TCL1A Expression Delineates Biological and Clinical Variability in B-Cell Lymphoma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Leukaemia Section
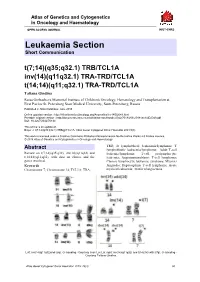
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL INIST-CNRS Leukaemia Section Short Communication t(7;14)(q35;q32.1) TRB/TCL1A inv(14)(q11q32.1) TRA-TRD/TCL1A t(14;14)(q11;q32.1) TRA-TRD/TCL1A Tatiana Gindina Raisa Gorbacheva Memorial Institute of Children's Oncology, Hematology and Transplantation at First Pavlov St. Petersburg State Medical University, Saint-Petersburg, Russia Published in Atlas Database: June 2018 Online updated version : http://AtlasGeneticsOncology.org/Anomalies/inv14ID2049.html Printable original version : http://documents.irevues.inist.fr/bitstream/handle/2042/70184/06-2018-inv14ID2049.pdf DOI: 10.4267/2042/70184 This article is an update of : Boyer J. t(7;14)(q35;q32.1) TRB@/TCL1A. Atlas Genet Cytogenet Oncol Haematol 2001;5(3) This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2019 Atlas of Genetics and Cytogenetics in Oncology and Haematology TRD; B lymphoblastic leukaemia/lymphoma; T Abstract lymphoblastic leukaemia/lymphoma; Adult T-cell Review on t(7;14)(q35;q32), inv(14)(q11q32) and leukemia/lymphoma; T-cell prolymphocytic t(14;14)(q11;q32), with data on clinics, and the leukemia; Angioimmunoblastic T-cell lymphoma; genes involved. Chronic lymphocytic leukemia; syndrome; Mycosis Keywords fungoides; Hepatosplenic T-cell lymphoma; Acute Chromosome 7; Chromosome 14; TCL1A; TRA; myeloid leukaemia; Ataxia telangiectasia. Left: inv(14)(q11q32)and i(8q), G- banding - Courtesy Jean Luc Lai; right: inv(14)(q11q32) and t(14)(14) with i(7q), G- banding - Courtesy Tatiana Gindina. Atlas Genet Cytogenet Oncol Haematol. 2019; 23(4) 90 t(7;14)(q35;q32.1) TRB/TCL1A Gindina T inv(14)(q11q32.1) TRA-TRD/TCL1A t(14;14)(q11;q32.1) TRA-TRD/TCL1A Cytogenetics Clinics and pathology Chromosomal abnormalities are detected in most T- Disease PLL after culture with mitogens like PHA. -

Biological Pathways, Candidate Genes, and Molecular Markers Associated with Quality-Of-Life Domains: an Update
Qual Life Res (2014) 23:1997–2013 DOI 10.1007/s11136-014-0656-1 REVIEW Biological pathways, candidate genes, and molecular markers associated with quality-of-life domains: an update Mirjam A. G. Sprangers • Melissa S. Y. Thong • Meike Bartels • Andrea Barsevick • Juan Ordon˜ana • Qiuling Shi • Xin Shelley Wang • Pa˚l Klepstad • Eddy A. Wierenga • Jasvinder A. Singh • Jeff A. Sloan Accepted: 19 February 2014 / Published online: 7 March 2014 Ó Springer International Publishing Switzerland 2014 Abstract (depressed mood) and positive (well-being/happiness) Background There is compelling evidence of a genetic emotional functioning, social functioning, and overall foundation of patient-reported quality of life (QOL). Given QOL. the rapid development of substantial scientific advances in Methods We followed a purposeful search algorithm of this area of research, the current paper updates and extends existing literature to capture empirical papers investigating reviews published in 2010. the relationship between biological pathways and molecu- Objectives The objective was to provide an updated lar markers and the identified QOL domains. overview of the biological pathways, candidate genes, and Results Multiple major pathways are involved in each molecular markers involved in fatigue, pain, negative QOL domain. The