Weekly Bulletin on Outbreaks and Other Emergencies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Addressing Root Causes of Conflict: a Case Study Of
Experience paper Addressing root causes of conflict: A case study of the International Security and Stabilization Support Strategy and the Patriotic Resistance Front of Ituri (FRPI) in Ituri Province, eastern Democratic Republic of Congo Oslo, May 2019 1 About the Author: Ingebjørg Finnbakk has been deployed by the Norwegian Resource Bank for Democracy and Human Rights (NORDEM) to the Stabilization Support Unit (SSU) in MONUSCO from August 2016 until February 2019. Together with SSU Headquarters and Congolese partners she has been a key actor in developing and implementing the ISSSS program in Ituri Province, leading to a joint MONUSCO and Government process and strategy aimed at demobilizing a 20-year-old armed group in Ituri, the Patriotic Resistance Front of Ituri (FRPI). The views expressed in this report are her own, and do not represent those of either the UN or the Norwegian Refugee Council/NORDEM. About NORDEM: The Norwegian Resource Bank for Democracy and Human Rights (NORDEM) is NORCAP’s civilian capacity provider specializing in human rights and support for democracy. NORDEM has supported the SSU with personnel since 2013, hence contribution significantly with staff through the various preparatory phases as well as during the implementation. Acknowledgements: Reaching the point of implementing ISSSS phase two programs has required a lot of analyses, planning and stakeholder engagement. The work presented in this report would not be possible without all the efforts of previous SSU staff under the leadership of Richard de La Falaise. The FRPI process would not have been possible without the support and visions from Francois van Lierde (deployed by NORDEM) and Frances Charles at SSU HQ level. -

Emerging Infections: Microbial Threats to Health in the United States I
Emerging Infections: Microbial Threats to Health in the United States http://www.nap.edu/catalog/2008.html i EMERGING INFECTIONS riginal paper book, not from the Microbial Threats to Health in the United States the authoritative version for attribution. ing-specific formatting, however, cannot be Joshua Lederberg, Robert E. Shope, Stanley C. Oaks, Jr., Editors Committee on Emerging Microbial Threats to Health Division of Health Sciences Policy Division of International Health INSTITUTE OF MEDICINE NATIONAL ACADEMY PRESS Washington, D.C. 1992 About PDFthis file: This new digital representation of original workthe has been recomposed XMLfrom files created from o the original typesetting files. breaks Page are true the line lengths, word to original; breaks, heading styles, and other typesett aspublication this inserted.Please versionoftypographicerrors have been accidentallyretained, and some print use the may Copyright © National Academy of Sciences. All rights reserved. Emerging Infections: Microbial Threats to Health in the United States http://www.nap.edu/catalog/2008.html ii NATIONAL ACADEMY PRESS 2101 Constitution Avenue, N.W. Washington, D.C. 20418 NOTICE: The project that is the subject of this report was approved by the Governing Board of the National Research Council, whose members are drawn from the councils of the National Academy of Sciences, the National Academy of Engineering, and the Institute of Medicine. The members of the committee responsible for the report were chosen for their special competences and with regard for appropriate balance. This report has been reviewed by a group other than the authors according to procedures approved by a Report Review Committee consisting of members of the National Academy of Sci- ences, the National Academy of Engineering, and the Institute of Medicine. -

A Life of Fear and Flight
A LIFE OF FEAR AND FLIGHT The Legacy of LRA Brutality in North-East Democratic Republic of the Congo We fled Gilima in 2009, as the LRA started attacking there. From there we fled to Bangadi, but we were confronted with the same problem, as the LRA was attacking us. We fled from there to Niangara. Because of insecurity we fled to Baga. In an attack there, two of my children were killed, and one was kidnapped. He is still gone. Two family members of my husband were killed. We then fled to Dungu, where we arrived in July 2010. On the way, we were abused too much by the soldiers. We were abused because the child of my brother does not understand Lingala, only Bazande. They were therefore claiming we were LRA spies! We had to pay too much for this. We lost most of our possessions. Once in Dungu, we were first sleeping under a tree. Then someone offered his hut. It was too small with all the kids, we slept with twelve in one hut. We then got another offer, to sleep in a house at a church. The house was, however, collapsing and the owner chased us. He did not want us there. We then heard that some displaced had started a camp, and that we could get a plot there. When we had settled there, it turned out we had settled outside of the borders of the camp, and we were forced to leave. All the time, we could not dig and we had no access to food. -

