Ebola Response System Strengthening Along Western Area Peninsula Coastline LESSONS LEARNED
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
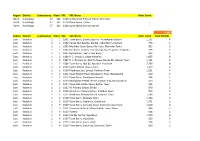
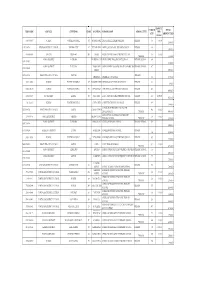
Region District Constituency Ward VRC VRC Name Voter Count North
Region District Constituency Ward VRC VRC Name Voter Count North Koinadugu 47 162 6169 Al-Harrakan Primary School, Woredala - North Koinadugu 47 162 6179 Open Space 2,Kabo - North Koinadugu 47 162 6180 Open Space, Kamayortortor - 9,493 Region District Constituency Ward VRC VRC Name Voter Count Total PS(100) East Kailahun 1 1 1001 Town Barry, Baoma, Baoma - Kunywahun Section 1,192 4 East Kailahun 1 1 1002 Palava Hut, Baoma, Baoma - Gborgborma Section 478 2 East Kailahun 1 1 1003 Mofindor Court Barry, Mofindor, Mofindor Town 835 3 East Kailahun 1 1 1004 Methodist primary school yengema, Yengama, Yengema 629 2 East Kailahun 1 1 1005 Nyanyahun Town, Town Barry 449 2 East Kailahun 1 2 1006 R. C. School 1, Upper Masanta 1,855 6 East Kailahun 1 2 1007 R. C. Primary 11, Gbomo Town, Buedu RD, Gbomo Town 1,121 4 East Kailahun 1 2 1008 Town Barry, Ngitibu, Ngitibu 1-Kailahum 2,209 8 East Kailahun 1 2 1009 KLDEC School, new London 1,259 4 East Kailahun 1 2 1010 Methodist Sec. School, Kailahun Town 1,031 4 East Kailahun 1 2 1011 Town Market Place, Bandajuma Town, Bandajuma 640 2 East Kailahun 1 2 1012 Town Barry, Bandajuma Sinneh 294 1 East Kailahun 1 2 1013 Bandajuma Health Centre, Luawa Foiya, Bandajuma Si 473 2 East Kailahun 1 2 1014 Town Hall, Borbu-Town, Borbu- Town 315 1 East Kailahun 1 2 1015 RC Primary School, Borbu 870 3 East Kailahun 1 2 1016 Amadiyya Primary School, Kailahun Town 973 3 East Kailahun 1 2 1017 Methodist Primary School, kailahun Town 1,266 4 East Kailahun 1 3 1018 Town Barry, Sandialu Town 1,260 4 East Kailahun 1 3 1019 Town -

Profile of Internal Displacement : Sierra Leone
PROFILE OF INTERNAL DISPLACEMENT : SIERRA LEONE Compilation of the information available in the Global IDP Database of the Norwegian Refugee Council (as of 15 October, 2003) Also available at http://www.idpproject.org Users of this document are welcome to credit the Global IDP Database for the collection of information. The opinions expressed here are those of the sources and are not necessarily shared by the Global IDP Project or NRC Norwegian Refugee Council/Global IDP Project Chemin Moïse Duboule, 59 1209 Geneva - Switzerland Tel: + 41 22 799 07 00 Fax: + 41 22 799 07 01 E-mail : [email protected] CONTENTS CONTENTS 1 PROFILE SUMMARY 6 EXECUTIVE SUMMARY 6 CAUSES AND BACKGROUND OF DISPLACEMENT 9 BACKGROUND TO THE CONFLICT 9 CHRONOLOGY OF SIGNIFICANT EVENTS SINCE INDEPENDENCE (1961 - 2000) 9 HISTORICAL OUTLINE OF THE FIRST EIGHT YEARS OF CONFLICT (1991-1998) 13 CONTINUED CONFLICT DESPITE THE SIGNING OF THE LOME PEACE AGREEMENT (JULY 1999-MAY 2000) 16 PEACE PROCESS DERAILED AS SECURITY SITUATION WORSENED DRAMATICALLY IN MAY 2000 18 RELATIVELY STABLE SECURITY SITUATION SINCE SIGNING OF CEASE-FIRE AGREEMENT IN ABUJA ON 10 NOVEMBER 2000 20 CIVIL WAR DECLARED OVER FOLLOWING THE FULL DEPLOYMENT OF UNAMSIL AND THE COMPLETION OF DISARMAMENT (JANUARY 2002) 22 REGIONAL EFFORTS TO MAINTAIN PEACE IN SIERRA LEONE (2002) 23 SIERRA LEONEANS GO TO THE POLLS TO RE-ELECT AHMAD TEJAN KABBAH AS PRESIDENT (MAY 2002) 24 SIERRA LEONE’S SPECIAL COURT AND TRUTH AND RECONCILIATION COMMISSION START WORK (2002-2003) 25 MAIN CAUSES OF DISPLACEMENT 28 COUNTRYWIDE DISPLACEMENT -

Profiles Was Part of the Transitional Government from 2003–2006