inflammatory pathway has the strongest evidence as a controlling mechanism underlying fatigue. Inflammation and neurotransmission are key processes On behalf of the GeneQol Consortium. involved in pain perception, and the catechol-O-methyl- transferase (COMT) gene is associated with multiple sorts Electronic supplementary material The online version of this article (doi:10.1007/s11136-014-0656-1) contains supplementary of pain. The neurotransmitter and neuroplasticity theories material, which is available to authorized users. -

Goat Anti-TCL1A Antibody Peptide-Affinity Purified Goat Antibody Catalog # Af2075a
10320 Camino Santa Fe, Suite G San Diego, CA 92121 Tel: 858.875.1900 Fax: 858.622.0609 Goat Anti-TCL1A Antibody Peptide-affinity purified goat antibody Catalog # AF2075a Specification Goat Anti-TCL1A Antibody - Product Information Application WB Primary Accession P56279 Other Accession NP_068801, 8115 Reactivity Human Host Goat Clonality Polyclonal Concentration 100ug/200ul Isotype IgG Calculated MW 13460 Goat Anti-TCL1A Antibody - Additional Information AF2075a (0.1 µg/ml) staining of Jurkat Cell Gene ID 8115 lysate (35 µg protein in RIPA buffer). Primary incubation was 1 hour. Detected by Other Names chemiluminescence. T-cell leukemia/lymphoma protein 1A, Oncogene TCL-1, Oncogene TCL1, Protein p14 TCL1, TCL1A, TCL1 Goat Anti-TCL1A Antibody - Background Format Overexpression of the TCL1 gene in humans 0.5 mg IgG/ml in Tris saline (20mM Tris has been implicated in the development of pH7.3, 150mM NaCl), 0.02% sodium azide, mature T cell leukemia, in which chromosomal with 0.5% bovine serum albumin rearrangements bring the TCL1 gene in close proximity to the T-cell antigen receptor Storage (TCR)-alpha (MIM 186880) or TCR-beta (MIM Maintain refrigerated at 2-8°C for up to 6 186930) regulatory elements (summarized by months. For long term storage store at -20°C in small aliquots to prevent Virgilio et al., 1998 [PubMed 9520462]). In freeze-thaw cycles. normal T cells TCL1 is expressed in CD4-/CD8- cells, but not in cells at later stages of Precautions differentiation. TCL1 functions as a coactivator Goat Anti-TCL1A Antibody is for research of the cell survival kinase AKT (MIM 164730) use only and not for use in diagnostic or (Laine et al., 2000 [PubMed 10983986]). -
Highly Dampened Blood Transcriptome Response in HIV Patients After Respiratory Infection Subhashini A
www.nature.com/scientificreports OPEN Highly dampened blood transcriptome response in HIV patients after respiratory infection Subhashini A. Sellers1, William A. Fischer II1, Mark T. Heise2,3,4 & Klaus Schughart 5,6,7* Respiratory viral (RV) infections represent a major threat for human health worldwide. Persons with HIV (PWH) have a compromised immune response and are thought to be at higher risk for severe RV disease. However, very little is known about the host immune response to RV infection in PWH. Here, we investigated gene expression changes in the peripheral blood of PWH co-infected with RV. Only very few diferentially expressed genes could be detected between PWH with and without RV infection, suggesting that the immune response to RV in PWH is strongly dampened. Our data provides important insights into the host response to RV infections in HIV patients. Respiratory viral (RV) infections, including infuenza and presently SARS-CoV-2 pose major threats to pub- lic health as they are responsible for epidemics and pandemics