PEI-EPI Synergy in Pakistan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
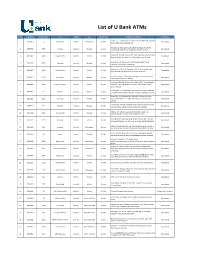
List of U Bank Atms
List of U Bank ATMs Sr No ATM ID No. Branch Code City Region Area ON /Off Site Complete ATM Address ATM Status HOUSE 17, TEXATION B-III, 2784/2, IHATA SINDA RAM, STADIUM 1 20190062 62 Bahawalpur Central 1 Bahawalpur On Site Operational ROAD FARID GATE BAHAWALPUR KHATANO.8, KHATOONI NO.63, NEAR HBL BRANCH LAYYAH 2 20193030 3030 Chobara Central 1 Bhakkar On Site Operational FAISALABAD ROAD, TEHSIL CHOBARA, DISTRICT LAYYAH. Khewat No.581/558 Khatooni No. 1969, Opposite Usmania Masjid, 3 20193004 3004 Ahmed Pur Sial Central 1 Multan On Site Operational Main Ahmedpur Sial Road, Tehsil Ahmedpur, District Jhang. Khewat No. 145, Khatooni No. 293, Rang Pur Adda, Tehsil 4 20193035 3035 Paharpur Central 1 Bhakkar On Site Operational Paharpur, District Dear Ismael khan. Khatooni no. 191 & 199, Khata No. 63/27973, Kacha Kho road, 5 20193003 3003 Abdul Hakeem Central 1 Multan On Site Operational Nized Sabzi Mandi Abdul Hakeem, district Khanewal. Khata 51, Khatoni 72 Near govt. college of commerce railway 6 20194654 4654 Darya Khan Central 1 Bhakkar On Site Operational road Darya Khan District Bhakkar Khewat No.449/443, Khatooni No. 1616 to 1617, Opposite Higher 7 20193024 3024 Qadir Pur Rawan Central 1 Multan On Site Secondary School Qadir Pur Ran towan, Tehsil Multan Sadar, Operational District Multan. KHEWAT NO. 431, KHATOONI 786, MOZA NEEL KOT CHUNGI NO 8 20190061 61 Multan Central 1 Multan On Site Operational 6, BOSAN ROAD PUNJAB NURSERY GULGASHT COLONY, MULTAN. KHATA NO.103, KHATOONI NO. 398-407, LAYYAH, KOT ADDU 9 20193001 3001 Kot Sultan Central 1 Bhakkar On Site ROAD, NEAR ASKAR 1 PETROL PUMP, KOT SULTAN DISTRICT Operational LAYYAH. -

Population Distribution in Sindh According to Census 2017 (Population of Karachi: Reality Vs Expectation)
Volume 3, Issue 2, February – 2018 International Journal of Innovative Science and Research Technology ISSN No:-2456 –2165 Population Distribution in Sindh According to Census 2017 (Population of Karachi: Reality vs Expectation) Dr. Faiza Mazhar TTS Assistant Professor Geography Department. Government College University Faisalabad, Pakistan Abstract—Sindh is our second largest populated province. Historical Populations Growth of Sindh It has a great role in culture and economy of Pakistan. Karachi the largest city of Pakistan in terms of population Census Year Total Population Urban Population also has a unique impact in development of Pakistan. Now 1951 6,047,748 29.23% according to the current census of 2017 Sindh is again 1961 8,367,065 37.85% standing on second position. Karachi is still on top of the list in Pakistan’s ten most populated cities. Population of 1972 14,155,909 40.44% Karachi has not grown on an expected rate. But it was due 1981 19,028,666 43.31% to many reasons like bad law and order situation, miss management of the Karachi and use of contraceptive 1998 29,991,161 48.75% measures. It would be wrong if it is said that the whole 2017 47,886,051 52.02% census were not conducted in a transparent manner. Source: [2] WWW.EN.WIKIPEDIA.ORG. Keywords—Component; Formatting; Style; Styling; Insert Table 1: Temporal Population Growth of Sindh (Key Words) I. INTRODUCTION According to the latest census of 2017 the total number of population in Sindh is 48.9 million. It is the second most populated province of Pakistan. -