Democratic Republic of the Congo Complex Emergency Fact Sheet #2
DEMOCRATIC REPUBLIC OF THE CONGO - COMPLEX EMERGENCY FACT SHEET #2, FISCAL YEAR (FY) 2018 MARCH 9, 2018 NUMBERS AT USAID/OFDA1 FUNDING HIGHLIGHTS BY SECTOR IN FY 2017–2018 A GLANCE • Conflict continues to displace 3% 3% populations within DRC and to 6% neighboring countries 6% 13.1 34% • requestsUN nearly $1.7 billion to meet 7% humanitarian needs in DRC during million 2018 People in DRC Requiring 18% • Cholera and polio type 2 remain critical Humanitarian Assistance 23% in 2018 health concerns UN – December 2017 Logistics Support & Relief Commodities (34%) Health (23%) HUMANITARIAN FUNDING Water, Sanitation & Hygiene (18%) FOR THE DRC RESPONSE IN FY 2017–2018 Protection (7%) Humanitarian Coordination & Information Management (6%) 7.7 Agriculture & Food Security (6%) USAID/OFDA $52,686,506 Nutrition (3%) million Other (3%) USAID/FFP $77,115,857 Acutely Food-Insecure 2 3 People in DRC USAID/FFP FUNDING State/PRM $62,496,034 UN – August 2017 BY MODALITY IN FY 2017–2018 48% 39% 11% 2% Local & Regional Procurement (48%) $192,298,397 U.S. In-Kind Food Aid (39%) 4.5 Cash Transfers for Food (11%) Complementary Services (2%) million IDPs in DRC UN – December 2017 KEY DEVELOPMENTS • The 2018 Humanitarian Response Plan (HRP) requests nearly $1.7 billion to provide humanitarian assistance to 10.5 million of the estimated 13.1 million people in need in 684,000 Democratic Republic of the Congo (DRC). The 2018 appeal is the largest to date for DRC and reflects the widening scope of emergency needs in the country. DRC Refugees and Asylum-Seekers Across • Conflict continues to drive population displacement in DRC, with the UN projecting up Africa to 2.4 million new internally displaced persons (IDPs) by the end of 2018. -
Modeling Spatiotemporal Aedes Aegypti Risk in French Guiana Using Meteorological and Remote Sensing Data
medRxiv preprint doi: https://doi.org/10.1101/2021.08.02.21261373; this version posted August 9, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Modeling spatiotemporal Aedes aegypti risk in French Guiana using meteorological and remote sensing data Sarah Bailly1,*, Vanessa Machault2, †,, Samuel Beneteau1, Philippe Palany3, Romain Girod4,5, Jean-Pierre Lacaux2, Philippe Quenel6, Claude Flamand1,7 1 Epidemiology unit, Institut Pasteur In French Guiana, French Guiana; 2 Aerology laboratory, Observatoire Midi-Pyrénées (OMP), Université Paul Sabatier Toulouse, France ; 3 Météo-France Antilles-Guyane, Martinique; 4 Medical entomology unit, Institut Pasteur in French Guiana, French Guiana 5 Current affiliation: Medical entomology unit, Institut Pasteur in Madagascar, Madagascar 6 Univ Rennes, Inserm, EHESP, Irset (Institut de recherche en santé, environnement et travail)— UMR_S 1085, F-35000 Rennes, France 7 Mathematical Modelling of Infectious Diseases Unit, Institut Pasteur, UMR2000, CNRS, Paris, France. †Current affiliation : University of Bordeaux, Bordeaux, France Abstract Although the development of vaccines for the prevention of arboviral diseases has been a priority in recent years, prevention strategies continue to depend on vector control. Risk maps at scales appropriate for these strategies can provide valuable information to assess entomological risk levels and guide actions. We used a spatio-temporal modeling approach to predict, at the local scale, the risk of homes potentially harboring Aedes aegypti larvae. The model used integrated larvae risk data collected in the field from September 2011 to February 2013, environmental data obtained from very high spatial resolution Pleiades imagery, and daily meteorological data, collected in the city of Matoury in French Guiana. -

