Evaluation and Management of Lymphadenopathy in Children Alison M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supraclavicular Artery Island Flap in Head and Neck Reconstruction
European Annals of Otorhinolaryngology, Head and Neck diseases 132 (2015) 291–294 View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Available online at ScienceDirect www.sciencedirect.com Technical note Supraclavicular artery island flap in head and neck reconstruction a b a,c a,∗,c S. Atallah , A. Guth , F. Chabolle , C.-A. Bach a Service de chirurgie ORL et cervico-faciale, hôpital Foch, 40 rue Worth, 92150 Suresnes, France b Service de radiologie, hôpital Foch, 40, rue Worth, 92150 Suresnes, France c Université de Versailles Saint-Quentin en Yvelines, UFR de médecine Paris Ouest Saint-Quentin-en-Yvelines, 78280 Guyancourt, France a r t i c l e i n f o a b s t r a c t Keywords: Due to the complex anatomy of the head and neck, a wide range of pedicled or free flaps must be available Supraclavicular artery island flap to ensure optimal reconstruction of the various defects resulting from cancer surgery. The supraclavi- Fasciocutaneous flap cular artery island flap is a fasciocutaneous flap harvested from the supraclavicular and deltoid regions. Head and neck cancer The blood supply of this flap is derived from the supraclavicular artery, a direct cutaneous branch of the Reconstructive surgery transverse cervical artery in 93% of cases or the supraclavicular artery in 7% of cases. The supraclavicular artery is located in a triangle delineated by the posterior border of the sternocleidomastoid muscle medi- ally, the external jugular vein posteriorly, and the median portion of the clavicle anteriorly. -

Left Supraclavicular Lymphadenopathy As the Only Clinical Presentation of Prostate Cancer: a Case Report
ACTA MEDICA MARTINIANA 2017 17/2 DOI: 10.1515/acm-2017-0011 41 LEFT SUPRACLAVICULAR LYMPHADENOPATHY AS THE ONLY CLINICAL PRESENTATION OF PROSTATE CANCER: A CASE REPORT MOHANAD ABUSULTAN1, HANZEL P2, DURCANSKY D3, HAJTMAN A3. 1Department of Otorhinolaryngology, Prievidza Hospital, Slovak Republic 2Comenius University, Jessenius Faculty of Medicine and University Hospital in Martin, Clinic of Otorhinolaryngology, Head and Neck Surgery, Martin, Slovak Republic 3Department of Pathology, Prievidza Hospital, Slovak Republic A bstract Prostate cancer usually metastasis to the regional lymph nodes and can rarely metastases to nonregional supradi- aphragmatic lymph nodes. Cervical lymph node metastasis of prostate cancer is extremely rare. However, it should be considered in the differential diagnosis of cervical lymphadenopathy in male patients with adenocarcinoma of unknown primary site. In this report we present a rare case of metastatic prostate adenocarcinoma with left supra- clavicular lymphadenopathy as the only clinical presentation with no other evidence of metastasis to the regional lymph nodes or bone metastasis. Key words: Prostate cancer, Supraclavicular lymphadenopathy, Metastasis INTRODUCTION Most of cancer metastasis to the cervical lymph nodes is from cancers of the mucosal surfaces of the upper aerodigestive tract. The second most common source of metastasis is nonmucosal tumors in the head and neck such as salivary glands, thyroid glands and skin [1]. Cancers originating from sites other than the head and neck can rarely metastasize to the cervical lymph nodes. However, neoplasms of the genitourinary tract make up a sig- nificant proportion of these cancers and should be considered in the differential diagnosis of neoplastic lesions of the head and neck [2]. -

