Dengue 2001 FP
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

L'education Prioritaire + Le Réseau De Papara
L’Education Prioritaire + Le Réseau de Papara Circonscription de Paea-Papara-Teva I Uta Août 2015 à juin 2018 Références : 1 -Loi du 8 juillet 2013 pour la refondation de l’école Circulaire n° 2014-077 du 4-6-2014 - Refondation de l'éducation prioritaire – BO n°23 du 05-06-2014 -Arrêté N°349 du CM, du 23 mars 2015 qui statue sur la création des trois REP+ de la Polynésie Française. -Notes d’informations de mai et du 1er juin 2015, du ministère de l’éducation et de l’enseignement supérieur de la Polynésie Française. Préambule : Ce projet de réseau est en lien avec le référentiel de l’éducation prioritaire national et les préconisations du ministère de la Polynésie Française. Il s’articule autour des axes suivants : Présentation et structure du réseau Indicateurs du réseau et diagnostiques Priorité et actions du réseau Annexes (fiches-actions et canevas de concertations, d’auto-évaluation, de compte-rendu et de bilan d’étape) Pendant les quatre années du projet de réseau, une auto-évaluation annuelle sera menée afin de réactualiser le projet en fonction des évolutions observées. Les modifications apportées pourront faire l’objet d’annexes complémentaires au document initial. 2 Table des matières 1. L’EDUCATION PRIORITAIRE, UNE CULTURE NOUVELLE SUR PAPARA 1.1. UN RESEAU PARTIEL 5 1.2. UN RESEAU JEUNE 1.3. CEC DU RESEAU 2. LES INDICATEURS DE CONTEXTE ET DE CLIMAT 2.1. LA COMPOSITION DU RESEAU 7 2.2. LES CLASSES ET EFFECTIFS DES ECOLES. 7 2.3. LES DIVISIONS ET EFFECTIFS DU COLLEGE 8 2.4. -

Répartition De La Population En Polynésie Française En 2017
Répartition de la population en Polynésie française en 2017 PIRAE ARUE Paopao Teavaro Hatiheu PAPEETE Papetoai A r c h MAHINA i p e l d FAA'A HITIAA O TE RA e s NUKU HIVA M a UA HUKA r q PUNAAUIA u HIVA OA i TAIARAPU-EST UA POU s Taiohae Taipivai e PAEA TA HUATA s NUKU HIVA Haapiti Afareaitu FATU HIVA Atuona PAPARA TEVA I UTA MOO REA TAIARAPU-OUEST A r c h i p e l d Puamau TAHITI e s T MANIHI u a HIVA OA Hipu RA NGIROA m Iripau TA KAROA PUKA P UKA o NA PUKA Hakahau Faaaha t u Tapuamu d e l a S o c i é MAKEMO FANGATA U - p e l t é h i BORA BORA G c a Haamene r MAUPITI Ruutia A TA HA A ARUTUA m HUAHINE FAKARAVA b TATAKOTO i Niua Vaitoare RAIATEA e TAHITI r TAHAA ANAA RE AO Hakamaii MOORE A - HIK UE RU Fare Maeva MAIAO UA POU Faie HA O NUKUTAVAKE Fitii Apataki Tefarerii Maroe TUREIA Haapu Parea RIMATARA RURUTU A r c h Arutua HUAHINE i p e TUBUAI l d e s GAMBIE R Faanui Anau RA IVAVAE A u s Kaukura t r Nombre a l AR UTUA d'individus e s Taahuaia Moerai Mataura Nunue 20 000 Mataiva RA PA BOR A B OR A 10 000 Avera Tikehau 7 000 Rangiroa Hauti 3 500 Mahu Makatea 1 000 RURUT U TUBUAI RANGIROA ´ 0 110 Km So u r c e : Re c en se m en t d e la p o p u la ti o n 2 0 1 7 - IS P F -I N SE E Répartition de la population aux Îles Du Vent en 2017 TAHITI MAHINA Paopao Papetoai ARUE PAPEETE PIRAE HITIAA O TE RA FAAA Teavaro Tiarei Mahaena Haapiti PUNAAUIA Afareaitu Hitiaa Papenoo MOOREA 0 2 Km Faaone PAEA Papeari TAIARAPU-EST Mataiea Afaahiti Pueu Toahotu Nombre PAPARA d'individus TEVA I UTA Tautira 20 000 Vairao 15 000 13 000 Teahupoo 10 000 TAIARAPU-OUEST -

