brewery is a place where beer is made.It was the first garden in Glasgow and the only mediaeval cathedral in “Wild West Show” to the very spot where his statue is was founded in 1740 by Hugh and Robert Tennent but cemetery in Scotland. -
Gilmorehill Campus Development Framework
80 University Brand & Visual issue 1.0 University Brand & Visual issue 1.0 81 of Glasgow Identity Guidelines of Glasgow Identity Guidelines Our lockup (where and how our marque appears) Our primary lockups Our lockup should be used primarily on Background We have two primary lockups, in line with our primary colour front covers, posters and adverts but not Use the University colour palette, and follow palette. We should always use one of these on core publications, within the inside of any document. the colour palette guidelines, to choose the such as: appropriate lockup for your purpose. For For consistency across our material, and · Annual Review example, if the document is for a specific to ensure our branding is clear and instantly · University’s Strategic Plan college, that college’s colour lockup recognisable, we have created our lockup. · Graduation day brochure. is probably the best one to use. If the This is made up of: document is more general, you may want Background to use a lockup from the primary palette. Our marque/Sub-identity Use a solid background colour – or a 70% Help and advice for compiling our transparent background against full bleed approved lockups are available images (see examples on page 84). from Corporate Communications at Our marque [email protected]. Our marque always sits to the left of the lockup on its own or as part of a sub- identity. 200% x U 200% x U Gilmorehill 200% x U Campus Lockup background. Can be solid or used at 70% transparency Development Framework < > contents | print | close -

Yorkhill 0/1, 30 Nairn Street, Glasgow G3 8SF
Yorkhill 0/1, 30 Nairn Street, Glasgow G3 8SF Ground Floor Flat Yorkhill Offers Over £99,995 Offered to the market in good decorative order, this ideal starter flat occupies a ground floor position within a red sandstone tenement building which is located within walking distance of Glasgow's flourishing West End, Glasgow University and indeed public transport links to Glasgow City Centre and beyond. Internally the accommodation is well laid out and comprises entrance hallway with stripped timber flooring and high level meters, bay windowed lounge with dining recess, double glazed windows, stripped flooring, focal point timber fire place with tiled backing and hearth and shelved storage alcove. The compact galley kitchen offers floor and wall mounted units, has front facing window, integrated oven, hob, hood, washing machine and fridge freezer to be included in the sale price, overhead downlighters and timber flooring. The double bedroom faces the rear of the property and has twin double glazed rear facing windows, storage cupboard housing the Vokera combination boiler for the central heating system and fitted carpet. The bathroom is internal with three piece white suite comprising low level wc, wash-hand basin and panelled bath with Triton mains shower above and tiling around the bath area. Further features include gas central heating, double glazing, security entry system operating the front communal access door, private and enclosed front gardens and enclosed rear gardens where the bin stores and located. Early viewing is strongly recommended as property within this particular area rarely graces the market and indeed tends to sell quickly. The West End of Glasgow is home to the main campus of the University of Glasgow and several major teaching hospitals. -

North West Sector Profile
Appendix North West Sector Profile Contents 1. Introduction Page 1 2. Executive Summary Page 2 3. Demographic & Socio – Economic Page 8 4. Labour Market/Employment/Education Page 13 5. Health Page 23 6. Neighbourhood Management Page 29 1. Introduction 1.1 The profile provides comparative information on the North West Sector Community Planning Partnership (CPP) area, including demographic & socio economic, employment, health and neighbourhood management information. 1.2 North West Glasgow is diverse in socio economic terms, as illustrated by the map, as it contains Glasgow’s city centre/ business area, the more affluent west end of Glasgow but also localities with significant issues relating to employment, health and poverty. The North West is the academic centre of the City with the three Glasgow Universities located in the sector and also has many cultural & historical buildings of interest as well as large areas of green space. Table 1: North West Sector Summary Population (2011 Census) 206,483 (up 7.1%) Population (2011 Census) exc. communal establishments 197,419 Working Age Population 16-64 (2011 Census) 151,345 (73.3%) Electorate (2014) 165,009 Occupied Households (2011 Census) 101,884 (up 9.5%) Average Household Size (2011) exc. communal establishments 1.94 (2.07 in 2011) Housing Stock (2014) 105,638 No. of Dwellings per Hectare (2012) 22.28 Out Of Work Benefit Claimants (May 2014) 24,230 (16.0%) Job Seekers Allowance (February 2015) 5,141 (3.4%) 2. Executive Summary Demographic Information 2.1 Population According to the 2011 Census, The North West sector population was 206,483. The population in the North West Sector increased by 13,773 (7.1%) from 2001 Census. -

