Bulletin 07/2009
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

216 Part 218—Railroad Operating Practices
Pt. 217, App. A 49 CFR Ch. II (10–1–12 Edition) APPENDIX A TO PART 217—SCHEDULE OF CIVIL PENALTIES 1 Willful viola- Section Violation tion 217.7 Operating rules: (a) ............................................................................................................................................ $2,500 $5,000 (b) ............................................................................................................................................ $2,000 $5,000 (c) ............................................................................................................................................ $2,500 $5,000 217.9 Operational tests and inspections: (a) Failure to implement a program ........................................................................................ $9,500– $13,000– 12,500 16,000 (b) Railroad and railroad testing officer responsibilities:. (1) Failure to provide instruction, examination, or field training, or failure to con- duct tests in accordance with program ................................................................. 9,500 13,000 (2) Records ............................................................................................................... 7,500 11,000 (c) Record of program; program incomplete .......................................................................... 7,500– 11,000– 12,500 16,000 (d) Records of individual tests and inspections ...................................................................... 7,500 (e) Failure to retain copy of or conduct:. (1)(i) Quarterly -

Operation of Points
9100-000-007 Safeworking Rules and Procedures PUBLIC TRANSPORT AUTHORITY SAFEWORKING RULES AND PROCEDURES 9012 OPERATION OF POINTS 9012 Operation of Points Rev1.00 Date: 01 November 15 Page 1 of 18 9100-000-007 Safeworking Rules and Procedures CONTENTS 1. Purpose ................................................................................................................. 3 2. General .................................................................................................................. 3 3. Setting Points ........................................................................................................ 4 3.1. Indications of Points Setting ......................................................................... 4 3.2. Restoration of Points .................................................................................... 4 4. Movement over Points ........................................................................................... 5 4.1. Rail Traffic .................................................................................................... 5 4.2. Competent Workers ..................................................................................... 5 4.3. Trailing Points .............................................................................................. 5 5. Damaged Points .................................................................................................... 6 6. Failed Electrically Operated Points ....................................................................... 6 -
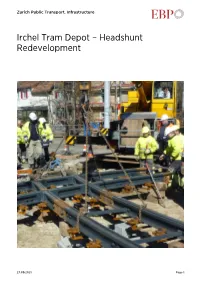
Irchel Tram Depot – Headshunt Redevelopment
Zurich Public Transport, Infrastructure Irchel Tram Depot – Headshunt Redevelopment 27.09.2021 Page 1 Irchel Tram Depot – Headshunt Redevelopment Client Facts Zurich Public Transport, Infrastructure Period 2010 - 2013 Project Country Switzerland Redeveloped headshunt enables Zurich Public Transport (VBZ) to operate its Irchel Tram Depot more efficiently. Difficult and time-consuming shunting tasks are now a thing of the past. Trams with low-floor cars in the middle and trailers (also referred to as “sedan-pony trams”) have been in operation on Line 7 since November 2010. These trams are now to be maintained and housed at the Irchel Tram Depot. The existing headshunt was not long enough to permit the expeditious handling of trams longer than 43 metres. Handling the 45-metre sedan-pony trams on the existing headshunt involved disconnecting the tram cars, shunting them separately into the depot and then reconnecting them – an overly complicated, time consuming and operationally impractical process. In response, Zurich Public Transport (VBZ) initiated an internal process of identifying alternative solutions. These solutions were also expected to take account of the new tram specifications that will apply following Zurich Public Transport’s purchase of a new tram generation (NTG). In October 2010, Zurich Public Transport commissioned EBP to conduct an independent and comprehensive review of the various development proposals it had worked out. The review was also to include an examination of the associated costs and relative merits of the proposed construction measures and their impact on the depot’s immediate vicinity and on railway operation in general. Working in the capacity of a general planner, EBP evaluated the various proposals and used the results of its review to outline the steps that would need to be taken to gain approval for and execute the redevelopment project. -

the Swindon and Cricklade Railway
The Swindon and Cricklade Railway Construction of the Permanent Way Document No: S&CR S PW001 Issue 2 Format: Microsoft Office 2010 August 2016 SCR S PW001 Issue 2 Copy 001 Page 1 of 33 Registered charity No: 1067447 Registered in England: Company No. 3479479 Registered office: Blunsdon Station Registered Office: 29, Bath Road, Swindon SN1 4AS 1 Document Status Record Status Date Issue Prepared by Reviewed by Document owner Issue 17 June 2010 1 D.J.Randall D.Herbert Joint PW Manager Issue 01 Aug 2016 2 D.J.Randall D.Herbert / D Grigsby / S Hudson PW Manager 2 Document Distribution List Position Organisation Copy Issued To: Copy No. (yes/no) P-Way Manager S&CR Yes 1 Deputy PW Manager S&CR Yes 2 Chairman S&CR (Trust) Yes 3 H&S Manager S&CR Yes 4 Office Files S&CR Yes 5 3 Change History Version Change Details 1 to 2 Updates throughout since last release SCR S PW001 Issue 2 Copy 001 Page 2 of 33 Registered charity No: 1067447 Registered in England: Company No. 3479479 Registered office: Blunsdon Station Registered Office: 29, Bath Road, Swindon SN1 4AS Table of Contents 1 Document Status Record ....................................................................................................................................... 2 2 Document Distribution List ................................................................................................................................... 2 3 Change History ..................................................................................................................................................... -