Emerging Infections: Microbial Threats to Health in the United States I
Emerging Infections: Microbial Threats to Health in the United States http://www.nap.edu/catalog/2008.html i EMERGING INFECTIONS riginal paper book, not from the Microbial Threats to Health in the United States the authoritative version for attribution. ing-specific formatting, however, cannot be Joshua Lederberg, Robert E. Shope, Stanley C. Oaks, Jr., Editors Committee on Emerging Microbial Threats to Health Division of Health Sciences Policy Division of International Health INSTITUTE OF MEDICINE NATIONAL ACADEMY PRESS Washington, D.C. 1992 About PDFthis file: This new digital representation of original workthe has been recomposed XMLfrom files created from o the original typesetting files. breaks Page are true the line lengths, word to original; breaks, heading styles, and other typesett aspublication this inserted.Please versionoftypographicerrors have been accidentallyretained, and some print use the may Copyright © National Academy of Sciences. All rights reserved. Emerging Infections: Microbial Threats to Health in the United States http://www.nap.edu/catalog/2008.html ii NATIONAL ACADEMY PRESS 2101 Constitution Avenue, N.W. Washington, D.C. 20418 NOTICE: The project that is the subject of this report was approved by the Governing Board of the National Research Council, whose members are drawn from the councils of the National Academy of Sciences, the National Academy of Engineering, and the Institute of Medicine. The members of the committee responsible for the report were chosen for their special competences and with regard for appropriate balance. This report has been reviewed by a group other than the authors according to procedures approved by a Report Review Committee consisting of members of the National Academy of Sci- ences, the National Academy of Engineering, and the Institute of Medicine. -

Weekly Bulletin on Outbreaks and Other Emergencies
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 28: 05 - 11 July 2021 Data as reported by: 17:00; 11 July 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 117 106 12 New event Ongoing events Outbreaks Humanitarian crises 146 082 3 836 Algeria ¤ 1 034 0 6 328 185 Mauritania 1 313 74 14 463 528 48 0 110 0 46 175 1 194 Niger 21 672 489 6 284 29 Mali 21 0 9 0 Cape Verde 6 471 16 4 954 174 Chad Eritrea Senegal 5 538 194 Gambia 66 0 33 006 289 1 414 8 Guinea-Bissau 847 17 Burkina Faso 2 060 56 277 071 4 343 168 552 2 124 Guinea 13 509 168 13 0 3 947 70 2 2 Benin 198 0 Nigeria 1 286 4 61 0 30 0 Ethiopia 13 2 6 995 50 556 5 872 15 Sierra Leone Togo 626 0 80 858 1 324 Ghana 7 142 98 Côte d'Ivoire 10 879 117 19 000 304 81 0 45 0 Liberia 17 0 South Sudan Central African Republic 1 313 2 0 25 0 50 14 0 97 585 801 6 738 221 Cameroon 24 117 299 3 0 48 776 318 35 339 197 7 0 58 0 199 2 1 411 30 9 1 620 1 188 754 3 722 2 0 168 0 1 1 6 031 112 14 270 133 8 790 122 Equatorial Guinea Uganda 867 2 827 9 Sao Tome and Principe 4 0 5 215 144 716 494 198 87 277 2 104 Kenya Gabon Legend Congo 3 516 93 305 26 Rwanda 8 199 104 2 392 37 48 244 560 25 164 162 Democratic Republic of the Congo 12 790 167 Burundi Measles Humanitarian crisis 5 686 8 Seychelles 44 139 980 436 0 693 57 Monkeypox Yellow fever United Republic of Tanzania 197 0 16 957 68 Meningitis Lassa fever 509 21 241 1 6 257 229 Leishmaniasis Cholera 39 958 935 175 729 2 822 Comoros Plague 304 3 cVDPV2 Angola Malawi Diarrhoeal disease in children under five years 36 926 1 250 -
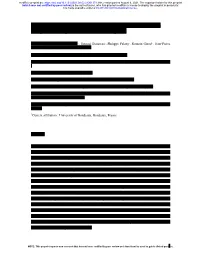
Modeling Spatiotemporal Aedes Aegypti Risk in French Guiana Using Meteorological and Remote Sensing Data
medRxiv preprint doi: https://doi.org/10.1101/2021.08.02.21261373; this version posted August 9, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Modeling spatiotemporal Aedes aegypti risk in French Guiana using meteorological and remote sensing data Sarah Bailly1,*, Vanessa Machault2, †,, Samuel Beneteau1, Philippe Palany3, Romain Girod4,5, Jean-Pierre Lacaux2, Philippe Quenel6, Claude Flamand1,7 1 Epidemiology unit, Institut Pasteur In French Guiana, French Guiana; 2 Aerology laboratory, Observatoire Midi-Pyrénées (OMP), Université Paul Sabatier Toulouse, France ; 3 Météo-France Antilles-Guyane, Martinique; 4 Medical entomology unit, Institut Pasteur in French Guiana, French Guiana 5 Current affiliation: Medical entomology unit, Institut Pasteur in Madagascar, Madagascar 6 Univ Rennes, Inserm, EHESP, Irset (Institut de recherche en santé, environnement et travail)— UMR_S 1085, F-35000 Rennes, France 7 Mathematical Modelling of Infectious Diseases Unit, Institut Pasteur, UMR2000, CNRS, Paris, France. †Current affiliation : University of Bordeaux, Bordeaux, France Abstract Although the development of vaccines for the prevention of arboviral diseases has been a priority in recent years, prevention strategies continue to depend on vector control. Risk maps at scales appropriate for these strategies can provide valuable information to assess entomological risk levels and guide actions. We used a spatio-temporal modeling approach to predict, at the local scale, the risk of homes potentially harboring Aedes aegypti larvae. The model used integrated larvae risk data collected in the field from September 2011 to February 2013, environmental data obtained from very high spatial resolution Pleiades imagery, and daily meteorological data, collected in the city of Matoury in French Guiana. -