other war-affected and victims of sexual violence receive US$80. The september – Bio is struck on the head with a rock during a visit to EITI board renews Sierra Leone’s Candidate status, setting a new Bo, Sierra Leone’s second city. Several APC buildings are torched validation deadline of 9 December 2012. in retaliation and violence breaks out between rival SLPP and APC supporters. A temporary ban on political rallies is imposed. The UN August – SLPP selects the former head of the NPRC government, Security Council renews the UNIPSIL mandate for a further year with Julius Maada Bio, as its candidate for 2012 presidential elections. specific instructions to provide assistance during 2012 elections. Bio, popular in parts of the south and east, is criticised by opposition figures for alleged past abuses and his involvement in the 1992 coup. World Bank and UN official, Sirleaf first stood for election in 1997 and Profiles was part of the transitional government from 2003–2006. She was appointed President in elections in 2005. In her first year Sirleaf enacted a series of reforms aimed at fighting corruption and improving financial National accountability. She successfully lobbied the UN to lift sanctions and secured major debt relief from the World Bank. Sirleaf has faced Liberia criticisms domestically, most notably her slow implementation of recommendations made by the Truth and Reconciliation Commission Charles Taylor (TRC), which controversially recommended that she be barred from Charles Taylor was leader of the National Patriotic Front of Liberia public office. Her decision to contest 2011 presidential elections (NPFL) rebel group that invaded Liberia in 1989, sparking years of civil broke her earlier promise to stand down after one term in office. -

Aspects of the Population Geography of the Western Area, Sierra Leone
Durham E-Theses Aspects of the population geography of the western area, Sierra Leone Adeokun, Lawrence Adefemi How to cite: Adeokun, Lawrence Adefemi (1970) Aspects of the population geography of the western area, Sierra Leone, Durham theses, Durham University. Available at Durham E-Theses Online: http://etheses.dur.ac.uk/8056/ Use policy The full-text may be used and/or reproduced, and given to third parties in any format or medium, without prior permission or charge, for personal research or study, educational, or not-for-prot purposes provided that: • a full bibliographic reference is made to the original source • a link is made to the metadata record in Durham E-Theses • the full-text is not changed in any way The full-text must not be sold in any format or medium without the formal permission of the copyright holders. Please consult the full Durham E-Theses policy for further details. Academic Support Oce, Durham University, University Oce, Old Elvet, Durham DH1 3HP e-mail: [email protected] Tel: +44 0191 334 6107 http://etheses.dur.ac.uk ASPECTS OF THE POPULATION GEOGRAPHY OP THE WESTERN AREA. SIERRA l£OJ«E This thesis is largely based on data edited from original field sheets of the survey of sample households in the Western Area* It provides a description of the structure and distribution of selected population characteristics, an explanation of the patterns observed and an identification of population types and areas using principal components analysis0 In a brief original historical analysis, the population living within what is now the Western Area, prior to the esta• blishment of the 1787 settlement), is estimated to be about 3^000 persons. -