Trinidad and Tobago
Riskline / Country Report / 29 August 2021 TRINIDAD AND TOBAGO Overall risk level High Reconsider travel Can be dangerous and may present unexpected security risks Travel is possible, but there is a potential for disruptions Overview Emergency Numbers Medical 811 Upcoming Events There are no upcoming events scheduled Riskline / Country Report / 29 August 2021 / Trinidad and Tobago 2 Travel Advisories Riskline / Country Report / 29 August 2021 / Trinidad and Tobago 3 Summary Trinidad and Tobago is a High Risk destination: reconsider travel. High Risk locations can be dangerous and may present unexpected security risks. Travel is possible, but there is a potential for severe or widespread disruptions. Covid-19 High Risk A steep uptick in infections reported as part of a second wave in April-June prompted authorities to reimpose restrictions on movement and business operations. Infection rates are increasing again since July. International travel remains limited to vaccinated travellers only. Political Instability Low Risk A parliamentary democracy led by centrist Prime Minister Keith Rowley, Trinidad and Tobago's democracy is firmly entrenched thanks to a well-established system of checks and balances that helped it remain resilient in the face of sources of instability like politically motivated murders in 1980 and an Islamist coup attempt in 1990. Despite its status as a regional and economic leader in the Caribbean, the nation faces challenges of corruption allegations in the highest level of government and an extensive drug trade and associated crime that affects locals and tourists alike. Conflict Low Risk Trinidad and Tobago has been engaged in a long-standing, and at times confrontational, dispute over fishing rights with Barbados that also encompasses other resources like oil and gas. -

Mosquito-Born Dengue Fever Threat Spreading in the Americas
NRDC Issue Paper July 2009 Fever Pitch Mosquito-Borne Dengue Fever Threat Spreading in the Americas Authors Kim Knowlton, Dr.P.H. Gina Solomon, M.D., M.P.H. Miriam Rotkin-Ellman, M.P.H. Natural Resources Defense Council About NRDC The Natural Resources Defense Council (NRDC) is an international nonprofit environmental organization with more than 1.2 million members and online activists. Since 1970, our lawyers, scientists, and other environmental specialists have worked to protect the world’s natural resources, public health, and the environment. NRDC has offices in New York City, Washington, D.C., Los Angeles, San Francisco, Chicago, Montana, and Beijing. Visit us at www.nrdc.org. Acknowledgments The authors would like to thank Zev Ross and Hollie Kitson of ZevRoss Spatial Analysis, Ithaca, New York, for conducting the mapping, and to Sashti Balasundaram for dengue case data research. Dr. Chester G. Moore of Colorado State University generously provided access to mosquito occurrence data. We would also like to thank Cindy and Alan Horn for their support of NRDC’s Global Warming and Health Project. We are grateful to the following peer reviewers who provided invaluable comments on this report: Chester Moore, Colorado State University; Kristie L. Ebi, ESS, LLC; Joan Brunkard, U.S. Centers for Disease Control and Prevention; Mary Hayden, National Center for Atmospheric Research Institute for the Study of Society and Environment. NRDC Director of Communications: Phil Gutis NRDC Marketing and Operations Director: Alexandra Kennaugh NRDC Publications Director: Lisa Goffredi NRDC Publications Editor: Anthony Clark Production: Jon Prinsky Copyright 2009 by the Natural Resources Defense Council. -
DRC Complex Emergency Fact Sheet #5 09.30.2020
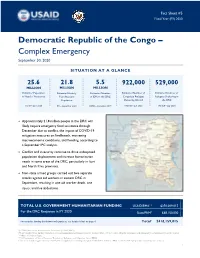
Fact Sheet #5 Fiscal Year (FY) 2020 Democratic Republic of the Congo – Complex Emergency September 30, 2020 SITUATION AT A GLANCE 25.6 21.8 5.5 922,000 529,000 MILLION MILLION MILLION Estimated Population Estimated Acutely Estimated Number Estimated Number of Estimated Number of in Need of Assistance Congolese Refugees Refugees Sheltering in Food Insecure of IDPs in the DRC Population Sheltering Abroad the DRC OCHA – June 2020 UNHCR – July 2020 UNHCR – July 2020 IPC – September 2020 OCHA – December 2019 Approximately 21.8 million people in the DRC will likely require emergency food assistance through December due to conflict, the impact of COVID-19 mitigation measures on livelihoods, worsening macroeconomic conditions, and flooding, according to a September IPC analysis. Conflict and insecurity continue to drive widespread population displacement and increase humanitarian needs in some areas of the DRC, particularly in Ituri and North Kivu provinces. Non-state armed groups carried out two separate attacks against aid workers in eastern DRC in September, resulting in one aid worker death, one injury, and five abductions. TOTAL U.S. GOVERNMENT HUMANITARIAN FUNDING USAID/BHA1,2 $350,009,015 For the DRC Response in FY 2020 State/PRM3 $68,150,000 For complete funding breakdown with partners, see detailed chart on page 6 Total4 $418,159,015 1USAID’s Bureau for Humanitarian Assistance (USAID/BHA) 2 Total USAID/BHA funding includes non-food humanitarian assistance from the former Office of U.S. Foreign Disaster Assistance and emergency food assistance from the former Office of Food for Peace. 3 U.S. Department of State’s Bureau of Population, Refugees, and Migration (State/PRM) 4 This total includes approximately $23,833,699 in supplemental funding through USAID/BHA and State/PRM for COVID-19 preparedness and response activities. -

