The Effect of Iron Status During Pregnancy on Hearing Functions in the Newborn
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Archdiocese of Los Angeles Catholic Directory 2020-2021
ARCHDIOCESE OF LOS ANGELES CATHOLIC DIRECTORY 2020-2021 Mission Basilica San Buenaventura, Ventura See inside front cover 01-FRONT_COVER.indd 1 9/16/2020 3:47:17 PM Los Angeles Archdiocesan Catholic Directory Archdiocese of Los Angeles 3424 Wilshire Boulevard Los Angeles, CA 90010-2241 2020-21 Order your copies of the new 2020-2021 Archdiocese of Los Angeles Catholic Directory. The print edition of the award-winning Directory celebrates Mission San Buenaventura named by Pope Francis as the first basilica in the Archdiocese. This spiral-bound, 272-page Directory includes Sept. 1, 2020 assignments – along with photos of the new priests and deacons serving the largest Archdiocese in the United States! The price of the 2020-21 edition is $30.00 (shipping included). Please return your order with payment to assure processing. (As always, advertisers receive one complimentary copy, so consider advertising in next year’s edition.) Directories are scheduled to begin being mailed in October. _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Please return this portion with your payment REG Archdiocese of Los Angeles 2020-2021 LOS ANGELES CATHOLIC DIRECTORY ORDER FORM YES, send the print version of the 2020-21 ARCHDIOCESE OF LOS ANGELES CATHOLIC DIRECTORY at the flat rate of $30.00 each. Please return your order with payment to assure processing. -

L'o S S E Rvator E Romano
Price € 1,00. Back issues € 2,00 L’O S S E RVATOR E ROMANO WEEKLY EDITION IN ENGLISH Unicuique suum Non praevalebunt Fifty-third year, number 35 (2.661) Vatican City Friday, 28 August 2020 At the General Audience the Pope continues his catechesis on the crises aggravated by the pandemic Inequality fruit of a ‘sick economy’ See page 3 Children from Harare, Zimbabwe, where the population is affected by severe drought, help carry buckets of water (Epa) Audiences to resume As of Wednesday, 2 September, To weather the storm: all together the General Audiences with the participation of the faithful will take place in the San Damaso ANDREA MONDA we cannot go on thinking of the gift of hope that comes from Courtyard of the Apostolic Palace, ourselves, but only together can we Christ. It is He who helps us navig- beginning at 9.30 am. Everyone remembers what hap- do this.... The storm exposes our ate the tumultuous waters of sick- Attendance is open to all pened five months ago in the after- vulnerability and uncovers those ness, death and injustice, which do without the need of tickets. noon of 27 March, when the shad- false and superfluous certainties not have the last word over our final ows of sunset were gathering togeth- around which we have constructed destination”. The risk is not only of er with the rain filled clouds over our daily schedules, our projects, losing hope but also reason, and of Saint Peter’s Square, and the Pope our habits and priorities”. letting fear and the struggle for sur- slowly climbed the steps of the par- The message was strong and vival prevail over the sense of solid- vis to raise his voice and pray to clear: we are not self-sufficient; on arity. -

Sons of Don Bosco Successors of The
SONS OF DON BOSCO SUCCESSORS OF THE APOSTLES SALESIAN BISHOPS 1884 to 2001 by Charles N. Bransom, Jr. INTRODUCTION he study of apostolic succession and episcopal lineages has long fascinated students of church history. It was not until the middle T of the twentieth century, however, that a systematic attempt was made to trace and catalogue the consecrations of bishops on a world-wide basis. A small group of researchers has catalogued the consecrations of tens of thou sands of bishops dating back many centuries. The fruits of their labors--labors that are on going-have resulted in a database, which can trace the episcopal lineage of any living bishop and the vast majority of deceased bishops. In 1984, I began a project on the episcopal ordinations of bishops of re ligious orders and congregations. One fruit of that work was a study of the ordi nations of Salesian bishops, Les Eveques Salesiens. The present work updates, corrects and expands the 1984 study. In 1984, the episcopal ordinations of 130 bishops were presented. This study contains the details of 196 bishops. The text has been expanded to include the episcopal lineages of the bishops. Of the 196 bishops in this study, 183 trace their orders to Scipione Re biba, who was appointed Auxiliary Bishop ofChieti in 1541. The Rebiban suc cession is the major episcopal line in the contemporary Catholic episcopate. More than 91 % of the more than 4,500 bishops alive today trace their orders 54 Journal of Salesian Studies back to Rebiba Why so many bishops should trace their lineages to this one bishop can be explained, in great part, by the intense sacramental activity of Pope Benedict XIII, who consecrated 139 bishops during his pontificate, many of them cardinals, nuncios and bishops of important sees who in tum conse crated many other bishops. -