Life Expectancy Trends Within Glasgow, 2001-2009
Glasgow: health in a changing city a descriptive study of changes in health, demography, housing, socioeconomic circumstances and environmental factors in Glasgow over the last 20 years Bruce Whyte March 2016 Contents Acknowledgements 3 Abbreviations/glossary 3 Executive summary 7 1. Introduction 9 2. Background 10 3. Aims and methods 14 4. An overview of changes in demography, housing, socioeconomic circumstances and environmental factors in Glasgow 17 5. Changes in life expectancy in Glasgow 38 6. Discussion 52 7. Policy implications 57 8. Conclusions 61 Appendices 62 References 65 2 Acknowledgements I would like to thank Craig Waugh and Lauren Schofield (both of ISD Scotland) who helped produce the GCPH’s local health profiles for Glasgow. Much of the data shown or referred to in this report has been drawn from the profiles. Thank you also to Ruairidh Nixon who summarised trends in key health and social indicators in an internal GCPH report; some of that work is incorporated in this report. I would also like to thank Alan MacGregor (DRS, Glasgow City Council), who provided data on housing tenure, completions and demolitions. I am grateful to my colleagues at the GPCH who have commented on this work as it has developed, in particular, Carol Tannahill, David Walsh, Sara Dodds, Lorna Kelly and Joe Crossland. I would also like to thank Jan Freeke (DRS, Glasgow City Council) who commented on drafts of the report. Members of the GCPH Management Board have also provided useful advice and comments at various stages in the analysis. 3 Abbreviations/glossary Organisations DRS Development and Regeneration Services. -

Glasgow City Health and Social Care Partnership Health Contacts
Glasgow City Health and Social Care Partnership Health Contacts January 2017 Contents Glasgow City Community Health and Care Centre page 1 North East Locality 2 North West Locality 3 South Locality 4 Adult Protection 5 Child Protection 5 Emergency and Out-of-Hours care 5 Addictions 6 Asylum Seekers 9 Breast Screening 9 Breastfeeding 9 Carers 10 Children and Families 12 Continence Services 15 Dental and Oral Health 16 Dementia 18 Diabetes 19 Dietetics 20 Domestic Abuse 21 Employability 22 Equality 23 Health Improvement 23 Health Centres 25 Hospitals 29 Housing and Homelessness 33 Learning Disabilities 36 Maternity - Family Nurse Partnership 38 Mental Health 39 Psychotherapy 47 NHS Greater Glasgow and Clyde Psychological Trauma Service 47 Money Advice 49 Nursing 50 Older People 52 Occupational Therapy 52 Physiotherapy 53 Podiatry 54 Rehabilitation Services 54 Respiratory Team 55 Sexual Health 56 Rape and Sexual Assault 56 Stop Smoking 57 Volunteering 57 Young People 58 Public Partnership Forum 60 Comments and Complaints 61 Glasgow City Community Health & Care Partnership Glasgow Health and Social Care Partnership (GCHSCP), Commonwealth House, 32 Albion St, Glasgow G1 1LH. Tel: 0141 287 0499 The Management Team Chief Officer David Williams Chief Officer Finances and Resources Sharon Wearing Chief Officer Planning & Strategy & Chief Social Work Officer Susanne Miller Chief Officer Operations Alex MacKenzie Clincial Director Dr Richard Groden Nurse Director Mari Brannigan Lead Associate Medical Director (Mental Health Services) Dr Michael Smith -

Cashback for Communities
CashBack for Communities Glasgow Local Authority 2015/16 About CashBack for Communities CashBack for Communities is a Scottish Government programme which takes funds recovered from the proceeds of crime and invests them into free activities and programmes for young people across Scotland. Inspiring Scotland is the delivery partner for the CashBack for Communities programme, appointed in July 2012. CashBack invests monies seized from criminals under the Proceeds of Crime Act 2002 back into our communities. Since 2008 the Scottish Government has committed £92 million to CashBack / community initiatives, funding community activities and facilities largely, but not exclusively, for young people. CashBack supports all 32 Local Authorities across Scotland. Sporting and recreational activities / culture / mentoring and employability / community projects. CashBack has delivered nearly 2 million activities and opportunities for young people. Phase 3 of CashBack runs to end March 2017 and is focused on positive outcomes for young people. CashBack for Communities: Aims CashBack activities: . Use the proceeds of crime in a positive way to expand young people’s horizons and increase their opportunities to develop their interests and skills in an enjoyable, fulfilling and supportive way. Are open, where possible, to all children and young people, while focusing resources in those communities suffering most from antisocial behaviour and crime. Seek to increase levels of participation to help divert young people away from ‘at risk’ behaviour, and will aim to increase the positive long-term outcomes for those who take part. Current CashBack Investment . Creative Scotland . YouthLink Scotland . Basketball Scotland . Celtic FC Foundation . Scottish Football Association . Youth Scotland . Scottish Rugby Union . -