resulting in high morbidity and mortality worldwide1,2. Te most severe infuenza human pandemic in 1918 resulted in about 30 million fatal casualties 3 and the current coronavirus pandemic has already resulted in over 700,000 deaths (WHO situation report 2020). Seasonal RV infections also represent a major health hazard causing morbidity, mortality, and enormous loss of the work force yearly1,4,5. Very little is known about the immune response in persons with HIV (PWH) afer RV infection. Symptoms of RV infection appear to be similar in PWH and non-HIV patients 6. -

The Human Gene Connectome As a Map of Short Cuts for Morbid Allele Discovery
The human gene connectome as a map of short cuts for morbid allele discovery Yuval Itana,1, Shen-Ying Zhanga,b, Guillaume Vogta,b, Avinash Abhyankara, Melina Hermana, Patrick Nitschkec, Dror Friedd, Lluis Quintana-Murcie, Laurent Abela,b, and Jean-Laurent Casanovaa,b,f aSt. Giles Laboratory of Human Genetics of Infectious Diseases, Rockefeller Branch, The Rockefeller University, New York, NY 10065; bLaboratory of Human Genetics of Infectious Diseases, Necker Branch, Paris Descartes University, Institut National de la Santé et de la Recherche Médicale U980, Necker Medical School, 75015 Paris, France; cPlateforme Bioinformatique, Université Paris Descartes, 75116 Paris, France; dDepartment of Computer Science, Ben-Gurion University of the Negev, Beer-Sheva 84105, Israel; eUnit of Human Evolutionary Genetics, Centre National de la Recherche Scientifique, Unité de Recherche Associée 3012, Institut Pasteur, F-75015 Paris, France; and fPediatric Immunology-Hematology Unit, Necker Hospital for Sick Children, 75015 Paris, France Edited* by Bruce Beutler, University of Texas Southwestern Medical Center, Dallas, TX, and approved February 15, 2013 (received for review October 19, 2012) High-throughput genomic data reveal thousands of gene variants to detect a single mutated gene, with the other polymorphic genes per patient, and it is often difficult to determine which of these being of less interest. This goes some way to explaining why, variants underlies disease in a given individual. However, at the despite the abundance of NGS data, the discovery of disease- population level, there may be some degree of phenotypic homo- causing alleles from such data remains somewhat limited. geneity, with alterations of specific physiological pathways under- We developed the human gene connectome (HGC) to over- come this problem. -

Assessing the Gene Regulatory Landscape in 1,188 Human Tumors
bioRxiv preprint doi: https://doi.org/10.1101/225441; this version posted November 29, 2017. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Assessing the Gene Regulatory Landscape in 1,188 Human Tumors 1,*,$ 2,3,4,*,$ 1,5,*,$ 7,$ 5 1 2,3 Calabrese C , Lehmann K , Urban L , Liu F , Erkek S , Fonseca NA , Kahles A , 10,11 6 5 5 7 Kilpinen H , Markowski J , PCAWG Group 3, Waszak SM , Korbel JO , Zhang Z , Brazma 1,# 2,3,4,8,9,# 1,6,# 1,5,# A , Rätsch G , Schwarz RF , Stegle O * These authors contributed equally and are listed in alphabetical order. $ First authors. # Last authors in alphabetical order. 1 European Molecular Biology Laboratory, European Bioinformatics Institute, Hinxton, UK 2 Department of Computer Science, ETH Zürich, Switzerland 3 Memorial Sloan Kettering Cancer Center, New York, USA 4 University Hospital Zurich, Switzerland 5 European Molecular Biology Laboratory, Heidelberg, Germany 6 Berlin Institute for Medical Systems Biology, -