A Pocket Manual of Percussion And
r — TC‘ B - •' ■ C T A POCKET MANUAL OF PERCUSSION | AUSCULTATION FOB PHYSICIANS AND STUDENTS. TRANSLATED FROM THE SECOND GERMAN EDITION J. O. HIRSCHFELDER. San Fbancisco: A. L. BANCROFT & COMPANY, PUBLISHEBS, BOOKSELLEBS & STATIONEB3. 1873. Entered according to Act of Congress, in the year 1872, By A. L. BANCROFT & COMPANY, Iii the office of the Librarian of Congress, at Washington. TRAN jLATOR’S PREFACE. However numerou- the works that have been previously published in the Fi 'lish language on the subject of Per- cussion and Auscultation, there has ever existed a lack of a complete yet concise manual, suitable for the pocket. The translation of this work, which is extensively used in the Universities of Germany, is intended to supply this want, and it is hoped will prove a valuable companion to the careful student and practitioner. J. 0. H. San Francisco, November, 1872. PERCUSSION. For the practice of percussion we employ a pleximeter, or a finger, upon which we strike with a hammer, or a finger, producing a sound, the character of which varies according to the condition of the organs lying underneath the spot percussed. In order to determine the extent of the sound produced, we may imagine the following lines to be drawr n upon the chest: (1) the mammary line, which begins at the union of the inner and middle third of the clavicle, and extends downwards through the nipple; (2) the paraster- nal line, which extends midway between the sternum and nipple ; (3) the axillary line, which extends from the centre of the axilla to the end of the 11th rib. -
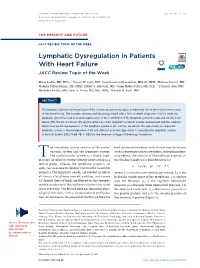
Lymphatic Dysregulation in Patients with Heart Failure JACC Review Topic of the Week
JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 78, NO. 1, 2021 ª 2021 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION PUBLISHED BY ELSEVIER THE PRESENT AND FUTURE JACC REVIEW TOPIC OF THE WEEK Lymphatic Dysregulation in Patients With Heart Failure JACC Review Topic of the Week a,b c d e Marat Fudim, MD, MHS, Husam M. Salah, MD, Janarthanan Sathananthan, MBCHB, MPH, Mathieu Bernier, MD, f g e,h i Waleska Pabon-Ramos, MD, MPH, Robert S. Schwartz, MD, Josep Rodés-Cabau, MD, PHD, François Côté, MD, j d a,b Abubaker Khalifa, MD, Sean A. Virani, MD, MSC, MPH, Manesh R. Patel, MD ABSTRACT The lymphatic system is an integral part of the circulatory system and plays an important role in the volume homeostasis of the human body. The complex anatomy and physiology paired with a lack of simple diagnostic tools to study the lymphatic system have led to an underappreciation of the contribution of the lymphatic system to acute and chronic heart failure (HF). Herein, we discuss the physiological role of the lymphatic system in volume management and the evidence demonstrating the dysregulation of the lymphatic system in HF. Further, we discuss the opportunity to target the lymphatic system in the management of HF and different potential approaches to accessing the lymphatic system. (J Am Coll Cardiol 2021;78:66–76) © 2021 by the American College of Cardiology Foundation. he circulatory system consists of the cardio- lead to interstitial edema with clinical manifestations T vascular system and the lymphatic system. such as extremity and tissue edema, including pulmo- The cardiovascular system is a closed, high- nary edema. -

Cancer and Lymphatics: Part I
Cancer And Lymphatics: Part I Jassin M. Jouria, MD Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University School of Medicine and has completed his clinical clerkship training in various teaching hospitals throughout New York, including King’s County Hospital Center and Brookdale Medical Center, among others. Dr. Jouria has passed all USMLE medical board exams, and has served as a test prep tutor and instructor for Kaplan. He has developed several medical courses and curricula for a variety of educational institutions. Dr. Jouria has also served on multiple levels in the academic field including faculty member and Department Chair. Dr. Jouria continues to serves as a Subject Matter Expert for several continuing education organizations covering multiple basic medical sciences. He has also developed several continuing medical education courses covering various topics in clinical medicine. Recently, Dr. Jouria has been contracted by the University of Miami/Jackson Memorial Hospital’s Department of Surgery to develop an e-module training series for trauma patient management. Dr. Jouria is currently authoring an academic textbook on Human Anatomy & Physiology. ABSTRACT In the human body, cells receive nutrition and oxygen from lymph, a fluid that is recirculated through the body via an extensive network of vessels. Upon arriving at one of many nodes found within the body, the lymph is filtered to discern healthy cells from those carrying disease or infection. However, cancer can either develop in the lymph nodes around the body, or it can travel there via the lymphatic vessel network. -