Detailed Species Accounts from The
Threatened Birds of Asia: The BirdLife International Red Data Book Editors N. J. COLLAR (Editor-in-chief), A. V. ANDREEV, S. CHAN, M. J. CROSBY, S. SUBRAMANYA and J. A. TOBIAS Maps by RUDYANTO and M. J. CROSBY Principal compilers and data contributors ■ BANGLADESH P. Thompson ■ BHUTAN R. Pradhan; C. Inskipp, T. Inskipp ■ CAMBODIA Sun Hean; C. M. Poole ■ CHINA ■ MAINLAND CHINA Zheng Guangmei; Ding Changqing, Gao Wei, Gao Yuren, Li Fulai, Liu Naifa, Ma Zhijun, the late Tan Yaokuang, Wang Qishan, Xu Weishu, Yang Lan, Yu Zhiwei, Zhang Zhengwang. ■ HONG KONG Hong Kong Bird Watching Society (BirdLife Affiliate); H. F. Cheung; F. N. Y. Lock, C. K. W. Ma, Y. T. Yu. ■ TAIWAN Wild Bird Federation of Taiwan (BirdLife Partner); L. Liu Severinghaus; Chang Chin-lung, Chiang Ming-liang, Fang Woei-horng, Ho Yi-hsian, Hwang Kwang-yin, Lin Wei-yuan, Lin Wen-horn, Lo Hung-ren, Sha Chian-chung, Yau Cheng-teh. ■ INDIA Bombay Natural History Society (BirdLife Partner Designate) and Sálim Ali Centre for Ornithology and Natural History; L. Vijayan and V. S. Vijayan; S. Balachandran, R. Bhargava, P. C. Bhattacharjee, S. Bhupathy, A. Chaudhury, P. Gole, S. A. Hussain, R. Kaul, U. Lachungpa, R. Naroji, S. Pandey, A. Pittie, V. Prakash, A. Rahmani, P. Saikia, R. Sankaran, P. Singh, R. Sugathan, Zafar-ul Islam ■ INDONESIA BirdLife International Indonesia Country Programme; Ria Saryanthi; D. Agista, S. van Balen, Y. Cahyadin, R. F. A. Grimmett, F. R. Lambert, M. Poulsen, Rudyanto, I. Setiawan, C. Trainor ■ JAPAN Wild Bird Society of Japan (BirdLife Partner); Y. Fujimaki; Y. Kanai, H. -

An Assessment of the Spatial and Temporal Distribution of Soil Salinity in Combination with Field and Satellite Data: a Case Study in Sujawal District
agronomy Article An Assessment of the Spatial and Temporal Distribution of Soil Salinity in Combination with Field and Satellite Data: A Case Study in Sujawal District Kashif Ali Solangi 1, Altaf Ali Siyal 2, Yanyou Wu 1,*, Bilawal Abbasi 3 , Farheen Solangi 3, Imran Ali Lakhiar 1 and Guiyao Zhou 4 1 Key Laboratory of Modern Agricultural Equipment and Technology, Ministry of Education, Institute of Agricultural Engineering, Jiangsu University, Zhenjiang 212013, Jiangsu, China; [email protected] (K.A.S.); [email protected] (I.A.L.) 2 U.S.-Pakistan Center for Advanced Studies in Water Mehran University of Engineering & Technology, Jamshoro 76062, Sindh, Pakistan; [email protected] 3 Institute of Agricultural Resources and Regional Planning, Chinese Academy of Agricultural Sciences, Beijing 100081, China; [email protected] (B.A.); [email protected] (F.S.) 4 Zhejiang Tiantong Forest Ecosystem National Observation and Research Station, Center for Global Change and Ecological Forecasting, East China Normal University, School of Ecological and Environmental Sciences, East China Normal University, Shanghai 200241, China; [email protected] * Correspondence: [email protected]; Tel.: +86-0851-8439-1746 Received: 1 November 2019; Accepted: 6 December 2019; Published: 10 December 2019 Abstract: Soil salinization is a serious environmental issue that significantly influences crop yield and soil fertility, especially in coastal areas. Numerous studies have been conducted on the salinity status in Pakistan. Information about the geospatial and temporal distribution of salinity in the Sujawal district is still lacking. The present study examines the soil salinity status and the impact of seawater intrusion in the entire district from 1990 to 2017 using field and remote sensing (RS) data. -