Catiline in Fiesole and Florence: the After-Life of a Roman Conspirator
Catiline in Fiesole and Florence: The After-life of a Roman Conspirator PATRICIA J. OSMOND The story of Catiline, the Roman noble who plotted to overthrow the Roman Republic in 63 B.C., occupies a significant place in Florentine historiography and political thought of the later Middle Ages and early Renaissance. Starting with the Chronica de origine civitatis (ca. 1228), this article traces the sources of the medieval account back to the ancient epitomes and investigates its relation to Sallust's Bellum Catilinae. It then describes the two branches or traditions of the story that developed in the course of the thirteenth and fourteenth centuries: (1) the classical or civic, which centered on the figure of Catiline-the- villain, rebel and enemy of Rome (and of Rome's daughter-city Florence) and (2) the feudal or chivalric, which recounted the legendary adventures of Catiline-the-knight, pro- tector of Fiesole, the rival of Florence. In the final sections of the article, attention focuses on the success of the classical version of the story, linked to Guelf ambienti and, in turn, to the growth of a conservative republican ideology. While the celebration of Roman civic virtues, summed up in Cicero's defense of the res publica against the rebel Catiline, legiti- mated and ennobled the claims of the rising merchant and banking families, the vilifica- tion of Catiline as public enemy provided effective propaganda against new challenges from lower-class movements. Continuously present in the elaboration of Florentine "civic humanism," Sallust's story of Catiline supplies, in fact, an important connection between Guelf patriotism and the classicizing republicanism of the Quattrocento. -

