Flying Blind
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Epidemiology of COVID-19 in Canada in 2020: the Pre-Vaccine Era February 2021
The Epidemiology of COVID-19 in Canada in 2020: The Pre-Vaccine Era February 2021 An RSC Policy Briefing The Epidemiology of COVID-19 in Canada in 2020: The Pre-Vaccine Era An RSC Policy Briefing Authors Wendy Sligl (Chair) University of Alberta David Waldner University of Alberta Jennie Johnstone University of Toronto Robyn Harrison University of Alberta Duncan Webster Dalhousie University Lynora Saxinger University of Alberta Peer Review Monitor Tom Marrie, FRSC Dalhousie University Peer Reviewers Nick Daneman University of Toronto Rob Fowler University of Toronto Srinivas Murthy The University of British Columbia David Patrick The University of British Columbia Dan Reid Dalhousie University Robert Strang Chief Medical Officer of Health, Nova Scotia Suggested citation for Policy Briefing Report: Waldner D, Harrison R, Johnstone J, Saxinger L, Webster D, Sligl W. The Epidemiology of COVID-19 in Canada in 2020: The Pre-Vaccine Era. Royal Society of Canada. 2021 Cover Art Christine De Vuono, For Your Own Good, (2020) Over the course of the pandemic, those in long term care facilities have been hit hardest with the impact of COVID-19 outbreaks. The response has been to lock down care homes and ban visitors, volunteers and even care packages, as attempts to stop the virus from entering the facility. This had the unintended, but very real consequence of isolating our most vulnerable from those who care for and love them. “For Your Own Good”, made of 100 carved figures from identical bars of soap, then placed in mason jars, which in turn are placed on shelves, allow us to look in on the miniature elderly figures, who look out at us. -

Summary of National Advisory Committee on Immunization (Naci) Updates of July 2, 2021
SUMMARY OF NATIONAL ADVISORY COMMITTEE ON IMMUNIZATION (NACI) UPDATES OF JULY 2, 2021 MRNA COVID-19 VACCINES AND MYOCARDITIS On July 2, 2021, the Public Health Agency of Canada released updated advice from the National Advisory Committee on Immunization (NACI) on the use of mRNA COVID-19 vaccines. These recommendations are based on current scientific evidence and NACI's expert opinion. On June 30, 2021, Health Canada updated the product monographs, the documents that provide information for health care providers on the use of the vaccines, for the mRNA COVID-19 vaccines (Pfizer-BioNTech, Moderna) to include very rare reports of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the tissue surrounding the heart) following vaccination. In light of these changes, NACI is providing updated advice on second doses for individuals who experienced myocarditis and/or pericarditis after receiving a first dose of an mRNA vaccine. NACI continues to strongly recommend that a complete series with an mRNA vaccine should be offered to all eligible individuals without contraindications, including those 12 years of age and older. The Pfizer-BioNTech vaccine is approved for use in people 12 years and over and the Moderna vaccine is approved for use in people 18 years of age and over. NACI is now also recommending the following: Informed consent for people receiving an mRNA vaccine should include a discussion about the very rare risk of myocarditis and/or pericarditis following immunization. As a precaution, NACI recommends that individuals who experienced myocarditis and/or pericarditis after a first dose of an mRNA vaccine should wait to get their second dose until more information is available. -
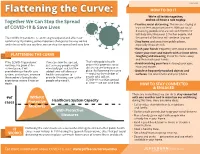
Flattening the Curve: 3/9/2020 We’Re All in This Together, Together We Can Stop the Spread and We All Have a Role to Play