Trinidad and Tobago
Riskline / Country Report / 29 August 2021 TRINIDAD AND TOBAGO Overall risk level High Reconsider travel Can be dangerous and may present unexpected security risks Travel is possible, but there is a potential for disruptions Overview Emergency Numbers Medical 811 Upcoming Events There are no upcoming events scheduled Riskline / Country Report / 29 August 2021 / Trinidad and Tobago 2 Travel Advisories Riskline / Country Report / 29 August 2021 / Trinidad and Tobago 3 Summary Trinidad and Tobago is a High Risk destination: reconsider travel. High Risk locations can be dangerous and may present unexpected security risks. Travel is possible, but there is a potential for severe or widespread disruptions. Covid-19 High Risk A steep uptick in infections reported as part of a second wave in April-June prompted authorities to reimpose restrictions on movement and business operations. Infection rates are increasing again since July. International travel remains limited to vaccinated travellers only. Political Instability Low Risk A parliamentary democracy led by centrist Prime Minister Keith Rowley, Trinidad and Tobago's democracy is firmly entrenched thanks to a well-established system of checks and balances that helped it remain resilient in the face of sources of instability like politically motivated murders in 1980 and an Islamist coup attempt in 1990. Despite its status as a regional and economic leader in the Caribbean, the nation faces challenges of corruption allegations in the highest level of government and an extensive drug trade and associated crime that affects locals and tourists alike. Conflict Low Risk Trinidad and Tobago has been engaged in a long-standing, and at times confrontational, dispute over fishing rights with Barbados that also encompasses other resources like oil and gas. -

Mosquito-Born Dengue Fever Threat Spreading in the Americas
NRDC Issue Paper July 2009 Fever Pitch Mosquito-Borne Dengue Fever Threat Spreading in the Americas Authors Kim Knowlton, Dr.P.H. Gina Solomon, M.D., M.P.H. Miriam Rotkin-Ellman, M.P.H. Natural Resources Defense Council About NRDC The Natural Resources Defense Council (NRDC) is an international nonprofit environmental organization with more than 1.2 million members and online activists. Since 1970, our lawyers, scientists, and other environmental specialists have worked to protect the world’s natural resources, public health, and the environment. NRDC has offices in New York City, Washington, D.C., Los Angeles, San Francisco, Chicago, Montana, and Beijing. Visit us at www.nrdc.org. Acknowledgments The authors would like to thank Zev Ross and Hollie Kitson of ZevRoss Spatial Analysis, Ithaca, New York, for conducting the mapping, and to Sashti Balasundaram for dengue case data research. Dr. Chester G. Moore of Colorado State University generously provided access to mosquito occurrence data. We would also like to thank Cindy and Alan Horn for their support of NRDC’s Global Warming and Health Project. We are grateful to the following peer reviewers who provided invaluable comments on this report: Chester Moore, Colorado State University; Kristie L. Ebi, ESS, LLC; Joan Brunkard, U.S. Centers for Disease Control and Prevention; Mary Hayden, National Center for Atmospheric Research Institute for the Study of Society and Environment. NRDC Director of Communications: Phil Gutis NRDC Marketing and Operations Director: Alexandra Kennaugh NRDC Publications Director: Lisa Goffredi NRDC Publications Editor: Anthony Clark Production: Jon Prinsky Copyright 2009 by the Natural Resources Defense Council. -