Gazette No. 6
The Sierra Leone Gazette Published by Authority Vol. CXLVI Thursday, 5th February, 2015 No. 6 G . N . Page CONTENTS NATIONAL ELECTORAL COMMISSION (NEC) G . N . Page 24 Public Service Notices ... ... 29-30 26 Declaration of Results ... 31-33 Office of the President BANK OF SIERRA LEONE 25 Day to be observed as Public Holiday 30 13-- COURT 23 Proforma Balance Sheet 31st January, to 28th November, 2014 respectively 34-44 12 Citation ... ... 30 Freetown. 5th February, 2015 Saccoh, Allieu F. B., Community Health Officer, 1.1.14. Barrie, Hawanatu A., House Officer, 1.11.14. Govt. Notice No. 24 Jalloh, Abdulai T., House Officer, 1.11.14. Kamara, Alusine R., House Officer, 1.11.14. Appointment Kamara, Ibrahim S., Nursing Officer, 1.8.14. Ministry of Defence Kanu, Abu Bakarr., House Officer, 1.11.14. Surrur, Hellen I., Higher Executive Officer, 1.1.15. Koroma, Abu Bakarr, House Officer, 1.11.14. Laggah, Michael, House Officer, 1.11.14. Ministry of Trade and Industry Sesay, Albertina, House Officer, 1.11.14. Bangura, Abdul A., Trade Monitor, 1.12.14. Sesay, Francess M. T., House Officer, 1.1.15. Bundu, Abdul Rahman., Trade Monitor, 1.12.14. Tanga, Wilma F., House Officer, 1.11.14. Kamara, Alusine M., Trade Monitor, 1.12.14. Surrur, Saida R., Higher Executive Officer, 1.1.15. Kamara, Taylor-Emerson., Trade Monitor, 1.12.14. Bundor, Jemba S., State Registered Nurse, 1.9.14. Kanu, Abu Bakarr., Trade Monitor, 1.12.14. Kalokoh, Marian S., State Registered Nurse, 1.9.14. Kargbo, Esheka., Trade Monitor, 1.12.14. -
Sierraleone Local Council Ward Boundary Delimitation Report
NATIONAL ELECTORAL COMMISSION Sierra Leone Local Council Ward Boundary Delimitation Report Volume Two Meets and Bounds April 2008 Table of Contents Preface ii A. Eastern region 1. Kailahun District Council 1 2. Kenema City Council 9 3. Kenema District Council 12 4. Koidu/New Sembehun City Council 22 5. Kono District Council 26 B. Northern Region 1. Makeni City Council 34 2. Bombali District Council 37 3. Kambia District Council 45 4. Koinadugu District Council 51 5. Port Loko District Council 57 6. Tonkolili District Council 66 C. Southern Region 1. Bo City Council 72 2. Bo District Council 75 3. Bonthe Municipal Council 80 4. Bonthe District Council 82 5. Moyamba District Council 86 6. Pujehun District Council 92 D. Western Region 1. Western Area Rural District Council 97 2. Freetown City Council 105 i Preface This part of the report on Electoral Ward Boundaries Delimitation process is a detailed description of each of the 394 Local Council Wards nationwide, comprising of Chiefdoms, Sections, Streets and other prominent features defining ward boundaries. It is the aspect that deals with the legal framework for the approved wards _____________________________ Dr. Christiana A. M Thorpe Chief Electoral Commissioner and Chair ii CONSTITUTIONAL INSTRUMENT No………………………..of 2008 Published: THE LOCAL GOVERNMENT ACT, 2004 (Act No. 1 of 2004) THE KAILAHUN DISTRICT COUNCIL (ESTABLISHMENT OF LOCALITY AND DELIMITATION OF WARDS) Order, 2008 Short title In exercise of the powers conferred upon him by subsection (2) of Section 2 of the Local Government Act, 2004, the President, acting on the recommendation of the Minister of Internal Affairs, Local Government and Rural Development, the Minister of Finance and Economic Development and the National Electoral Commission, hereby makes the following Order:‐ 1. -
Emis Code Council Chiefdom Ward Location School Name