Abdominal Examination
PACES- Abdomen Adel Hasanin Ahmed STATION 1 - ABDOMEN STEPS OF EXAMINATION (1) APPROACH THE PATIENT Read the instructions carefully for clues Approach the right hand side of the patient, shake hands, introduce yourself Ask permission to examine him “I am just going to feel your tummy, if it is all right with you” Position patient lying flat on the bed with one pillow supporting the head (but not the shoulder) and arms rested alongside the body Expose the whole abdomen and chest including inguinal regions (breasts can remain covered in ladies) (2) GENERAL INSPECTION STEPS POSSIBLE FINDINGS 1. Scan the patient. Palpate for glandular breast Nutritional status: under/average built or overweight tissue in obese subjects if gynaecomastia is Abnormal Facies: Cushingoid (steroid therapy in renal suspected disease or post renal transplant), bronzing/slate-grey skin (haemochromatosis) Skin marks: Spider naevi (see theoretical notes), scratch marks, purpura, bruises, vitiligo (autoimmune disease) Decreased body hair (in face and chest for males and in axilla and pubic hair for both sexes) Gynaecomastia A-v fistula 2. Examine the eyes: pull down the eyelid. Xanthelasma (primary biliary cirrhosis). Anaemia (pallor) in the conjunctivae at the guttering between the eyeball and the lower lid Check the sclera for icterus Kayser-Fleischer rings (see theoretical notes) 3. Examine the mouth: Central cyanosis (in the under-surface of the tongue) . look at the lips Cheilosis/angular cheilitis (swollen cracked bright-red lips in . Ask the patient to evert his lips (inspect iron, folate, vitamin B12 or B6 deficiency) the inner side of the lips) Abnormal odour of breath (see theoretical notes) . -

M. H. RATZLAFF: the Superficial Lymphatic System of the Cat 151
M. H. RATZLAFF: The Superficial Lymphatic System of the Cat 151 Summary Four examples of severe chylous lymph effusions into serous cavities are reported. In each case there was an associated lymphocytopenia. This resembled and confirmed the findings noted in experimental lymph drainage from cannulated thoracic ducts in which the subject invariably devdops lymphocytopenia as the lymph is permitted to drain. Each of these patients had com munications between the lymph structures and the serous cavities. In two instances actual leakage of the lymphography contrrult material was demonstrated. The performance of repeated thoracenteses and paracenteses in the presenc~ of communications between the lymph structures and serous cavities added to the effect of converting the. situation to one similar to thoracic duct drainage .The progressive immaturity of the lymphocytes which was noted in two patients lead to the problem of differentiating them from malignant cells. The explanation lay in the known progressive immaturity of lymphocytes which appear when lymph drainage persists. Thankful acknowledgement is made for permission to study patients from the services of Drs. H. J. Carroll, ]. Croco, and H. Sporn. The graphs were prepared in the Department of Medical Illustration and Photography, Dowristate Medical Center, Mr. Saturnino Viloapaz, illustrator. References I Beebe, D. S., C. A. Hubay, L. Persky: Thoracic duct 4 Iverson, ]. G.: Phytohemagglutinin rcspon•e of re urctcral shunt: A method for dccrcasingi circulating circulating and nonrecirculating rat lymphocytes. Exp. lymphocytes. Surg. Forum 18 (1967), 541-543 Cell Res. 56 (1969), 219-223 2 Gesner, B. M., J. L. Gowans: The output of lympho 5 Tilney, N. -