Increasing Risk of Dengue Transmission Potential Using Climate and Non-Climate Datasets Jung-Seok Lee1* and Andrew Farlow2
Lee and Farlow BMC Public Health (2019) 19:934 https://doi.org/10.1186/s12889-019-7282-3 RESEARCH ARTICLE Open Access The threat of climate change to non- dengue-endemic countries: increasing risk of dengue transmission potential using climate and non-climate datasets Jung-Seok Lee1* and Andrew Farlow2 Abstract Background: Dengue is a major public health problem in the tropics and sub-tropics, but the disease is less known to non-dengue-endemic countries including in Northeast Asia. However, an unexpected dengue outbreak occurred in 2014 in Japan. Given that autochthonous (domestic) dengue cases had not been reported for the past 70 years in Japan, this outbreak was highly unusual and suggests that several environmental factors might have changed in a way that favors vector mosquitoes in the Northeast Asian region. Methods: A Climate Risk Factor (CRF) index, as validated in previous work, was constructed using climate and non- climate factors. This CRF index was compared to the number of reported dengue cases in Tokyo, Japan where the outbreak was observed in 2014. In order to identify high-risk areas, the CRF index was further estimated at the 5 km by 5 km resolution and mapped for Japan and South Korea. Results: The high-risk areas determined by the CRF index corresponded well to the provinces where a high number of autochthonous cases were reported during the outbreak in Japan. At the provincial-level, high-risk areas for dengue fever were the Eastern part of Tokyo and Kanakawa, the South-Eastern part of Saitama, and the North-Western part of Chiba. -

The Case of Chikungunya in French Guiana
Am. J. Trop. Med. Hyg., 97(2), 2017, pp. 344–355 doi:10.4269/ajtmh.16-1028 Copyright © 2017 by The American Society of Tropical Medicine and Hygiene The Role of Risk Proximity in the Beliefs and Behaviors Related to Mosquito-Borne Diseases: The Case of Chikungunya in French Guiana Claude Flamand,1† Camille Fritzell,1† Pauline Obale,2 Philippe Quenel,2,3 and Jocelyn Raude2,4,5* 1United ´ ’Epid´ emiologie, ´ Institut Pasteur de la Guyane, Cayenne, France; 2Ecole des Hautes Etudes en Sante ´ Publique, Universite ´ Sorbonne Paris Cite, ´ Rennes, France; 3UMR Inserm 1085-IRSET Institut de Recherche sur la Sante, ´ l’Environnement et le Travail, Rennes, France; 4UMR 190 EPV “Emergence des Pathologies Virales,” Aix-Marseille University, IRD 190, INSERM 1207, EHESP, Marseille, France; 5UMR “Processus Infectieux en Milieu Insulaire Tropical,” INSERM 1187, CNRS 9192, IRD 249, UniversitedeLaR´ ´ eunion, Saint-Denis, France Abstract. Human behaviors are increasingly recognized to play a key role in the spread of infectious diseases. Although a set of social and cognitive determinants has been consistently found to affect the adoption of health protective behaviors aiming to control and prevent a variety of infections, little is currently known about the ecological drivers of these behaviors in epidemic settings. In this article, we took advantage of the outbreak of chikungunya, a reemerging mosquito- borne disease, that occurred in French Guiana in 2014–15 to test empirically the assumption proposed by Zielinski- Gutierrez and Hayden that the proximity of the disease and perceptions of the natural environment may considerably shape public response to an emerging health threat. -