AMOUNT ENROLM TOTAL EMIS CODE COUNCIL CHIEFDOM WARD LOCATION SCHOOL NAME SCHOOL LEVEL PER ENT AMOUNT PAID CHILD 5103-2-09037 WARDC WATERLOO RURAL 391 ROGBANGBA ABDUL JALIL ACADEMY PRIMARY PRIMARY 369 10,000 3,690,000 1291-2-00714 KENEMA DISTRICT COUNCIL KENEMA CITY 67 FULAWAHUN ABDUL JALIL ISLAMIC PRIMARY SCHOOL PRIMARY 380 3,800,000 4114-2-06856 BO CITY TIKONKO 289 SAMIE ABDUL TAWAB HAIKAL PRIMARY SCHOOL 610 10,000 PRIMARY 6,100,000 KONO DISTRICT TANKORO DOWN BALLOP ABDULAI IBN ABASS PRIMARY SCHOOL PRIMARY SCHOOL 694 1391-2-02007 6,940,000 KONO DISTRICT TANKORO TAMBA ABU ABDULAI IBNU MASSOUD ANSARUL ISLAMIC MISPRIMARY SCHOOL 407 1391-2-02009 STREET 4,070,000 5208-2-10866 FREETOWN CITY COUNCIL WEST III PRIMARY ABERDEEN ABERDEEN MUNICIPAL 366 3,660,000 5103-2-09002 WARDC WATERLOO RURAL 397 KOSSOH TOWN ABIDING GRACE PRIMARY SCHOOL PRIMARY 62 620,000 5103-2-08963 WARDC WATERLOO RURAL 373 BENGUEMA ABNAWEE ISLAMIC PRIMARY SCHOOOL PRIMARY 405 4,050,000 4109-2-06695 BO DISTRICT KAKUA 303 KPETEMA ACEF / MOUNT HORED PRIMARY SCHOOL PRIMARY 411 10,000.00 4,110,000 Not found WARDC WATERLOO RURAL COLE TOWN ACHIEVERS PRIMARY TUTORAGE PRIMARY 388 3,880,000 ACTION FOR CHILDREN AND YOUTH 5205-2-09766 FREETOWN CITY COUNCIL EAST III CALABA TOWN 460 10,000 DEVELOPMENT PRIMARY 4,600,000 ADA GORVIE MEMORIAL PREPARATORY 320401214 BONTHE DISTRICT IMPERRI MORIBA TOWN 320 10,000 PRIMARY SCHOOL PRIMARY 3,200,000 KONO DISTRICT TANKORO BONGALOW ADULLAM PRIMARY SCHOOL PRIMARY SCHOOL 323 1391-2-01954 3,230,000 1109-2-00266 KAILAHUN DISTRICT LUAWA KAILAHUN ADULLAM PRIMARY -

Volume One National Disaster Management
VOLUME ONE NATIONAL DISASTER MANAGEMENT PREPAREEDNESS PLAN 1 SECTION 1 1.0 INTRODUCTION The eleven year conflict in Sierra Leone underscores the need for a national disaster management plan with a coordinated and multi-sectoral approach to prevent, mitigate and respond to disasters. Events in recent times have shown that Sierra Leone is confronted with several hazards. These include weather, climatic, geological, ecological, pest, health, environment and other man-made hazards. The government of Sierra Leone has developed contingency plans for individual hazards and has harmonised these plans into a national plan through a comprehensive approach with inputs from the United Nations Agencies, Private Sector and other Non- Governmental Organisations. Some of these include the Vulnerability and Capacity Assessments jointly conducted by the Sierra Leone Red Cross Society and the Disaster Management Department and the National Hazard Profile developed by the Disaster Management Department. In spite of the good intention of government and its development partners to assist disaster victims, yet, it is clear that without a national plan that can be owned up by all the partners, efforts made would not be effective, efficient and comprehensive. Assistance of relief by disaster management experts would be better appreciated by disaster victims if it would be administered in a timely manner. This can only be achieved through a national disaster response plan. 2 1.1 PURPOSE The purpose of the National Disaster Preparedness and Response Plan (NDPRP) is to establish a comprehensive all-hazard approach to national incident management spectrum of activities including preparedness, prevention, mitigation, response and recovery. The plan incorporates best practices as shown in other regions of the world. -

Sierra Leone Year Report 2017