Ricerche Storiche Salesiane Storiche Ricerche
52-RSScop_51-RSScop.qxd 27/11/15 07:34 Pagina 1 ISSN 0393-3830 ISTITUTO STORICO SALESIANO FONTI RICERCHE STORICHE Serie prima: Giovanni Bosco. Scritti editi e inediti SALESIANE 1. Giovanni BOSCO, Costituzioni della Società di S. Francesco di Sales [1858] - 1875. RIVISTA SEMESTRALE DI STORIA RELIGIOSA E CIVILE Testi critici a cura di Francesco Motto (= ISS, Fonti, Serie prima, 1). LAS-Roma, 1981, 272 p.(in folio) + 8 tav. € 15,49* 2. Giovanni BOSCO, Costituzioni per l’Istituto delle Figlie di Maria Ausiliatrice (1872-1885). Testi critici a cura di Cecilia Romero (= ISS, Fonti, Serie prima, 2). LAS-Roma, 1982, 358 p. + 8 tav. f.t. € 10,33 4. Giovanni BOSCO, Memorie dell’Oratorio di S. Francesco di Sales dal 1815 al 1855. In troduzione, note e testo critico a cura di Antonio Ferreira Da Silva (= ISS, Fonti, Serie prima, 4). LAS-Roma, 1991, 255 p. € 10,33 52 ANNO XXVII - N. 2 LUGLIO-DICEMBRE 2008 5. Giovanni BOSCO, Memorie dell’Oratorio di S. Francesco di Sales dal 1815 al 1855. Intro duzione e note a cura di Antonio Ferreira Da Silva (= ISS, Fonti, Serie prima, 5). LAS-Roma, 1991, 236 p. [edizione divulgativa] € 10,33 RICERCHE STORICHE SALESIANE RICERCHE STORICHE 6. Giovanni BOSCO, Epistolario. Vol. I (1835-1863) lett. 1-726. Introduzione, note critiche e storiche a cura di Francesco Motto (= ISS, Fonti, Serie prima, 6). LAS-Roma, 1991, 718 p. € 25,82* 8. Giovanni BOSCO, Epistolario. Vol. II (1864-1868) lett. 727-1263. Introduzione, note critiche e stori che a cura di Francesco Motto (= ISS, Fonti, Serie prima, 8). -
Ricerche Storiche Salesiane Rivista Semestrale Di Storia Religiosa E Civile
www50-RSScop_www50-RSScop.qxd 27/11/15 07:30 Pagina 1 2015 - Digital Collections - Biblioteca Don Bosco - Roma - http://digital.biblioteca.unisal.it ISSN 0393-3830 ISTITUTO STORICO SALESIANO FONTI RICERCHE STORICHE Serie prima: Giovanni Bosco. Scritti editi e inediti SALESIANE 1. Giovanni BOSCO, Costituzioni della Società di S. Francesco di Sales [1858] - 1875. RIVISTA SEMESTRALE DI STORIA RELIGIOSA E CIVILE Testi critici a cura di Francesco Motto (= ISS, Fonti, Serie prima, 1). LAS-Roma, 1981, 272 p.(in folio) + 8 tav. € 15,49* 2. Giovanni BOSCO, Costituzioni per l’Istituto delle Figlie di Maria Ausiliatrice (1872-1885). Testi critici a cura di Cecilia Romero (= ISS, Fonti, Serie prima, 2). LAS-Roma, 1982, 358 p. + 8 tav. f.t. € 10,33 4. Giovanni BOSCO, Memorie dell’Oratorio di S. Francesco di Sales dal 1815 al 1855. In troduzione, note e testo critico a cura di Antonio Ferreira Da Silva (= ISS, Fonti, Serie prima, 4). LAS-Roma, 1991, 255 p. € 10,33 50 ANNO XXVI - N. UNICO GENNAIO-DICEMBRE 2007 5. Giovanni BOSCO, Memorie dell’Oratorio di S. Francesco di Sales dal 1815 al 1855. Intro duzione e note a cura di Antonio Ferreira Da Silva (= ISS, Fonti, Serie prima, 5). LAS-Roma, 1991, 236 p. [edizione divulgativa] € 10,33 RICERCHE STORICHE SALESIANE RICERCHE STORICHE 6. Giovanni BOSCO, Epistolario. Vol. I (1835-1863) lett. 1-726. Introduzione, note critiche e storiche a cura di Francesco Motto (= ISS, Fonti, Serie prima, 6). LAS-Roma, 1991, 718 p. € 25,82* 8. Giovanni BOSCO, Epistolario. Vol. II (1864-1868) lett. 727-1263. Introduzione, note critiche e stori che a cura di Francesco Motto (= ISS, Fonti, Serie prima, 8). -
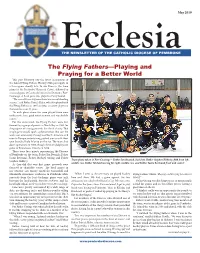
The Flying Fathers—Playing and Praying for a Better World
May 2019 The Flying Fathers—Playing and Praying for a Better World This past February saw the latest incarnation of the famed Flying Fathers Hockey Club participate in a three-game charity tour. In our Diocese, the team played at the Pembroke Memorial Centre, followed by a second game at Centre de Loisirs des Draveurs, Fort- Coulonge. A third game was played in Parry Sound. “The recent three-day mini-tour was an outstanding success,” said Father Patrick Blake, who first played with the Flying Fathers in 1965 and was an active player on the team for over 40 years. “In each place where the team played there were enthusiastic fans, good entertainment and worthwhile c au s e s .” For the uninitiated, the Flying Fathers were first formed by a group of priests in North Bay in 1964 for the purpose of raising proceeds for a local charity. That single game would spark a phenomenon that saw the team tour extensively throughout North America, and even to Europe, entertaining packed arenas with their own brand of holy hilarity on the ice. The team shut down operations in 2009, though the team did play one game in Ennismore, Ontario in 2018. There were four priests representing the Diocese of Pembroke on the team; Father Jim Beanish, Father Justin Bertrand, Father Michael Goring and Father Stephen Helferty. Team photo taken in Fort Coulonge – Father Jim Beanish, back left, Father Stephen Helferty, ftfif h from left, As they did that very first game, proceeds were middle row, Father Michael Goring far right, middle row, and Father Justin Bertrand front and centre! donated to charitable causes. -