December 2016 Inter City Railway Society Founded 1973
TTRRAA CCKKSS Inter City Railway Society - December 2016 Inter City Railway Society founded 1973 www.intercityrailwaysociety.org Volume 44 No.12 Issue 528 December 2016 The content of the magazine is the copyright of the Society No part of this magazine may be reproduced without prior permission of the copyright holder President: Simon Mutten (01603 715701) Coppercoin, 12 Blofield Corner Rd, Blofield, Norwich, Norfolk NR13 4RT Chairman: Carl Watson - [email protected] Mob (07403 040533) 14, Partridge Gardens, Waterlooville, Hampshire PO8 9XG Treasurer: Peter Britcliffe - [email protected] (01429 234180) 9 Voltigeur Drive, Hart, Hartlepool TS27 3BS Membership Sec: Colin Pottle - [email protected] (01933 272262) 166 Midland Road, Wellingborough, Northants NN8 1NG Mob (07840 401045) Secretary: Stuart Moore - [email protected] (01603 714735) 64 Blofield Corner Rd, Blofield, Norwich, Norfolk NR13 4SA Magazine: Editor: Trevor Roots - [email protected] (01466 760724) Mill of Botary, Cairnie, Huntly, Aberdeenshire AB54 4UD Mob (07765 337700) Sightings: James Holloway - [email protected] (0121 744 2351) 246 Longmore Road, Shirley, Solihull B90 3ES Photo Database: Colin Pottle Website: Trevor Roots - [email protected] contact details as above Events: Sales Stand: Christine Field Trip Co-ordinator: vacant Books: Publications Manager: Carl Watson - [email protected] Publications Team: Trevor -

A Bibliography of the History of Inland Waterways, Railways and Road Transport in the British Isles, 2001
A Bibliography of the History of Inland Waterways, Railways and Road Transport in the British Isles, 2001 This is the seventeenth of these annual bibliographies. annual listing. (Michael Woods is collecting data on Peter Somervail has been one of the regular the ever-growing number of railway-related official contributors from the beginning, submitting details publications.) As regards periodical publications, of historical articles published in Waterways World however, only historical articles are noted; the and of books reviewed there; however, he has now contemporaneous literature is too just too extensive. requested leave to retire. Fortuitously this followed There is also a degree of selection: short items of an offer from Tony Harvey to widen the range of less than a page and articles that are a re-working of waterway periodicals that are systematically searched previously published work are generally omitted. (the first results of this appear below) and to lead the Publication of annual bibliographies was always compilation of the Canal and River Navigations seen as an interim service. As their number increases, section. This is also the last year that John Langford searching through them becomes ever more daunting. is able to provide the main input on Irish publications. Some form of cumulative publication is needed, In thanking these member for their past and future back-dated to cover earlier years. The accumulated support, this is an opportunity to thank also the other data on railway books and pamphlets up to 1995 was regular contributors, several of whom have also been included in Ottley’s Bibliography of British Railway involved since 1985: Alan Jackson, Paul Reynolds, History: second supplement and it is expected that Paul Sowan, Donald Steggles, Richard Storey and there will be a third supplement in due course. -
Collision Between Freight Wagons (For Train 4MP5) and Passenger Train 8622 Moonee Ponds Creek Junction, South Dynon, Victoria
ATSB TRANSPORT SAFETY INVESTIGATION REPORT Rail Occurrence Investigation 2005001 Final Collision Between Freight Wagons (for train 4MP5) and Passenger Train 8622 Moonee Ponds Creek Junction, South Dynon, Victoria 19 January 2005 ATSB TRANSPORT SAFETY INVESTIGATION REPORT RAIL REPORT 2005/001 Final Collision Between Freight Wagons (for Train 4MP5) and Passenger Train 8622 Moonee Ponds Creek Junction, South Dynon 19 January 2005 Released in accordance with section 25 of the Transport Safety Investigation Act 2003 – ii – Published by: Australian Transport Safety Bureau Postal address: PO Box 967, Civic Square ACT 2608 Office location: 15 Mort Street, Canberra City, Australian Capital Territory Telephone: 1800 621 372; from overseas + 61 2 6274 6590 Accident and serious incident notification: 1800 011 034 (24 hours) Facsimile: 02 6274 6474; from overseas + 61 2 6274 6474 E-mail: [email protected] Internet: www.atsb.gov.au © Commonwealth of Australia 2006. This work is copyright. In the interests of enhancing the value of the information contained in this publication you may copy, download, display, print, reproduce and distribute this material in unaltered form (retaining this notice). However, copyright in the material obtained from non- Commonwealth agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you want to use their material you will need to contact them directly. Subject to the provisions of the Copyright Act 1968, you must not make any other use of the material in this publication unless you have the permission of the Australian Transport Safety Bureau. Please direct requests for further information or authorisation to: Commonwealth Copyright Administration Copyright Law Branch Attorney-General’s Department Robert Garran Offices National Circuit BARTON ACT 2600 www.ag.gov.au/cca ISBN and formal report title: see ‘Document retrieval information’ on page vi. -