©- Sierra Leone Year Report 2017- Sierra Leone 2017 Year Report & Records of Interest (White necked Picatharte - Picathartes gymnocephalus ©David Monticelli) Momoh B. Sesay 1 ©- Sierra Leone Year Report 2017- INTRODUCTION This is the report of the activities, initiatives and the most interesting bird species that have been recorded in 2017 by myself or by others. The idea of this 39p. birding report - a first of its kind !- is : to give a global image of what has been seen and done in Sierra Leone in 2017; to hopefully open the way to new birding initiatives and field projects. The 2017 birding data have been collected from various internet platforms and sources as well as through contacting people. As a consequence, certain information is most probably missing. The enclosed annotated birdlist gives a fairly good snapshot of last year's available data. It also means you are definitely part of this year report initiative. So please, do contact us : for any further information or help; for giving us datas and feedbacks about your experience and any interesting birding records made around the country. Whatever the way you choose for birding Sierra Leone a lot is still to be done there. It is no terra incognita but for some tricky species, there still is no really reliable site in the country. I hope this first of his kind year report in this - magnificent and safe (!) - country of Sierra Leone will motivate more birdwatchers to come ! Best regards, Momoh B. Sesay I'm working as African Bird Club representative for Sierra Leone & as BirdLife International Field officer attached at Conservation Society of Sierra Leone (CSSL) helping Birdlife International on various projects - among other on the White-Necked Picarthertes at Kambui Hill Forest. -

Climate Change Vulnerability Assessment in Mangrove Regions of Sierra Leone
Climate Change Vulnerability Assessment in Mangrove regions of Sierra Leone Full Report January 2018 This work was conducted under the USAID-funded West Africa Biodiversity and Climate Change (WA BiCC) project. The report is an unabridged version of the official USAID report by the same name published as an Abridged Report in May 2017, and available at http://www.ciesin.columbia.edu/wa-bicc/wa-bicc-ccva-abridged-ff.pdf. The report was prepared by the Center for International Earth Science Information Network (CIESIN) of the Earth Institute of Columbia University. The vulnerability assessment was led by CIESIN under contract with Tetra Tech, and CIESIN also led the analysis and report development. In addition to the CIESIN lead researcher, Sylwia Trzaska, the field research was conducted by a team comprised of representatives from the WA BiCC technical unit in Freetown, Fourah Bay College, Njala University, the National Protected Areas Authority (NPAA), Environmental Protection Agency (EPA), the Ministry of Agriculture, Forestry and Food Security, the Ministry of Lands, Country Planning and Environment, the Ministry of Fisheries and Marine Resources, Conservation Society of Sierra Leone and other stakeholders. The authors of the report are Sylwia Trzaska, Alex de Sherbinin, Paola Kim-Blanco, Valentina Mara, Emilie Schnarr, Malanding Jaiteh, and Pinki Mondal at CIESIN. The team wishes to acknowledge the contributions of Zebedee Njisuh, Aiah Lebbie, Samuel Weekes, George Ganda and Michael Balinga. A full list of field research staff can be found in Annex 5 of this report. Without their hard work and dedication under challenging conditions, this vulnerability assessment would not have been possible. -