Glasgow City Council
Item 6 16th April 2019 Glasgow Community Planning Partnership Hillhead Area Partnership Report by Executive Director of Neighbourhoods and Sustainability. Contact: Stevie Scott Ext: 0141 287 8292 Glasgow Food Growing Strategy Purpose of Report: To provide committee with: 1. feedback from the Hillhead and Anderston/City/Yorkhill wards stakeholder engagement event held in relation to development of a Food Growing Strategy for Glasgow and 2. advise of next stages. Recommendations: It is recommended that committee note this report and considers further opportunities for food growing in the Hillhead Area Partnership area. 1. Introduction 1.1 A report was brought to the Environment, Sustainability and Carbon Reduction City Policy Committee on 12th June, 2018, advising of: Progress on Glasgow’s Allotment Strategy and its links with the statutory duty, under the Community Empowerment (Scotland) Act 2015 to undertake a Food Growing Strategy (FGS) for the city The details of what a FGS for Glasgow should contain The FGS linkages to broader City strategic objectives Previous stakeholder engagement events undertaken in relation to the FGS and plans for future events 1.2 The report summarised the key actions that would be taken forward in the immediate two years as: holding a series of community consultations focussing on specific area partnerships to ascertain existing and potential growing sites; aligning the sites identified to the Glasgow Open Space Strategy process; developing an online or publicly accessible map outlining potential growing sites; carrying out an Equality Impact Assessment; developing options and funding bids in support of any actions recommended to increase the provision by Glasgow City Council of allotments, or other areas of land for use by a community for the cultivation of vegetables, fruit, herbs or flowers within the life of the Strategy; and signpost communities to resources which may support them in bringing forward their own food growing proposals. -
Flat 0/1, 76 Partickhill R O a D Partickhill, Glas G O W G 1 1 5 N B
Flat 0/1, 76 Partickhill r o a d Partickhill www.rettie.co.uk Flat 0/1, 76 Partickhill r o a d Partickhill, Glas G o w G 1 1 5 N B introduction Forming part of a really attractive modern development of stylish and innovative design which blends well with neighbouring properties this ground floor flat has some really distinct and rarely available west End features: Double doors to outside space (south facing) Private parking the development has a gradual front pathway up to the communal entrance and a side residents’ driveway which leads round to the private residents’ car park. the master bedroom has double doors leading to the private outside space and there is a further south facing grassed area (for residents) beyond. internally the flat has a well presented layout and a few of the many notable features include wooden flooring in the hall and the lounge/dining room, an excellent fitted kitchen (with door to hall, large sliding door to lounge/dining room and granite worktops) and there is an attractive en suite shower room off the master bedroom (in addition to the main bathroom off the hall). Flat 0/1, 76 Partickhill r o a d Partickhill, Glas G o w G 1 1 5 N B accommodation security entry system, communal entrance, reception hall with wooden flooring, 2 generous hall storage cupboards (one having the boiler), large main lounge/dining room to the front with wooden flooring, double windows to the front, double doors from the hall and a substantial sliding door to the kitchen, modern fitted kitchen with side window, built-in appliances and granite worktops, bedroom 1 to the rear with built-in wardrobes and double doors to the back garden, en suite shower room with window to the side, bedroom 2 to the rear with built-in wardrobes, bathroom with shower over the bath. -