A Cardiff Capital Region Metro: Impact Study: Metro Interventions Appraisal Report
Report to the Minister for Economy, Science and Transport Merthyr Ebbw Hirwaun Tydfil Rhymney Tredegar Vale Brynmawr Abergavenny Aberdare Treherbert Abertillery Pontypool Bargoed Blackwood Newbridge Abercynon Cwmbran Pontypridd Ystrad Mynach Cross Keys Porth Maesteg Talbot Green Taffs Well Caerphilly Caerleon Pontyclun Cardiff Gate North West Heath Bridgend Cardiff Severn Queen Tunnel Ely Mill Street Newport Junction Porthcawl St Llanwern Chepstow Mellons Culverhouse Cross Pill Cardiff Cardiff Bay Bristol Airport Sports Village Cardiff Central Barry Penarth Porth Teigr A Cardiff Capital Region Metro: Impact Study: Metro Interventions Appraisal Report October 2013 Metro Interventions Appraisal Report FINAL Report | September 2013 Project No: CS/060195 Doc Ref: CS/060195 Rev: Client: Welsh Government Issue Date: September 2013 Metro Interventions Appraisal Report: FINAL Report Name Signature Date Author Michelle North-Jones 30/09/2013 Checker David McCallum 30/09/2013 Approver David McCallum 30/09/2013 Issue Record Rev Date Description/Comments Author/Prepared by: Approved for Issue by: “The report shall be for the private and confidential use of the clients for whom the report is undertaken and should not be reproduced in whole or in part or relied upon by third parties for any use whatsoever without the express written authority of the Consultant’ Metro Interventions Appraisal Report: FINAL Report September 2013 CONTENTS 1. Introduction 1 1.1 Context 1.2 Report Purpose and Structure 2. Appraisal Methodology 3 2.1. Modal Interventions 2.2 Appraisal Criteria 2.3 Intervention Assessment 3. Appraisal Results and Recommended Interventions Packages 10 3.1 Appraisal Results by Intervention Category 3.2 Intervention Packages 3.3 Quick Wins 4. -

Investigation Report 2011-R001 Laois Traincare Depot Derailment 20
Investigation Report 2011-R001 Laois Traincare Depot Derailment th 20 January 2010 Laois Traincare Depot Derailment Document History Title Laois Traincare Depot Derailment, 20th January 2010 Document type Investigation Report Document number 2011-R001 Document issue date 19th January 2011 Revision Revision Summary of changes number date RAIU ii Investigation Report 2011-R001 Laois Traincare Depot Derailment Function of the Railway Accident Investigation Unit The Railway Accident Investigation Unit (RAIU) is a functionally independent investigation unit within the Railway Safety Commission (RSC). The purpose of an investigation by the RAIU is to improve railway safety by establishing, in so far as possible, the cause or causes of an accident or incident with a view to making recommendations for the avoidance of accidents in the future, or otherwise for the improvement of railway safety. It is not the purpose of an investigation to attribute blame or liability. The RAIU’s investigations are carried out in accordance with the Railway Safety Act 2005 and European railway safety directive 2004/49/EC. Any enquiries about this report should be sent to: RAIU Trident House Blackrock County Dublin Ireland RAIU iii Investigation Report 2011-R001 Laois Traincare Depot Derailment Executive Summary At 15.25 hours on the 20th January 2010 a Class 22000 six carriage train was scheduled to leave Laois Traincare Depot after routine servicing. The intended destination of the train was Heuston Station. The Train Driver performed his pre-departure checks and the Shunter authorised the train to proceed out of Laois Traincare Depot as far as signal PL278, which controls the exit from the depot onto the down loop adjacent to the main line. -