The Size of Lymph Nodes in the Neck on Sonograms As a Radiologic Criterion for Metastasis: How Reliable Is It?
AJNR Am J Neuroradiol 19:695–700, April 1998 The Size of Lymph Nodes in the Neck on Sonograms as a Radiologic Criterion for Metastasis: How Reliable Is It? Michiel W. M. van den Brekel, Jonas A. Castelijns, and Gordon B. Snow PURPOSE: A definition of cut-off points for nodal size is essential to determine whether cervical lymph nodes are metastatic or not. Because the currently used size criteria are defined for random populations of patients with head and neck cancer, we set out to study whether these criteria are optimal for patients without palpable metastases in different levels of the neck. We defined optimal size criteria for sonography by calculating the sensitivity and specificity of different size cut-off points. METHODS: We compared the sensitivity and specificity of different size cut-off points as measured on sonograms for various levels in the neck in a series of 117 patients with and 131 patients without palpable neck metastases. RESULTS: A minimum axial diameter of 7 mm for level II and 6 mm for the rest of the neck revealed the optimal compromise between sensitivity and specificity in necks without palpable metastases. For all necks together (with and without palpable metastases), the criteria were 1 to 2 mm larger. CONCLUSION: Our findings indicate that the current sonographic size criteria used for random patient populations are not optimal for necks without palpable metastases, nor can the same cut-off points be used for all levels in the neck. The management of lymph node metastases in the cious lymph nodes may convert both selective neck neck in patients with squamous cell carcinoma of the treatment and a wait-and-see policy to more secure upper air and food passages is a continuing source of comprehensive treatment of all levels of the neck (6). -

Anatomy and Physiology in Relation to Compression of the Upper Limb and Thorax
Clinical REVIEW anatomy and physiology in relation to compression of the upper limb and thorax Colin Carati, Bren Gannon, Neil Piller An understanding of arterial, venous and lymphatic flow in the upper body in normal limbs and those at risk of, or with lymphoedema will greatly improve patient outcomes. However, there is much we do not know in this area, including the effects of compression upon lymphatic flow and drainage. Imaging and measuring capabilities are improving in this respect, but are often expensive and time-consuming. This, coupled with the unknown effects of individual, diurnal and seasonal variances on compression efficacy, means that future research should focus upon ways to monitor the pressure delivered by a garment, and its effects upon the fluids we are trying to control. More is known about the possible This paper will describe the vascular Key words effects of compression on the anatomy of the upper limb and axilla, pathophysiology of lymphoedema when and will outline current understanding of Anatomy used on the lower limbs (Partsch and normal and abnormal lymph drainage. It Physiology Junger, 2006). While some of these will also explain the mechanism of action Lymphatics principles can be applied to guide the use of compression garments and will detail Compression of compression on the upper body, it is the effects of compression on fluid important that the practitioner is movement. knowledgeable about the anatomy and physiology of the upper limb, axilla and Vascular drainage of the upper limb thorax, and of the anatomical and vascular It is helpful to have an understanding of Little evidence exists to support the differences that exist between the upper the vascular drainage of the upper limb, use of compression garments in the and lower limb, so that the effects of these since the lymphatic drainage follows a treatment of lymphoedema, particularly differences can be considered when using similar course (Figure 1). -