Increasing Risk of Dengue Transmission Potential Using Climate and Non-Climate Datasets Jung-Seok Lee1* and Andrew Farlow2
Lee and Farlow BMC Public Health (2019) 19:934 https://doi.org/10.1186/s12889-019-7282-3 RESEARCH ARTICLE Open Access The threat of climate change to non- dengue-endemic countries: increasing risk of dengue transmission potential using climate and non-climate datasets Jung-Seok Lee1* and Andrew Farlow2 Abstract Background: Dengue is a major public health problem in the tropics and sub-tropics, but the disease is less known to non-dengue-endemic countries including in Northeast Asia. However, an unexpected dengue outbreak occurred in 2014 in Japan. Given that autochthonous (domestic) dengue cases had not been reported for the past 70 years in Japan, this outbreak was highly unusual and suggests that several environmental factors might have changed in a way that favors vector mosquitoes in the Northeast Asian region. Methods: A Climate Risk Factor (CRF) index, as validated in previous work, was constructed using climate and non- climate factors. This CRF index was compared to the number of reported dengue cases in Tokyo, Japan where the outbreak was observed in 2014. In order to identify high-risk areas, the CRF index was further estimated at the 5 km by 5 km resolution and mapped for Japan and South Korea. Results: The high-risk areas determined by the CRF index corresponded well to the provinces where a high number of autochthonous cases were reported during the outbreak in Japan. At the provincial-level, high-risk areas for dengue fever were the Eastern part of Tokyo and Kanakawa, the South-Eastern part of Saitama, and the North-Western part of Chiba. -

The Case of Chikungunya in French Guiana
Am. J. Trop. Med. Hyg., 97(2), 2017, pp. 344–355 doi:10.4269/ajtmh.16-1028 Copyright © 2017 by The American Society of Tropical Medicine and Hygiene The Role of Risk Proximity in the Beliefs and Behaviors Related to Mosquito-Borne Diseases: The Case of Chikungunya in French Guiana Claude Flamand,1† Camille Fritzell,1† Pauline Obale,2 Philippe Quenel,2,3 and Jocelyn Raude2,4,5* 1United ´ ’Epid´ emiologie, ´ Institut Pasteur de la Guyane, Cayenne, France; 2Ecole des Hautes Etudes en Sante ´ Publique, Universite ´ Sorbonne Paris Cite, ´ Rennes, France; 3UMR Inserm 1085-IRSET Institut de Recherche sur la Sante, ´ l’Environnement et le Travail, Rennes, France; 4UMR 190 EPV “Emergence des Pathologies Virales,” Aix-Marseille University, IRD 190, INSERM 1207, EHESP, Marseille, France; 5UMR “Processus Infectieux en Milieu Insulaire Tropical,” INSERM 1187, CNRS 9192, IRD 249, UniversitedeLaR´ ´ eunion, Saint-Denis, France Abstract. Human behaviors are increasingly recognized to play a key role in the spread of infectious diseases. Although a set of social and cognitive determinants has been consistently found to affect the adoption of health protective behaviors aiming to control and prevent a variety of infections, little is currently known about the ecological drivers of these behaviors in epidemic settings. In this article, we took advantage of the outbreak of chikungunya, a reemerging mosquito- borne disease, that occurred in French Guiana in 2014–15 to test empirically the assumption proposed by Zielinski- Gutierrez and Hayden that the proximity of the disease and perceptions of the natural environment may considerably shape public response to an emerging health threat. -