1 Riccardo Burigana
Riccardo Burigana RICCARDO BURIGANA (Firenze, 1964) via Italo Svevo 49 30121 Mogliano Veneto (Tv) email: [email protected] telefono +393483821778 Docente di Storia ecumenica della Chiesa presso l’Istituto di Studi Ecumenici dal 2004, docente invitato di ecumenismo presso la Facoltà Teologica dell’Italia Centrale di Firenze, visiting professor all’Università Cattolica del Pernambuco di Recife, dal 2008 direttore del Centro Studi per l’Ecumenismo in Italia; dal 2010 direttore scientifico della rivista «Colloquia Mediterranea» della Fondazione Giovanni Paolo II e collaboratore de «L’Osservatore Romano»; dal 2016 membro della Commissione Internazionale per il Dialogo dell’Ordine Francescano, curatore del progetto per una storia dell’Eparchia di Lungro (1919-2019) e co-coordinatore del progetto internazionale di ricerca Eredità della Riforma; fondatore e direttore della newsletter «Veritas in caritate. Informazioni dall’Ecumenismo in Italia» e co-direttore della newsletter «Ecumenismo Quotidiano»; presidente dell’Associazione Italiana Docenti di Ecumenismo. Ha pubblicato numerosi saggi sulla storia della Riforma, del Concilio Vaticano II e del movimento ecumenico, tra i più recenti, Storia del concilio Vaticano II, (Torino, Lindau, 2012), Una straordinaria avventura. Storia del movimento ecumenico in Italia (Bologna, EDB, 2013), Un cuore solo. Papa Francesco e l’unità della Chiesa (Milano, Edizioni Terra Santa, 2014), Fratelli in cammino. Storia della dichiarazione Nostra Aetate (Milano, Edizioni Terra Santa, 2015) e La pace di Assisi. 27 ottobre 1986 il dialogo tra le religioni trent’anni dopo (Milano, Edizioni Terra Santa, 2016). TITOLI ACCADEMICI 1991 Dottorato in Discipline Storiche presso l'Alta Scuola di Studi Storici dell'Università di San Marino, con la tesi, L’università di Wittenberg tra Lutero e Melantone (1502-1560). -

Decreto N. 21
Decreto n. 21 MINISTERO DELLA DIFESA DIREZIONE GENERALE PER IL PERSONALE MILITARE IL VICE DIRETTORE GENERALE VISTO il decreto legislativo 30 marzo 2001, n. 165 e successive modificazioni, recante norme generali sull’ordinamento del lavoro alle dipendenze delle amministrazioni pubbliche e, in particolare, l’articolo 16, concernente le funzioni dei dirigenti di uffici dirigenziali generali; VISTO il decreto legislativo 8 maggio 2001, n. 215 e successive modificazioni, recante la disciplina della trasformazione progressiva dello strumento militare in professionale; VISTA la legge 23 agosto 2004, n. 226, che ha previsto la sospensione anticipata del servizio obbligatorio di leva e la disciplina dei volontari di truppa in ferma prefissata di un anno (VFP 1) nonché la delega al Governo per il conseguente coordinamento con la normativa di settore; VISTO il decreto del Ministro della difesa 1° settembre 2004, concernente le modalità di reclutamento dei VFP 1 dell’Esercito, della Marina e dell’Aeronautica, emanato ai sensi dell’articolo 6 della citata legge 226/2004; VISTO il decreto dirigenziale della Direzione generale per il personale militare (DGPM) 29 agosto 2008, n 71, pubblicato nella Gazzetta ufficiale 4ª serie speciale - concorsi ed esami n. 70 del 9 settembre 2008, con cui veniva indetto, per l’anno 2009, un bando per il reclutamento di 12.000 VFP 1 nell’Esercito; VISTO il decreto dirigenziale della DGPM 31 luglio 2009, n. 61, che modificava l’articolo 1, comma 1 del citato bando di reclutamento, con particolare riferimento al numero massimo dei VFP 1 da arruolare per il 3° e il 4° blocco di incorporamento per l’anno 2009; TENUTO CONTO che lo Stato maggiore della difesa, con comunicazione n. -

Quotquot Invenire Posset: Inventiones and Historical Memory in Southern Italy, C
Quotquot invenire posset: Inventiones and Historical Memory in Southern Italy, c. 900-1150 by Bridget Kathryn Riley A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Centre for Medieval Studies University of Toronto © Copyright by Bridget Riley 2020 Quotquot invenire posset: Inventiones and Historical Memory in Southern Italy, c. 900-1150 Bridget Riley Doctor of Philosophy Centre for Medieval Studies University of Toronto 2020 Abstract This dissertation examines inventiones, that is narratives of relic discoveries, written in southern Italy between the tenth and twelfth centuries. During this period, communities dealt with sweeping changes brought on by political upheaval, invasion, and ecclesiastical reforms. Several inventiones written concomitantly to these events have received little scholarly attention. This dissertation has two goals: to enhance our understanding of the genre in general and to explore further the local circumstances that prompted their composition and copying. The following four case studies pertain to Christian communities in Naples, Benevento, and Larino, and the abbey of San Vincenzo al Volturno respectively. This dissertation argues that, because of their “inventive” nature, these sources were powerful means of writing and rewriting history and, more often than not, the exercise of historical memory fueled their production. In particular, this dissertation contends that in eleventh-and twelfth-century southern Italy, as communities underwent the transition from Lombard to Norman authorities, the memory of the Lombard lords of the past was utilized in inventiones as a powerful tool to rewrite the identity of a community as it negotiated the changing political and ecclesiastical landscape. Furthermore, this dissertation argues that because of the devotional nature of inventiones, typically composed for use in the liturgy and thus potentially exposed to a large public, the history encoded within these sources ii was made all the more powerful. -