TCL1A, a Novel Transcription Factor and a Co-Regulator of NF-Кb P65: SNP and Estrogen- Dependence
JPET manuscript # 247718 TCL1A, a novel transcription factor and a co-regulator of NF-кB p65: SNP and estrogen- dependence Ming-Fen Ho, Ph.D., Edroaldo Lummertz da Rocha, Ph.D., Cheng Zhang, Ph.D., James N. Ingle, M.D., Paul E. Goss, M.D., Ph.D., Lois E. Shepherd, M.D., Michiaki Kubo, M.D., Ph.D., Liewei Wang, M.D., Ph.D., Hu Li, Ph.D., and Richard M. Weinshilboum, M.D. Division of Clinical Pharmacology, Department of Molecular Pharmacology and Experimental Therapeutics, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USA (MH, ELR, CZ, LW, HL and RW). Division of Hematology/Oncology, Department of Medicine, Massachusetts General Hospital Cancer Center, 55 Fruit Street, Lawrence House, LRH-302, Boston, Massachusetts 02114, USA (PG). Canadian Cancer Trials Group, 10 Stuart Street, Kingston, Ontario K7L 3N6 Canada (LS). Division of Medical Oncology, Department of Oncology, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USA (JI). RIKEN Center for Integrative Medical Science, 1-7-22 Suehiro-cho, Tsurumi-ku, Yokohama, 230-0045 Japan (MK). 1 JPET manuscript # 247718 Running title: TCL1A, a transcription factor and co-regulator of NF-кB p65 Corresponding author: Richard Weinshilboum, M.D., Mayo Clinic 200 First Street SW, Rochester, MN 55905, Phone: 507-284-2790, FAX: 507-284-4455, Email: [email protected] Number of text pages: 23 Number of tables: 0 (+4 Supplementary Tables) Number of figures: 8 (+5 Supplementary Figures) References: 27 Abstract, 196/250 words Introduction: 457/750 words Discussion: 1265/1500 words -

Pharmacoinformatics and Preclinical Studies of NSC765690 and NSC765599, Potential STAT3/CDK2/4/6 Inhibitors with Antitumor Activ
biomedicines Article Pharmacoinformatics and Preclinical Studies of NSC765690 and NSC765599, Potential STAT3/CDK2/4/6 Inhibitors with Antitumor Activities against NCI60 Human Tumor Cell Lines Bashir Lawal 1,2,† , Yen-Lin Liu 3,4,5,6,† , Ntlotlang Mokgautsi 1,2 , Harshita Khedkar 1,2, Maryam Rachmawati Sumitra 1,2, Alexander T. H. Wu 6,7,8,9,* and Hsu-Shan Huang 1,2,9,10,11,* 1 PhD Program for Cancer Molecular Biology and Drug Discovery, College of Medical Science and Technology, Taipei Medical University and Academia Sinica, Taipei 11031, Taiwan; [email protected] (B.L.); [email protected] (N.M.); [email protected] (H.K.); [email protected] (M.R.S.) 2 Graduate Institute for Cancer Biology and Drug Discovery, College of Medical Science and Technology, Taipei Medical University, Taipei 11031, Taiwan 3 Department of Pediatrics, Taipei Medical University Hospital, Taipei 11031, Taiwan; [email protected] 4 Taipei Cancer Center, Taipei Medical University, Taipei 11031, Taiwan 5 Department of Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei 11031, Taiwan 6 TMU Research Center of Cancer Translational Medicine, Taipei Medical University, Taipei 11031, Taiwan 7 The PhD Program of Translational Medicine, College of Science and Technology, Taipei Medical University, Taipei 11031, Taiwan 8 Clinical Research Center, Taipei Medical University Hospital, Taipei Medical University, Taipei 11031, Taiwan 9 Graduate Institute of Medical Sciences, National Defense Medical Center, Taipei 11490, Taiwan 10 School of Pharmacy, National Defense Medical Center, Taipei 11490, Taiwan 11 PhD Program in Biotechnology Research and Development, College of Pharmacy, Taipei Medical University, Citation: Lawal, B.; Liu, Y.-L.; Taipei 11031, Taiwan Mokgautsi, N.; Khedkar, H.; Sumitra, * Correspondence: [email protected] (A.T.H.W.); [email protected] (H.-S.H.) M.R.; Wu, A.T.H.; Huang, H.-S. -