3/23/2020 HOW TO DO IT Flattening the Curve: 3/9/2020 We’re all in this together, Together We Can Stop the Spread and we all have a role to play. • Practice social distancing. This means staying at of COVID-19 & Save Lives least six feet away from others. Without social distancing, people who are sick with COVID-19 will likely infect between 2-3 other people, and The COVID-19 pandemic is continuing to expand and affect our the spread of the virus will continue to grow. community. By making some important changes to the way we live • Stay home and away from public places, and interact with one another, we can stop the spread and save lives. especially if you are sick. • Wash your hands frequently with soap and water. • Cover your nose and mouth with a tissue when FLATTENING THE CURVE coughing and sneezing, throw the tissue away and then wash your hands. If the COVID-19 pandemic If we can slow the spread, That’s why public health orders that promote social • Avoid touching your face including your eyes, continues to grow at the just as many people might nose and mouth. current pace, it will eventually get sick, but the distancing are being put in overwhelm our health care added time will allow our place. By flattening the curve • Disinfect frequently touched objects and system, and in-turn, increase health care system to — reducing the number of surfaces, like door knobs and your phone. the number of people who provide lifesaving care to the people who will get experience severe illness or people who need it. -

Atlantic Agriculture
FOR ALUMNI AND FRIENDS OF DALHOUSIE’S FACULTY OF AGRICULTURE SPRING 2021 Atlantic agriculture In memory Passing of Jim Goit In June 2020, campus was saddened with the sudden passing The Agricultural Campus and the Alumni Association of Jim Goit, former executive director, Development & External acknowledge the passing of the following alumni. We extend Relations. Jim had a long and lustrous 35-year career with the our deepest sympathy to family, friends and classmates. Province of NS, 11 of which were spent at NSAC (and the Leonard D’Eon 1940 Faculty of Agriculture). Jim’s impact on campus was Arnold Blenkhorn 1941 monumental – he developed NSAC’s first website, created Clara Galway 1944 an alumni and fundraising program and built and maintained Thomas MacNaughton 1946 many critical relationships. For his significant contributions, George Leonard 1947 Jim was awarded an honourary Barley Ring in 2012. Gerald Friars 1948 James Borden 1950 Jim retired in February 2012 and was truly living his best life. Harry Stewart 1951 On top of enjoying the extra time with his wife, Barb, their sons Stephen Cook 1954 and four grandchildren, he became highly involved in the Truro Gerald Foote 1956 Rotary Club and taught ski lessons in the winter. In retirement, Albert Smith 1957 Jim also enjoyed cooking, travelling, yard work and cycling. George Mauger 1960 Phillip Harrison 1960 In honour of Jim’s contributions to campus and the Alumni Barbara Martin 1962 Association, a bench was installed in front of Cumming Peter Dekker 1964 Hall in late November. Wayne Bhola Neil Murphy 1964 (Class of ’74) kindly constructed the Weldon Smith 1973 beautiful bench in Jim’s memory. -

The Halifax Region Tourism Opening
The Halifax Region Tourism Opening 2020 Plan Prepared for Discover Halifax Halifax Regional Municipality Prepared by FINAL REPORT June 11, 2020 Prepared for Discover Halifax Halifax Regional Municipality Prepared by Fathom Studio 1 Starr Lane Dartmouth, NS 902 461 2525 fathomstudio.ca Release R1—11 June 2020 Contents 01 Protecting People; Our Two Imperatives ......................................... 1 1.1 The Tourism Imperative & Objectives of this Plan ..................................................2 02 Introduction ......................................... 5 2.1 A Pre-Covid Snapshot of Tourism in NS ...................................................................5 2.2 The Provincial Reopening Strategy .7 2.3 A Proposal for the Easing of Tourism Restrictions ...............................................8 03 Strategy for keeping our Destination Safe ......................................................13 3.1 Travel Between Safe Markets .........14 3.2 Safe Spaces ...........................................22 3.3 Communication to promote safe travel & public health goals ..............32 3.4 Responsive Design to Adapt to Changing Epidemiology......................36 04 Site Specific Actions .......................39 4.1 Halifax & Lunenburg Waterfronts .43 4.2 Citadel Hill National Historic Site ...51 4.3 Nova Scotia Provincial Parks ...........55 4.4 Halifax Regional Municipality Parks, Trails, & Gardens ....................................57 4.5 Downtown Halifax / Dartmouth ......61 4.6 Halifax Shopping Centre ....................64 -