Epidemiological Analysis of the Kaohsiung City Strategy for Dengue Fever Quarantine and Epidemic Prevention
Epidemiological analysis of the Kaohsiung city strategy for dengue fever quarantine and epidemic prevention Chun-Hong CHEN ( [email protected] ) National Health Research Institutes Chao Ying Pan Department of Health ,Kaohsiung city Goverment, Taiwan Wei-Liang Liu NMDBC, NHRI Matthew P. Su The University of Manchester Faculty of Biology Medicine and Health Te Pin Chang NMDBC, NHRI Hui-Pin Ho Department of Health, Kaohsiung city Government Joh-Jong Huang Bureau of Social Affairs, Tainan city Government Li Jen Lin Department of Health, Kaohsiung city Government Research article Keywords: Dengue virus, Imported dengue cases, Concealment, Indigenous dengue fever, Airport fever screening, Noncontact infrared thermometers Posted Date: October 1st, 2019 DOI: https://doi.org/10.21203/rs.2.15494/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published at BMC Infectious Diseases on May 15th, 2020. See the published version at https://doi.org/10.1186/s12879-020-4942-y. Page 1/13 Abstract Abstract Background. Dengue is endemic in over 100 countries and is an important public health problem worldwide. Dengue is not considered endemic in Taiwan however, with importation of dengue viruses from neighboring countries via close commercial links and air travel believed to be the cause of local outbreaks. Disease control efforts have therefore focused on preventing the importation of dengue into Taiwan. Here, we investigate the relationships between numbers of imported and indigenous dengue cases to test the validity of this strategy. Methods. Dengue-fever case data from between 2013 and 2018 was obtained from the surveillance systems of the Taiwan Center for Disease Control and Kaohsiung City Health department. -

“Break-Bone” Fever in Philadelphia, 1780: Reflections on the History of Disease
The Fielding H. Garrison Lecture: “Break-Bone” Fever in Philadelphia, 1780: Reflections on the History of Disease Randall M. Packard Bulletin of the History of Medicine, Volume 90, Number 2, Summer 2016, pp. 193-221 (Article) Published by Johns Hopkins University Press DOI: https://doi.org/10.1353/bhm.2016.0041 For additional information about this article https://muse.jhu.edu/article/622044 [ Access provided at 3 Oct 2021 02:47 GMT with no institutional affiliation ] THE FIELDING H. GARRISON LECTURE “Break-Bone” Fever in Philadelphia, 1780: Reflections on the History of Disease RANDALL M. PACKARD Summary: In the Autumn of 1780 an epidemic hit the city of Philadelphia. The symptoms of the disease resembled those of present day dengue fever, and sub- sequent observers argued that the disease was in fact dengue. But was it? The question forces us to confront the challenges of retrospective epidemiology and how we examine the history of a disease. This paper examines the 1780 epidemic from two perspectives. First, it looks at evidence that the disease was dengue and examines what this tells us about the epidemic and the conditions that caused it. Second, it looks at the disease from the perspective of Dr. Benjamin Rush, who treated hundreds of patients during the epidemic. In other words, it examines the disease through the lens of eighteenth century medical ideas. The paper concludes that each approach is valuable and reveals different aspects of the relationship between society and disease. Keywords: breakbone fever, dengue, Benjamin Rush, Philadelphia, epidemics The summer of 1780 was filled with promise for the residents of Phila- delphia.