Microrna Modulation of Aldosterone Production in the Adrenal Gland Nur
Ab Razak, Nur Izah (2016) MicroRNA modulation of aldosterone production in the adrenal gland. PhD thesis. https://theses.gla.ac.uk/7719/ Copyright and moral rights for this work are retained by the author A copy can be downloaded for personal non-commercial research or study, without prior permission or charge This work cannot be reproduced or quoted extensively from without first obtaining permission in writing from the author The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given Enlighten: Theses https://theses.gla.ac.uk/ [email protected] MicroRNA modulation of aldosterone production in the adrenal gland Nur Izah Ab Razak (MBBS Malaya) Thesis submitted for the degree of Doctor of Philosophy to the University of Glasgow Institute of Cardiovascular and Medical Sciences College of Medical, Veterinary and Life Sciences University of Glasgow April 2016 © Nur Izah Ab Razak 2016 1 Abstract Hypertension is the major risk factor for coronary disease worldwide. Primary hypertension is idiopathic in origin but is thought to arise from multiple risk factors including genetic, lifestyle and environmental influences. Secondary hypertension has a more definite aetiology; its major single cause is primary aldosteronism (PA), the greatest proportion of which is caused by aldosterone- producing adenoma (APA), where aldosterone is synthesized at high levels by an adenoma of the adrenal gland. There is strong evidence to show that high aldosterone levels cause adverse effects on cardiovascular, cerebrovascular, renal and other systems. -

Monoclonal Antibody(Clone: TCL1/2747R)
9853 Pacific Heights Blvd. Suite D. San Diego, CA 92121, USA Tel: 858-263-4982 Email: [email protected] 36-3410: Anti-TCL1 (T-Cell Marker) Monoclonal Antibody(Clone: TCL1/2747R) Clonality : Monoclonal Clone Name : TCL1/2747R Application : IHC Reactivity : Human Gene : TCL1A Gene ID : 10232 Uniprot ID : P56279 TCL1A; Lymphoma/leukemia, T-cell; Oncogene TCL1; P14 TCL1; T cell leukemia 1; T cell Alternative Name : lymphoma 1; T cell lymphoma 1A;T-cell leukemia/lymphoma 1A; TCL1; TCL1A Isotype : Rabbit IgG Immunogen Information : Recombinant human TCL1 protein fragment (around aa 2-109) (exact sequence is proprietary) Description T-cell leukemia/Lymphoma Protein 1A (TCL-1A), also known as p14TCL1 is a product of the TCL1 gene that is involved in T-cell prolymphocytic leukemia (TPLL). T-PLL is a rare form of mature T-cell leukemia, which is consistently associated with chromosomal rearrangements characterized by the juxtaposition of the TCRA locus on chromosome 14q11 and the TCL1A gene on 14q32.13. TCL1 is overexpressed in Burkitt lymphoma, the majority of AIDS-related non-Hodgkin lymphoma- designated immunoblastic plasmacytoid lymphoma, lymphoblastic lymphoma, chronic lymphocytic leukemia, mantle cell lymphoma, follicular lymphoma, diffuse large B-cell lymphoma, and primary cutaneous B-cell lymphoma. Product Info Amount : 20 µg / 100 µg 200 µg/ml of Ab Purified from Bioreactor Concentrate by Protein A/G. Prepared in 10mM PBS with Content : 0.05% BSA & 0.05% azide. Also available WITHOUT BSA & azide at 1.0mg/ml. Antibody with azide - store at 2 to 8°C. Antibody without azide - store at -20 to -80°C. -