Youth Group Performs 'Lion King'
PRSRT STD US POSTAGE PAID OVERTON, NV PERMIT NO. 11 Your Hometown Newspaper Since 1987 Wednesday, June 23, 2021 www.mvprogress.com VVWD Board Youth group performs ‘Lion King’ approves projects By BOBBIE GREEN to improve system The Progress weak points The Virgin Valley Theater Group (VVTG) held the first ses- By VERNON ROBISON sion of its Youth Summer Theatre The Progress Camp last week for high school and middle school participants. The Virgin Valley Water Dis- A week of rigorous rehearsals trict (VVWD) Board of Directors for the young cast yielded two got the ball rolling last week on impressive performances of The a number of projects that will Lion King on Saturday, June 19. proactively address aging infra- The Youth Summer Theatre structure and weak spots in the Camp was supposed to have VVWD distribution system. gotten off the ground last year. At a meeting held on Tuesday, It was the brainchild of Beaver June 15, the board approved more Dam High School Drama teacher than $250,000 for design and en- Wende Wolfe-Killinger, who also gineering work on three different serves on the board of VVTG. projects at various points in the She has organized and led per- system. forming arts camps in other states Perhaps most pressing was a where she has lived and wanted BOBBIE GREEN / The Progress proposal to award engineering The cast of the VVTG Summer Youth Camp takes a final curtain call following their first performance of The services on a project to replace See Theatre on page 6A Lion King on Saturday afternoon. -
Pandemic.Pdf.Pdf
1 PANDEMICS: Past, Present, Future Published in 2021 by the Mahatma Gandhi Institute of Education for Peace and Challenges & Opportunities Sustainable Development, 35 Ferozshah Road, New Delhi 110001, India © UNESCO MGIEP This publication is available in Open Access under the Attribution-ShareAlike Coordinating Lead Authors: 3.0 IGO (CC-BY-SA 3.0 IGO) license (http://creativecommons.org/licenses/ ANANTHA KUMAR DURAIAPPAH by-sa/3.0/ igo/). By using the content of this publication, the users accept to be Director, UNESCO MGIEP bound by the terms of use of the UNESCO Open Access Repository (http:// www.unesco.org/openaccess/terms-use-ccbysa-en). KRITI SINGH Research Officer, UNESCO MGIEP The designations employed and the presentation of material throughout this publication do not imply the expression of any opinion whatsoever on the part of UNESCO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The ideas and opinions expressed in this publication are those of the authors; they Lead Authors: NANDINI CHATTERJEE SINGH are not necessarily those of UNESCO and do not commit the Organization. Senior Programme Officer, UNESCO MGIEP The publication can be cited as: Duraiappah, A. K., Singh, K., Mochizuki, Y. YOKO MOCHIZUKI (Eds.) (2021). Pandemics: Past, Present and Future Challenges and Opportunities. Head of Policy, UNESCO MGIEP New Delhi. UNESCO MGIEP. SHAHID JAMEEL Coordinating Lead Authors: Director, Trivedi School of Biosciences, Ashoka University Anantha Kumar Duraiappah, Director, UNESCO MGIEP Kriti Singh, Research Officer, UNESCO MGIEP Lead Authors: Nandini Chatterjee Singh, Senior Programme Officer, UNESCO MGIEP Contributing Authors: CHARLES PERRINGS Yoko Mochizuki, Head of Policy, UNESCO MGIEP Global Institute of Sustainability, Arizona State University Shahid Jameel, Director, Trivedi School of Biosciences, Ashoka University W. -

Coronavirus Fact Sheet