Lymph and Lymphatic Vessels
Cardiovascular System LYMPH AND LYMPHATIC VESSELS Venous system Arterial system Large veins Heart (capacitance vessels) Elastic arteries Large (conducting lymphatic vessels) vessels Lymph node Muscular arteries (distributing Lymphatic vessels) system Small veins (capacitance Arteriovenous vessels) anastomosis Lymphatic Sinusoid capillary Arterioles (resistance vessels) Postcapillary Terminal arteriole venule Metarteriole Thoroughfare Capillaries Precapillary sphincter channel (exchange vessels) Copyright © 2010 Pearson Education, Inc. Figure 19.2 Regional Internal jugular vein lymph nodes: Cervical nodes Entrance of right lymphatic duct into vein Entrance of thoracic duct into vein Axillary nodes Thoracic duct Cisterna chyli Aorta Inguinal nodes Lymphatic collecting vessels Drained by the right lymphatic duct Drained by the thoracic duct (a) General distribution of lymphatic collecting vessels and regional lymph nodes. Figure 20.2a Lymphatic System Outflow of fluid slightly exceeds return Consists of three parts 1. A network of lymphatic vessels carrying lymph 1. Transports fluid back to CV system 2. Lymph nodes 1. Filter the fluid within the vessels 3. Lymphoid organs 1. Participate in disease prevention Lymphatic System Functions 1. Returns interstitial fluid and leaked plasma proteins back to the blood 2. Disease surveillance 3. Lipid transport from intestine via lacteals Venous system Arterial system Heart Lymphatic system: Lymph duct Lymph trunk Lymph node Lymphatic collecting vessels, with valves Tissue fluid Blood Lymphatic capillaries Tissue cell capillary Blood Lymphatic capillaries capillaries (a) Structural relationship between a capillary bed of the blood vascular system and lymphatic capillaries. Filaments anchored to connective tissue Endothelial cell Flaplike minivalve Fibroblast in loose connective tissue (b) Lymphatic capillaries are blind-ended tubes in which adjacent endothelial cells overlap each other, forming flaplike minivalves. -
Functions of Lymphatic System
Lymphatic system The lymphatic system contains three parts, a network of lymphatic vessels, a fluid inside of the vessels called lymph, and lymph nodes that cleanse the lymph while it passes through. Functions of Lymphatic system: 1. Draining excess interstitial fluid-It is responsible for the removal of interstitial fluid from tissues 2. Transporting dietary lipids-It absorbs and transports fatty acids and fats as chyle from the digestive system 3. Carrying out immune response- It transports white blood cells to and from the lymph nodes into the bones. The lymph transports antigen-presenting cells, such as dendritic cells, to the lymph nodes where an immune response is stimulated. 4. The lymphatic system returns fluids that have leaked from the blood (vascular system) back to the blood. Without it, our cardiovascular and immune systems would begin to shut down. FLOW OF LYMPH Lymphatic Capillaries Lymphatic capillaries merge together into larger lymphatic vessels to carry lymph through the body. The structure of lymphatic vessels closely resembles that of veins: they both have thin walls and carrying fluids under low pressure. Lymph is transported through lymphatic vessels by the skeletal muscle pump— contractions of skeletal muscles constrict the vessels to push the fluid forward. Check valves prevent the fluid from flowing back toward the lymphatic capillaries. The sequence of fluid flow is blood capillaries (blood) interstitial spaces (interstitial fluid) lymphatic capillaries (lymph) lymphatic vessels (lymph) lymphatic ducts (lymph) junction of the internal jugular and subclavian veins (blood). The interstitial fluid picked up by lymphatic capillaries is known as lymph. Lymph very closely resembles the plasma found in the veins: it is a mixture of about 90% water and 10% solutes such as proteins, cellular waste products, dissolved gases, and hormones. -

Lymphatic System Urls
Lymphatic System URLs Human Anatomy & Physiology 16 http://www.howstuffworks.com/immune-system.htm http://www.thebody.com/step/immune.html http://www.emc.maricopa.edu/faculty/farabee/BIOBK/ BioBookIMMUN.html & http://www.cayuga-cc.edu/about/facultypages/greer/ r http://www.acm.uiuc.edu/sigbio/project/updated- lymphatic/lymph1.html http://www.pblsh.com/Healthworks/lymphart.html Karen Webb Smith Unit Fou Introduction A. The lymphatic system is closely associated with the cardiovascular system and is comprised of a network of vessels that circulate body fluids. B. Lymphatic vessels transport excess fluid away from interstitial spaces between cells in most tissues & return it to the bloodstream. C. Lymphatic vessels called lacteals (located in the in the lining of the smallsmall intestine) absorb fats resulting from digestion, & then transport fats to the circulatory system. D. The organs of the lymphatic system help defend Lymphatic vessels against disease. transporting fluid from interstitial spaces to the bloodstream Lymphatic Pathways A. Lymphatic pathways start as lymphatic capillaries that merge to form larger vessels that empty into the circulatory system. (This is key to understanding this chapter.) B. Lymphatic Capillaries *are microscopic, close-ended tubes that extend into interstitial spaces forming networks that parallel the networks of the blood capillaries *walls consist of single layer squamous epithelial cells which enables interstitial fluid to enter the lymphatic capillaries *lymph – the fluid inside a lymph capillary C. Lymphatic Vessels *walls of lymphatic vessels are thinner than walls of veins * have semilunar valves to prevent backflow of lymph *lymph nodes – specialized lymph organs that are composed of a mass of lymphoid tissue located along the course of a lymphatic vessel D.