Rail Freight Study
Wigan Rail Freight Study Final Report Prepared for: Transport for Greater Manchester & Wigan Council by MDS Transmodal Limited Date: May 2012 Ref: 211076r_ver Final CONTENTS 1. Introduction and Background 2. Freight Activity in North West and Wigan 3. Inventory of Intermodal Terminals in North West 4. Economics of Rail Freight 5. Future Prospects and Opportunities 6. Summary, Conclusions and Next Steps Appendix: Data Tables COPYRIGHT The contents of this document must not be copied or reproduced in whole or in part without the written consent of MDS Transmodal 1. INTRODUCTION Wigan Council (alongside Transport for Greater Manchester ± TfGM) commissioned MDS Transmodal in December 2011 to undertake a study into rail freight within the Wigan Council area. The main objective of the study was to identify existing use of rail freight, assess realistic future prospects and determine what kind of facilities would need to be developed. The study will inform the development of a wider transport strategy for Wigan Council. This technical report documHQWSURYLGHVDVXPPDU\RIWKHVWXG\¶VPDLQILQGLQJV,WEURDGO\ covers the following: Background information and data concerning the rail freight sector nationally; An assessment of cargo currently lifted in the North West and Wigan area; An inventory of existing non-bulk rail terminal facilities in the North West and planned terminal developments; The economics of rail freight; Realistic future prospects and opportunities for rail in the Wigan area, including the identification of large freight traffic generators in the Wigan area i.e. organisations which potentially have sufficient traffic, either individually or combined, to generate full-length rail freight services; and Overall conclusions and recommended next steps. -

Rail Accident Report
Rail Accident Report Collision at Swanage station 16 November 2006 Report 35/2007 September 2007 This investigation was carried out in accordance with: l the Railway Safety Directive 2004/49/EC; l the Railways and Transport Safety Act 2003; and l the Railways (Accident Investigation and Reporting) Regulations 2005. © Crown copyright 2007 You may re-use this document/publication (not including departmental or agency logos) free of charge in any format or medium. You must re-use it accurately and not in a misleading context. The material must be acknowledged as Crown copyright and you must give the title of the source publication. Where we have identified any third party copyright material you will need to obtain permission from the copyright holders concerned. This document/publication is also available at www.raib.gov.uk. Any enquiries about this publication should be sent to: RAIB Email: [email protected] The Wharf Telephone: 01332 253300 Stores Road Fax: 01332 253301 Derby UK Website: www.raib.gov.uk DE21 4BA This report is published by the Rail Accident Investigation Branch, Department for Transport. Rail Accident Investigation Branch 3 Report 35/2007 www.raib.gov.uk September 2007 Collision at Swanage station 16 November 2006 Contents Introduction 6 Summary of the report 7 Key facts about the accident 7 Immediate cause, causal and contributory factors, underlying causes 7 Recommendations 8 The Accident 9 Summary of the accident 9 Location 9 The parties involved 10 External circumstances 10 The infrastructure 10 The train 12 Events -

Rail Accident Report
Rail Accident Report Collision at Pickering station North Yorkshire Moors Railway 5 May 2007 Report 29/2007 August 2007 This investigation was carried out in accordance with: l the Railway Safety Directive 2004/49/EC; l the Railways and Transport Safety Act 2003; and l the Railways (Accident Investigation and Reporting) Regulations 2005. © Crown copyright 2007 You may re-use this document/publication (not including departmental or agency logos) free of charge in any format or medium. You must re-use it accurately and not in a misleading context. The material must be acknowledged as Crown copyright and you must give the title of the source publication. Where we have identified any third party copyright material you will need to obtain permission from the copyright holders concerned. This document/publication is also available at www.raib.gov.uk. Any enquiries about this publication should be sent to: RAIB Email: [email protected] The Wharf Telephone: 01332 253300 Stores Road Fax: 01332 253301 Derby UK Website: www.raib.gov.uk DE21 4BA This report is published by the Rail Accident Investigation Branch, Department for Transport. Investigation into collision at Pickering station North Yorkshire Moors Railway, 5 May 2007 Contents Introduction 4 Summary 5 Location 5 The train and its crew 7 The incident 9 Conclusions 12 Actions reported as already taken by the NYMR 13 Recommendations 14 Appendices 15 Appendix A: Glossary of terms 15 Appendix B: NYMR damage report on GN General Managers Saloon 16 Rail Accident Investigation Branch Report 29/2007 www.raib.gov.uk August 2007 Introduction 1 The sole purpose of a Rail Accident Investigation Branch (RAIB) investigation is to prevent future accidents and incidents and improve railway safety.