CORONAVIRUS FACT SHEET The Assembly of First Nations (AFN) is providing this overview of the coronavirus, and information on resources in your region. As the situation is evolving rapidly, please visit the Public Health Agency of Canada and Indigenous Services Canada for the most updated information. Canada’s Chief Public Health Officer, Dr Theresa Tam, has assessed the public health risk of COVID-19 within Canada to be low. • Coronaviruses in general are part of a large family of viruses which may cause illness in people and in animals. Human coronaviruses are common and are typically associated with mild illnesses, like the common cold. • Coronavirus Disease 2019 (COVID-19) is a new disease that has not been previously identified in humans. • Currently there is NO vaccine to protect against 2019 novel coronavirus infection. • Those who are infected with COVID-19 may have little to no symptoms. You may not know you • The flu vaccine doesnot protect against have symptoms of COVID-19 because they are coronaviruses. similar to a cold or flu. • For now, there is no specific treatment. Most o Symptoms may take up to 14 days to appear people with the common coronavirus illness after exposure to COVID-19. This is the lon- will recover on their own and your health care gest known infectious period for this disease. provider may recommend steps you can take to relieve symptoms. o Symptoms have included fever, cough, difficulty breathing, pneumonia in both lungs. • Common prevention measures for viruses, such as the COVID-19 and influenza, include: • Coronavirus infections are diagnosed by a health care provider based on symptoms and confirmed o Regular hand washing with soap and warm through laboratory tests. -

Covid-19: How Doctors and Healthcare Systems Are Tackling Coronavirus
BMJ 2020;368:m1090 doi: 10.1136/bmj.m1090 (Published 18 March 2020) Page 1 of 5 Feature BMJ: first published as 10.1136/bmj.m1090 on 18 March 2020. Downloaded from FEATURE GLOBAL HEALTH Covid-19: how doctors and healthcare systems are tackling coronavirus worldwide As coronavirus continues to spread, doctors and healthcare systems are facing a multitude of challenges at all stages of the pandemic Janice Hopkins Tanne 1, Erika Hayasaki 2, Mark Zastrow 3, Priyanka Pulla 4, Paul Smith 5, Acer Garcia Rada 6 1New York; 2Boston; 3Seoul; 4Bangalore; 5Sydney; 6Madrid United States least one site already open in the New York City suburb of New Rochelle, handling around 250 people a day. The United States declared a national emergency on 13 March The American Medical Association, which represents about as covid-19 spread to 49 of the country’s 50 states. half of US doctors, called the emergency declaration “necessary http://www.bmj.com/ President Donald Trump announced $50bn (£42.1bn; €45.6bn) to help ensure that America’s health system has sufficient to help combat the virus, as well as powers to waive laws and resources.” Meanwhile, some doctors complained that they did restrictions to make care more available, such as through not have test kits and were short of protective equipment. Other telehealth and allowing doctors to practise in states they are not physicians said that access to Medicaid, insurance for poor licensed in. patients, should be improved and sped up. The president—who has tested negative for covid-19 after At a 15 March press conference Anthony Fauci, head of the contact with an infected Brazilian official—said that many more National Institute of Allergy and Infectious Diseases, told the on 30 April 2020 by guest. -

Received by NSD/FARA Registration Unit 02/16/2021 11:18:01 AM
Received by NSD/FARA Registration Unit 02/16/2021 11:18:01 AM 02/12/21 Friday This material is distributed by Ghebi LLC on behalf of Federal State Unitary Enterprise Rossiya Segodnya International Information Agency, and additional information is on file with the Department of Justice, Washington, District of Columbia. Lincoln Project Faces Exodus of Advisers Amid Sexual Harassment Coverup Scandal by Morgan Artvukhina Donald Trump was a political outsider in the 2016 US presidential election, and many Republicans refused to accept him as one of their own, dubbing themselves "never-Trump" Republicans. When he sought re-election in 2020, the group rallied in support of his Democratic challenger, now the US president, Joe Biden. An increasing number of senior figures in the never-Trump political action committee The Lincoln Project (TLP) have announced they are leaving, with three people saying Friday they were calling it quits in the wake of a sexual assault scandal involving co-founder John Weaver. "I've always been transparent about all my affiliations, as I am now: I told TLP leadership yesterday that