THE YAWRI BAY OVERVIEW Kambia District the YAWRI BAY Is Located on the Coast of Sierra Leone, on the Atlantic Ocean
West Africa Biodiversity and Climate Change Program THE YAWRI BAY OVERVIEW Kambia District THE YAWRI BAY is located on the coast of Sierra Leone, on the Atlantic Ocean. The Bay opens to the south-west of the country and is located about 25 km south of Freetown. LAND AREA Freetown Sierra Leone The total area of Yawri Bay is estimated at 29,505 ha. 29,505 ha PEOPLE • The Themene and Mende are the majority • 40.7% of the population (age 10 and above) ethnic groups. The region is also known to is illiterate. have several cosmopolitan settlements. • 88.3% of the Yawri Bay communities have • The local government operates through access to improved sources of drinking the Moyamba District council which has water such as public taps and well-secured legislative, financial, and administrative rivers or streams. powers. The district is further divided • Sanitation facilities include communal bush, into 14 chiefdoms controlled by tradition river beds, latrines, and buckets. Paramount Chiefs. • The Western area rural district (Waterloo) • The Western Area Rural District has a total is connected to the national grid and population of 444,270 people (221,351 receives hydro-powered electricity in the males and 22,1919 females). The Moyamba rainy season. Most other communities in District has 318,588 inhabitants (153,699 Yawri Bay depend on rechargeable batteries males and 164,889 females). or solar-powered devices for electricity. ECONOMY The employment rate The region is home to Agriculture is the main is 56% in the Moyamba some of the Sierra Leone’s economic driver in District and 73% in the primary fisheries and trade Moyamba, while trade Western rural area. -

Declaration of Results for Western Area Rural District Village Head Elections Held on Saturday 29Th June 2013
National Electoral Commission (NEC) OAU Drive, Tower Hill PRESS STATEMENT ON THE DECLARATION OF RESULTS FOR WESTERN AREA RURAL DISTRICT VILLAGE HEAD ELECTIONS HELD ON SATURDAY 29TH JUNE 2013 1. By the powers vested in it under section 33 of the 1991 Constitution of Sierra Leone (Act No. 6 of 1991) the National Electoral Commission conducted Village Head Elections on Saturday 29th June 2013 in the Western Area Rural District; 2. The Village Head Elections were conducted in accordance with the relevant electoral legal framework; 3. The Political Parties Registration Commission (PPRC), National Elections Watch (NEW), the Media were accredited observers for the elections; 4. The Sierra Leone Police ( SLP ) provided security in all centres where elections were held; 5. Vacancies were declared for a total of Ninety Six (96) Villages. The Commission received nominations for Ninety One (91) villages. Fifty Five (55) were contested and Thirty Six (36) uncontested. No nominations were received for the following five (5) Villages - i. Rikette-Banana Island, ii. Makonteh, iii. Malamina, iv. Masorie Nyor and v. Bekemakandor. The positions of Village Head for these villages therefore remain vacant until they are filled by elections conducted by the National Electoral Commission. Page 1 of 10 DECLARATION OF RESULTS A. UNCONTESTED By the powers vested in me, as National Returning Officer, I hereby declare as duly elected the sole nominated candidates as Village Heads in the following Villages: VILLAGE NAME OF CANDIDATE 1. BATH-KUMP KANU KABBA 2. BUREH TOWN TUCKER MICHAEL 3. CHARLOTTE HARDING CATHERINE K. 4. DEVIL HOLE SESAY ALHAJI IBRAHIM 5. FABAINA CONTEH SAIDU 6.