Bid Evaluation Report
NO.XEN/MA/TC/SIND / GOVERNMENT OF SIN H OFFICE OF THE EXECUTIVE GINEER, Minority Affair Sindh, Barra• No12 Sindh Secretariats 4A, Karac i dated The Manager (CB) Sindh Public Procurement Regulatory Authority, Government of Sindh, Karachi SUBJECT:- NIT NO. XEN/EE-I/154 — DATED: 17-01-2017 Kindly refer as subject, in this context, it is submi ed that above said tenders were opened on dated: 23/02/2017 at 3:00 p.m. in the presence of ember of procurement committee and bidders / representatives of bidders. Bid evaluatio Reports, Attendance Sheet, Minutes of the Meeting of bid opening are attached herewith as d ired. I. Minutes of the Meeting 2. Attendance Sheet 3. Bid Evaluation Report Ex utiv Engineer Minor ties Affairs Sind!) it i OFFICE OF THE EXECUTIVE ENGINEER, MINO' TY AFFAIR SINDH, BARRACK N012 SINDH SECRETARIATS 4 , KARACHI MINUTES OF THE MEET I G SUBJECT: MINUTES OF THE MEETING HELD 0 AT THE MINORITY AFFAIR SINDH, BARRACK NO 12 SIND SECRETARIATS 4A KARACHI FOR OPENING OF TE rt ERS. Ref:- N.I.T. NO. XEN/EE-I/154 DATED:- 17-01-2117 The tenders for the following works were invited by t e Executive Engineer, Minorities Affairs Department Vide NIT No. referred abov. In this respect, a meeting regarding opening of tenders held on 23/02/2017, at the office of the office of the Executive Engineer, Minority Affair Sindh, Barrack Nol ► Sindh Secretariats 4A, Karachi Under the Chairmanship of Chairman Procurement ommittee / The tenders were opened at 3:00 p.m. as per schedule in the presence of Chairman & members of procurement committee, as well as Government contractor's welfare, Association & bidders / representatives of bidders (Attendan e Sheet is attached herewith) Total 81 Nos. -

(RNA) Monsoon Rains
Rapid Need Assessment Report (RNA) Monsoon Rains Thatta, Sujawal and Hyderabad th th 24 – 27 August 2020 Thatta Sujjawal Hyderabad Prepared by: Health And Nutrition Development Society (HANDS) Address: Plot #158, Off M9 (Karachi – Hyderabad) Motorway, Gadap Road, Karachi, Pakistan, Ph: (0092-21) 32120400-9 , +92-3461117771 Web: www.hands.org.pk Email: [email protected] Table of Contents 1. Introduction ......................................................................................................................................... 3 1.1. Background ................................................................................................................................. 3 1.2. Objectives .................................................................................................................................... 4 1.3. Methodology ................................................................................................................................ 4 1.4. Limitations ................................................................................................................................... 4 1.5. Summary of Findings ................................................................................................................. 4 1.6. Sectoral Need Priority Ranking................................................................................................. 6 2. Key Findings District Thatta .............................................................................................................. -

Public Notice Auction of Gold Ornaments and Valuables
PUBLIC NOTICE AUCTION OF GOLD ORNAMENTS AND VALUABLES Finance facilities were extended by JS Bank Limited to its customers mentioned below against the security of deposit and pledge of Gold ornaments/valuables. The customers have neglected and failed to repay the finances extended to them by JS Bank Limited along with the mark-up thereon. The current outstanding liability of such customers is mentioned below. Notice is hereby given to the under mentioned customers that if payment of the entire outstanding amount of finance along with mark-up is not made by them to JS Bank Limited within 15 days of the publication of this notice, JS Bank Limited shall auction the Gold ornaments/valuables after issuing public notice regarding the date and time of the public auction and the proceeds realized from such auction shall be applied towards the outstanding amount due and payable by the customers to JS Bank Limited. No further public notice shall be issued to call upon the customers to make payment of the outstanding amounts due and payable to JS Bank as mentioned hereunder: Total Outstanding as ACCOUNT Customer Name Address of 8th March, 2020 1419730 TASNEEM 698,499 HOUSE NO E 37 MOHALL AH GULISTAN E SAJJAD QASIMABAD HYDERABAD HYDERABAD 1263339 MIR MUHAMMAD ALI 362,212 H NO 52 PARO CIVIL L INES HYDERABAD HYDERABAD 1299330 AHSAN ALI 261,430 KHALIFO FILLING STAT ION NEAR ALFALAH BANK KACHERY ROAD KHAIRPUR KHAIRPUR 1346800 MUHAMMAD SHAHBAN 248,049 VILLAGE BANGHAO BULL O BULLA PO KOT BULLO TAL PANOA KIL DISTT SUKKUR SUKKUR 1250313 SIDRA TALAT 234,822 -