I'm stepping down as an unpaid adviser as they sort this out and decide their future direction and organization," Tom Nichols, a “never-Trump” Republican who supported the group’s effort to rally conservative support for US President Joe Biden in the 2020 election, tweeted on Friday afternoon. Nichols was joined by another adviser, Kurt Bardella and by Navvera Hag, who hosted the PAC’s online show “The Lincoln Report.” Late on Friday, Lincoln Project co-founder Steve Schmidt reportedly announced his resignation following accusations from PAC employees that he handled the harassment scandal poorly, according to the Daily Beast. -

WHO COVID-19 Database Search Strategy (Updated 26 May 2021)
Search purpose: Systematic search of the COVID-19 literature performed Monday through Friday for the WHO Database. Search strategy as of 26 May 2021. Searches performed by Tomas Allen, Kavita Kothari, and Martha Knuth. Use following commands to pull daily new entries: Entry_date:( [20210101 TO 20210120]) Entry_date:( 20210105) Duplicates: Duplicates are found in EndNote and Distillr using the Wichor method. Further screening is done by expert reviewers but some duplicates may still be in the database. Daily Search Strategy: Database Daily Search Strategy Medline (coronavir* OR corona virus* OR corona pandemic* OR betacoronavir* OR covid19 OR covid OR (Ovid) nCoV OR novel CoV OR CoV 2 OR CoV2 OR sarscov2 OR sars2 OR 2019nCoV OR wuhan virus* OR 1946- NCOV19 OR solidarity trial OR operation warp speed OR COVAX OR "ACT-Accelerator" OR BNT162b2 OR comirnaty OR "mRNA-1273" OR CoviShield OR AZD1222 OR Sputnik V OR CoronaVac OR "BBIBP-CorV" OR "Ad26.CoV2.S" OR "JNJ-78436735" OR Ad26COVS1 OR VAC31518 OR EpiVacCorona OR Convidicea OR "Ad5-nCoV" OR Covaxin OR CoviVac OR ZF2001 OR "NVX-CoV2373" OR "ZyCoV-D" OR CIGB 66 OR CVnCoV OR "INO-4800" OR "VIR-7831" OR "UB-612" OR BNT162 OR Soberana 1 OR Soberana 2 OR "B.1.1.7" OR "VOC 202012/01" OR "VOC202012/01" OR "VUI 202012/01" OR "VUI202012/01" OR "501Y.V1" OR UK Variant OR Kent Variant OR "VOC 202102/02" OR "VOC202102/02" OR "B.1.351" OR "VOC 202012/02" OR "VOC202012/02" OR "20H/501.V2" OR "20H/501Y.V2" OR "501Y.V2" OR "501.V2" OR South African Variant OR "B.1.1.28.1" OR "B.1.1.28" OR "B.1.1.248" OR -

The Relative Performance of Federal and Non-Federal Countries During the Pandemic
The Forum of Federations, the global network on federalism and multilevel governance, supports better governance through learning among practitioners and experts. Active on six continents, it runs programs in over 20 countries including established federations, as well as countries transitioning to devolved and decentralized governance options. The Forum publishes a range of information and educational materials. It is supported by the following partner countries: Australia, Brazil, Canada, Ethiopia, Germany, India, Mexico, Nigeria, Pakistan and Switzerland. The Relative Performance of Federal and Non-federal Countries During the Pandemic David Cameron © Forum of Federations, 2021 ISSN: 1922-558X (online ISSN 1922-5598) Occasional Paper Series Number 50 The Relative Performance of Federal and Non-federal Countries During the Pandemic By David Cameron For more information about the Forum of Federations and its publications, please visit our website: www.forumfed.org. Forum of Federations 75 Albert Street, Suite 411 Ottawa, Ontario (Canada) K1P 5E7 Tel: (613) 244-3360 Fax: (613) 244-3372 [email protected] Suggested citation for Forum of Federations' publications: Rupak Chattopadhyay, Handbook of Federal Countries 2009 (Forum of Federations, Oxford Press, 2009) The Relative Performance of Federal and Non-federal Countries During the Pandemic 3 Introduction The story of COVID-19 can be divided into two broad, overlapping phases. The first phase covers the period from the initial outbreak of the pandemic at the beginning of 2020 until about January 2021. That is the time when – without a preventive vaccine – the world struggled to contain its spread and to provide health care to those who fell ill. The second phase of the story starts in early 2021, when effective vaccines began to be manufactured and administered to national populations.