Epidemiological Analysis of the Kaohsiung City Strategy for Dengue Fever Quarantine and Epidemic Prevention
Epidemiological analysis of the Kaohsiung city strategy for dengue fever quarantine and epidemic prevention Chun-Hong CHEN ( [email protected] ) National Health Research Institutes Chao Ying Pan Department of Health ,Kaohsiung city Goverment, Taiwan Wei-Liang Liu NMDBC, NHRI Matthew P. Su The University of Manchester Faculty of Biology Medicine and Health Te Pin Chang NMDBC, NHRI Hui-Pin Ho Department of Health, Kaohsiung city Government Joh-Jong Huang Bureau of Social Affairs, Tainan city Government Li Jen Lin Department of Health, Kaohsiung city Government Research article Keywords: Dengue virus, Imported dengue cases, Concealment, Indigenous dengue fever, Airport fever screening, Noncontact infrared thermometers Posted Date: October 1st, 2019 DOI: https://doi.org/10.21203/rs.2.15494/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published at BMC Infectious Diseases on May 15th, 2020. See the published version at https://doi.org/10.1186/s12879-020-4942-y. Page 1/13 Abstract Abstract Background. Dengue is endemic in over 100 countries and is an important public health problem worldwide. Dengue is not considered endemic in Taiwan however, with importation of dengue viruses from neighboring countries via close commercial links and air travel believed to be the cause of local outbreaks. Disease control efforts have therefore focused on preventing the importation of dengue into Taiwan. Here, we investigate the relationships between numbers of imported and indigenous dengue cases to test the validity of this strategy. Methods. Dengue-fever case data from between 2013 and 2018 was obtained from the surveillance systems of the Taiwan Center for Disease Control and Kaohsiung City Health department. -

“Break-Bone” Fever in Philadelphia, 1780: Reflections on the History of Disease
The Fielding H. Garrison Lecture: “Break-Bone” Fever in Philadelphia, 1780: Reflections on the History of Disease Randall M. Packard Bulletin of the History of Medicine, Volume 90, Number 2, Summer 2016, pp. 193-221 (Article) Published by Johns Hopkins University Press DOI: https://doi.org/10.1353/bhm.2016.0041 For additional information about this article https://muse.jhu.edu/article/622044 [ Access provided at 3 Oct 2021 02:47 GMT with no institutional affiliation ] THE FIELDING H. GARRISON LECTURE “Break-Bone” Fever in Philadelphia, 1780: Reflections on the History of Disease RANDALL M. PACKARD Summary: In the Autumn of 1780 an epidemic hit the city of Philadelphia. The symptoms of the disease resembled those of present day dengue fever, and sub- sequent observers argued that the disease was in fact dengue. But was it? The question forces us to confront the challenges of retrospective epidemiology and how we examine the history of a disease. This paper examines the 1780 epidemic from two perspectives. First, it looks at evidence that the disease was dengue and examines what this tells us about the epidemic and the conditions that caused it. Second, it looks at the disease from the perspective of Dr. Benjamin Rush, who treated hundreds of patients during the epidemic. In other words, it examines the disease through the lens of eighteenth century medical ideas. The paper concludes that each approach is valuable and reveals different aspects of the relationship between society and disease. Keywords: breakbone fever, dengue, Benjamin Rush, Philadelphia, epidemics The summer of 1780 was filled with promise for the residents of Phila- delphia. -

Political Reviews
Political Reviews Micronesia in Review: Issues and Events, 1 July 2010 to 30 June 2011 john r haglelgam, david w kupferman, kelly g marsh, samuel f mcphetres, donald r shuster, tyrone j taitano Polynesia in Review: Issues and Events, 1 July 2010 to 30 June 2011 lorenz gonschor, hapakuke pierre leleivai, margaret mutu, forrest wade young © 2012 by University of Hawai‘i Press 135 Polynesia in Review: Issues and Events, 1 July 2010 to 30 June 2011 Reviews of American Sëmoa, Cook claimed Tahoeraa to be an opposition Islands, Hawai‘i, Niue, Tokelau, party. During a budgetary debate on Tonga, and Tuvalu are not included in 2 August, Tahoeraa representatives this issue. charged Tong Sang with incompetency to lead the country and called on him French Polynesia to resign (tp, 2 Aug 2010). The period under review was not par- Tahoeraa’s confusing attitude of ticularly rich in new events. While no attacking the president and demand- economic recovery was in sight, local ing his resignation, while at the same politicians, fed by French subsidies, time allowing its members to keep continued their games of making and their cabinet portfolios, can only be unmaking majorities in the Assembly understood by looking at the pecu- of French Polynesia, culminating in liarities of French Polynesia’s political the eleventh change of government system. As long as Tong Sang did not since 2004. The only possibly inter- resign, he could only be overthrown esting development is that the new by a constructive vote of no confi- pro-independence majority now wants dence, which would require an overall to internationalize the country’s prob- majority and entail the automatic lems and get it out of the grip of Paris.