Environmental and Social Management Framework Pakistan
Environmental and Social Management Public Disclosure Authorized Framework Pakistan Integrated Literacy and Skills Development for Youth Project Public Disclosure Authorized Public Disclosure Authorized Draft Public Disclosure Authorized Sanjh Preet Organization Date: June 30, 2020 Pakistan Integrated Literacy and Skills Development for Youth Project Executive Summary Introduction Outbreak of COVID-19 since March 2020 has worsened the educational situation in Pakistan. The disruption of education services during the COVID-19 pandemic will disproportionately affect disadvantaged and unreached children, including girls and young women. Despite an increasing trend in the enrollment rate in the pre-pandemic time, a large number of children still remained out-of-school, the situation is likely to be worsened. The National Education Management Information Systems (NEMIS) estimates that around 22 million children were out of school in 2016/17, of which there were more than 5 million out-of-school children in primary school ages 5–9 years, more than 11 million in ages 10–14 years, and 6.2 million in age 15–16 years. Even before the COVID-19 pandemic, education systems in both Punjab and Sindh provinces faced major challenges, including limited school access and low retention rates. Provincial governments are responsible for providing free and compulsory education to all children aged 5-16 years in their respective provinces. School Education and Literacy Department (SELD) in Sindh and Literacy & Non-Formal Basic Education Department (LNFBED) in Punjab are respectively responsible for non-formal education. In both provinces, lack of school access and high dropout rates, especially at the primary level, are responsible for its large out-of-school population. -