Table S1. 103 Ferroptosis-Related Genes Retrieved from the Genecards
Table S1. 103 ferroptosis-related genes retrieved from the GeneCards. Gene Symbol Description Category GPX4 Glutathione Peroxidase 4 Protein Coding AIFM2 Apoptosis Inducing Factor Mitochondria Associated 2 Protein Coding TP53 Tumor Protein P53 Protein Coding ACSL4 Acyl-CoA Synthetase Long Chain Family Member 4 Protein Coding SLC7A11 Solute Carrier Family 7 Member 11 Protein Coding VDAC2 Voltage Dependent Anion Channel 2 Protein Coding VDAC3 Voltage Dependent Anion Channel 3 Protein Coding ATG5 Autophagy Related 5 Protein Coding ATG7 Autophagy Related 7 Protein Coding NCOA4 Nuclear Receptor Coactivator 4 Protein Coding HMOX1 Heme Oxygenase 1 Protein Coding SLC3A2 Solute Carrier Family 3 Member 2 Protein Coding ALOX15 Arachidonate 15-Lipoxygenase Protein Coding BECN1 Beclin 1 Protein Coding PRKAA1 Protein Kinase AMP-Activated Catalytic Subunit Alpha 1 Protein Coding SAT1 Spermidine/Spermine N1-Acetyltransferase 1 Protein Coding NF2 Neurofibromin 2 Protein Coding YAP1 Yes1 Associated Transcriptional Regulator Protein Coding FTH1 Ferritin Heavy Chain 1 Protein Coding TF Transferrin Protein Coding TFRC Transferrin Receptor Protein Coding FTL Ferritin Light Chain Protein Coding CYBB Cytochrome B-245 Beta Chain Protein Coding GSS Glutathione Synthetase Protein Coding CP Ceruloplasmin Protein Coding PRNP Prion Protein Protein Coding SLC11A2 Solute Carrier Family 11 Member 2 Protein Coding SLC40A1 Solute Carrier Family 40 Member 1 Protein Coding STEAP3 STEAP3 Metalloreductase Protein Coding ACSL1 Acyl-CoA Synthetase Long Chain Family Member 1 Protein -

Monoclonal Antibody to TCL1A / TCL1
AM26558BT-N OriGene Technologies Inc. OriGene EU Acris Antibodies GmbH 9620 Medical Center Drive, Ste 200 Schillerstr. 5 Rockville, MD 20850 32052 Herford UNITED STATES GERMANY Phone: +1-888-267-4436 Phone: +49-5221-34606-0 Fax: +1-301-340-8606 Fax: +49-5221-34606-11 [email protected] [email protected] Monoclonal Antibody to TCL1A / TCL1 - Biotin Alternate names: T-cell leukemia/lymphoma protein 1A, TCL-1 Catalog No.: AM26558BT-N Quantity: 0.1 ml Concentration: 0.5 mg/ml Background: TCL1 (T cell leukemia/lymphoma 1), MTCP1 (mature T cell proliferation 1) and TCL1b belong to the TCL1 proto-oncogene family. The TCL1 gene at chromosome 14q32.1 is co mmonly activated in T cell neoplasms by chromosome r earrangements such as inversions inv(14)(q11;q32) and translocations t(14;14)(q11;q32) or t(7;14)(q35;q32). TCL1 expression is limited to immature thymocytes in early T-cell progenitors and from pre-B to mature B cells in the B-cell lineage. The TCL1/MTCP1/TCL1b proto-oncogene activation is the hallmark of human T-cell prolymphocytic leukemia (T-PLL), a form of adult leukemia. In addition to T- PLL, TCL1 is overexpressed in Burkitt's lymphoma cell lines, the majority of AIDS-related non-Hodgkin’s lymphoma-designated immunoblastic lymphoma plasmacytoids, lymphoblastic lymphoma, chronic lymphocytic leukemia, mantle cell lymphoma, follicular lymphoma, diffuse large B-cell lymphoma, and primary cutaneous B-cell lymphoma. It is also implicated in the development of hematopoietic abnormalities in patients with ataxia- telangiectasia. The members of the TCL1 proto-oncogene family bind to the serine/threonine kinase Akt (PKB), increasing its phosphorylation status and kinase activity.