Victoria Park Management Plan 2012 - 2017
Victoria Park Management Plan 2012 - 2017 LAND & ENVIRONMENTAL SERVICES VICTORIA PARK DRAFT MANAGEMENT PLAN 2012 - 2017 Victoria Park Vision To ensure that Victoria Park provides high quality facilities freely available that meet the recreational; leisure, educational and environmental needs of the community whilst protecting historical aspects and landscape character of the park. Victoria Park Management Plan 2012 - 2017 VICTORIA PARK MANAGEMENT PLAN TABLE OF CONTENTS Section 1 INTRODUCTION 3 1.1 Introduction to Victoria Park 3 1.2 Summary Information 4 1.3 Glasgow’s Parks and Open Spaces 5 1.4 Strategic Policy Framework 5 1.5 Management Plan Framework 6 1.6 Purpose of the Management Plan 6 1.7 Green Flag Award Scheme 7 Section 2 WHERE ARE WE NOW 8 2.1 History 8 2.2 The Locality 8 2.3 Map of Facilities 10 2.4 A Welcoming Place 11 2.5 Healthy Safe and Secure 14 2.6 Well Maintained and Clean 17 2.7 Sustainability 21 2.8 Conservation and Heritage 25 2.9 Community Involvement 30 2.10 Marketing 35 2.11 Management 37 Section 3 WHERE DO WE WANT TO GET TO 41 3.1 Glasgow City Council Key Objectives 41 3.2 Land and Environmental Services Mission Statement 41 3.3 Vision for Victoria Park 41 3.4 Assessment 41 Section 4 HOW WILL WE GET THERE 43 4.1 Overview 43 4.2 A Welcoming Place 44 4.3 Healthy Safe and Secure 46 4.4 Well Maintained and Clean 47 4.5 Sustainability 50 4.6 Conservation and Heritage 52 4.7 Community Involvement 55 4.8 Marketing 56 4.9 Management 57 Section 5 HOW WILL WE KNOW WHEN WE HAVE ARRIVED 59 5.1 Introduction 60 5.2 Management Plan Monitoring 60 5.3 Budget and Service Plan 60 5.4 Land and Environmental Services Annual Performance Report 60 5.5 Survey and Customer Feedback 60 5.6 Parks Development Programme Monitoring 61 1 Victoria Park Management Plan 2012 - 2017 VICTORIA PARK MANAGEMENT PLAN Section 6 APPENDICES 62 6.1 Strategic Policy Framework Details. -

South East Glasgow Community Health and Care Partnership Health Improvement Plan 2006/07 Draft
SOUTH EAST GLASGOW COMMUNITY HEALTH AND CARE PARTNERSHIP HEALTH IMPROVEMENT PLAN 2006/07 DRAFT DRAFT 1 FOREWORD Alan Stewart Chair, South East Community Health & Care Partnership (CHCP) This Plan sets out a programme for change and action to improve health and reduce the ‘inequalities gap’ of the people of South East Glasgow. Change in the way health and social care services are delivered and accessed and action that breaks the cycle of deprivation and helps build local communities where no one is held back by disadvantage. Delivering this agenda will require new ways of thinking to support and encourage people to take greater control for their own health and new ways of working that will win the support and commitment of our staff and the people we serve. Anticipating need, improving local access and shifting the balance of care from institutions with less reliance on hospital based and accommodated care to care closer to home will require greater collaboration and involvement from all partners. It is our intention to actively encourage service users, carers and the people of South East Glasgow to participate in local service planning, service modernisation and service delivery. We will also seek to secure involvement from all staff groups and key organisations. Targeting resources locally on the most vulnerable and those with greatest need to tackle lifestyle issues and those factors that are often considered outside the health domain will also be a key objective for us. These factors or determinants include: housing, education, employment status and living in a community where people feel safe from crime and anti social behaviour. -

Food Growing Strategy 2020 - 2025 DRAFT Information Contact Department
LET’S GROW TOGETHER Glasgow Food Growing Strategy 2020 - 2025 DRAFT information contact department... Contents Introduction 1.0 Our Vision • Achieving Our Vision • Strategic Context • National Strategies and policies • Local strategies and policies 2.0 Community Growing Options • Allotments • Community Gardens • Backcourts (and private gardens) • Stalled Spaces • School Grounds (or educational establishments in general) • Social Enterprises • Hospital Grounds • Housing Associations 3.0 What you said – Community Consultation 2015 to 2019 4.0 Increasing space for community growing and allotments • Allotment Sites • Community growing groups and spaces 5.0 How do I get started? • Finding land for growing • Getting permission to use a growing site • Who owns the land and do I need a lease? • Dealing with planning requirements • Getting community support or developing community group • Access to funding • Access to growing advice 6.0 How do I find out about community growing in my area? 7.0 Key Growing Themes / Opportunities Going Forward 8.0 Monitoring and Review 9.0 Next Steps / Action Plan 10.0 Appendices Appendix 1 – Food Growing Strategy Legislation Appendix 2 – Key Policies and Strategies Appendix 3 – Community Growing Matrix Appendix 4a – Food Growing Strategy Consultations Appendix 4b – Food Growing Strategy Appendix 4c – Allotments Consultation Appendix 5 – Help and Resources • Access to Land • Access to Community Support ■ Who can help you get your growing project off the ground ■ How do I set up my group • Access to funding • Funding Advice ■ Funding Guide • Access to Growing Advice ■ I want to grow fruit and vegetables – who can help me? ■ Lets Grow Glasgow Growing Guide Appendix 6 - Thanks Glasgow Food Growing Strategy 2020DRAFT Introduction I am delighted to introduce .....