Historia Causae Canonizationis Ioannis Pauli I
With the opening of the Cause for his beatification and canonisation John Paul I (26 August 1978 - 28 September 1978) becomes the sixth pontiff of the twentieth century to be put on the path to sainthood. Among the popes already raised to the honour of the altars for veneration by the universal Church are: Pius X, John XXIII, Paul VI and John Paul II. The Cause of Albino Luciani as Confessor of the faith was opened on the 23 November 2003 and concluded on the 8 November 2017 with the proclamation of his heroic virtues. Currently taking place is a 'Super miro' investigation for an alleged extraordinary healing attributed to the intercession of John Paul I. Should it be recognised the beatification could then take place. According to current norms of canon law the following step would be the recognition of a second 'Super miro' investigation. Only then could the Cause of canonisation proceed. HISTORIA CAUSAE CANONIZATIONIS IOANNIS PAULI I Immediately following the death of John Paul I, on the 28 September 1978, requests for his canonisation began to reach his home diocese from across the world. At the time the Bishop of Belluno-Feltre, Maffeo Ducoli, declared he had: «received a growing number of requests to open the Cause, all of which are now archived at the 'Archivio della Curia’ of Belluno». Requests that came in without any official stand on the part of the diocese. Rather signed petitions sent in by people from local communities throughout different countries, among which Switzerland, France, Canada and the United States. On the 9 June 1990, the Archbishop of Belo Horizonte, Dom Serafim Fernandes de Araújo, presented John Paul II with a request to open the Cause, handing him a petition signed by the entire episcopal Conference of Brazil. -

Chronicle / Crónica / Cronaca
Chronicle / Crónica / Cronaca ACCADEMIA ALFONSIANA Cronaca relativa all’anno accademico 2009-2010 Danielle Gros* 1. Eventi principali 1.1. Inaugurazione dell’anno accademico Il 9 ottobre 2009 è stato inaugurato l’anno accademico. La conce- lebrazione eucaristica, celebrata nella Chiesa di S. Alfonso, è stata presieduta dal Rev.mo Padre Serafino Fiore, Vicario Generale della Congregazione del Santissimo Redentore, che ha tenuto anche l’o- melia (cf. Inaugurazione dell’anno accademico 2009-2010, Roma, Eda- calf, 2009, pp. 5-8). La messa solenne è stata concelebrata anche dal Preside, Prof. Martin McKeever, dal Vicepreside, Prof. Bruno Hidber, dal Rettore della Comunità Redentorista, R. P. Luciano Panella e da numerosi professori e studenti. Al termine della celebrazione, nell’aula magna dell’Accademia si è svolto l’atto inaugurale articolato in due momenti: • il primo, sostanziatosi nella Relazione del Preside sull’anno accade- mico 2008-2009 (cf. ibidem, pp. 9-20), durante il quale sono sta- ti richiamati gli avvenimenti più significativi avvenuti durante lo scorso anno accademico; • il secondo, marcato dalla prolusione Questo è il momento di agi- re. La priorità della Chiesa nella tutela dei minori, tenuta dal Prof. * Segretaria Generale dell’Accademia Alfonsiana. 474 DANIELLE GROS Seán Cannon, Professore dell’Accademia Alfonsiana (cf. ibidem, pp. 21-45). Come ogni anno, l’atto accademico, conclusosi con un rinfresco, è stato occasione per uno scambio di idee tra professori, ufficiali e studenti. Per la prima volta, la Concelebrazione della Santa Messa per l’inizio dell’anno accademico 2009-2010 dei Pontifici Atenei Ro- mani è stata sostituita da una Udienza particolare con il Santo Padre Benedetto XVI, tenutasi giovedì 19 novembre 2009 alle ore 12.00 nell’Aula Paolo VI in Vaticano, alla quale hanno partecipato il Presi- de dell’Accademia, Prof.