Text Begins Here
SECRETARIAT - 150 route de Ferney, P.O. Box 2100, 1211 Geneva 2, Switzerland - TEL: +41 22 791 6033 - FAX: +41 22 791 6506 www.actalliance.org Appeal Pakistan Assistance to the Flood-Affected Families in Sindh & Punjab - PAK151 Revision 1 Appeal Target: US$268,794 Balance Requested: US$129,942 Geneva, 3 November 2015 Dear Colleagues, The ongoing flood emergency has further aggravated the lives and livelihoods of the affected communities in all the provinces of Pakistan and Azad Jammu & Kashmir (AJK) State. The rains which started in mid-July are continuing and hampering the daily routine and livelihood of the affected communities. Until recently, the National Disaster Management Authority (NDMA) recorded 917,791 people affected, 173 deaths and 127 injuries owing to the devastating floods. In Sindh, it has affected mostly the katcha area of the six districts, however it is anticipated that it will flow further to the low lying districts of the province. Rapid needs assessments were conducted by teams from both Community World Service Asia and NCA and their partners in the last week of July in District Ghotki and Kashmore in Sindh. NCA went on to conduct WASH assessments in Districts Layyah, Rajanpur and Muzaffargarh (Punjab). Through interviewing the affected population and observing the damage, the assessment team found that food, water and sanitation, immediate healthcare, non-food items and emergency shelters are top priority needs at this stage. In August there was also a joint multi-sectoral needs assessment of 12 districts, including District Sujawal, along with 19 other international and local NGOs using the UN MIRA assessment questionnaire. -
Branch Network
As ON 31-03-2014 Branch Network Domestic Operations – 1,217 Overseas Operations - 09 Branches – 1,208 Sri Lanka - 07 Retail – 1,161 Privilege – 10 WBG – 10 Bahrain - 01 Islamic – 27 Retail Sub-Branches – 09 EPZ - 01 UAE - 01 (Rep. Office) MCB Bank Limited FINANCIAL CONTROL GROUP (SOUTH) "BRANCH LICENSING UNIT" 18th Floor, MCB Tower I.I. Chundrigar Road, Karachi BRANCH NETWORK AS ON 31-03-2014 RETAIL BANKING GROUP RETAIL BANKING GROUP - SOUTH RETAIL BANKING GROUP - CENTRAL Circle/ Region No. No. Page Circle/ Region No. No. Page No. of Brs. of Brs. of Sub- No. No. of Brs. of Brs. of Sub- No. Brs. Brs. 1. KARACHI CITY 01. Karachi City 21 - 1-2 1. LAHORE 01.Lahore Central 24 - 36-37 45 02. Karachi North 24 - 3-4 97 02.Lahore City 23 - 38-39 03.Lahore East 26 - 40-41 2. KARACHI EAST 03. Karachi East 21 - 5-6 04.Lahore West 24 - 42-43 41 04. Karachi South 20 - 7-8 2. FAISALABAD 05.Faisalabad 36 - 44-45 3. KARACHI WEST 05. Karachi Central 21 - 9-10 101 06.Faisalabad City 37 - 46-47 42 06. Karachi West 21 - 11-12 07.Sheikhupura 28 - 48-49 3. GUJRANWALA 08.Gujranwala 27 1 50-51 4. HYDERABAD 07. Hyderabad 36 - 13-14 94 09.Gujrat 35 1 52-53 65 08. Nawabshah 29 1 15-16 10.Sialkot 32 - 54-55 4. SARGODHA 11.Jhang 30 1 56-57 5. QUETTA 09. Makran 10 - 17 92 12.Mianwali 29 - 58-59 41 Quetta 31 - 18-19 13.Sargodha 33 - 60-61 TOTAL RBG - SOUTH 234 01 TOTAL RBG - CENTRAL 384 03 RETAIL BANKING GROUP - EAST RETAIL BANKING GROUP - NORTH 1. -

View of the Above Stated Facts in Above Two Revision
ORDER SHEET IN THE HIGH COURT OF SINDH AT KARACHI Civil Revision Application No.74 of 2005 & Civil Revision Application No.75 of 2005 ------------------------------------------------------------------------------------- Date Order with signature of Judge ------------------------------------------------------------------------------------- Present: Mr. Justice Nazar Akbar 1. Civil Revision Application No.74 of 2005 Applicant No.1 : Ghulam Sarwar Applicant No.2 : Ghulam Jilani Applicant No.3 : Qamaruddin Applicant No.4 : Badaruddin Applicant No.5 : Fakharuddin Applicant No.6 : Mst. Attia Begum Applicant No.7 : Mst. Almas Begum Applicant No.8 : Mst. Durdana Applicant No.9 : Sikandar Applicant No.10 : Shahid All sons and daughters of Abdul Ghafoor through Mr. Muhammad Sadiq Hidayatullah, Advocate. Versus Respondent No.1 : Mst. Rahima Respondent No.2 : Ghulam Sheedi Respondent No.3 : Rafiq Ahmed Shah Respondent No.4 : Bibi Najmu Nisa Respondent No.5 : Shafquat Hussain Shah Respondent No.6 : Inam Hussain Shah Respondent No.7 : Bibi Munawar Sultana Respondent No.8 : Bibi Azra Begum Respondent No.9 : Bibi Jamila Begum Respondent No.10 : Mst. Bushra Bibi. At Sr. No.3 to 10 sons and daughters of Syed Nawaz Ali Shah. (Nemo for Respondents). 2. Civil Revision Application No.75 of 2005 Applicant No.1 : Badaruddin Applicant No.2 : Qamaruddin Applicant No.3 : Fakharuddin Applicant No.4 : Ghulam Jilani Applicant No.5 : Ghulam Sarwar Applicant No.6 : Sikandar Applicant No.7 : Shakeel Applicant No.8 : Mst. Atiya Begum Applicant No.9 : Mst. Almas Begum Applicant No.10 : Mst. Durdani All sons and daughters of Abdul Ghafoor through Mr. Muhammad Sadiq Hidayatullah, advocate. 2 Versus Respondent No.1 : Province of Sindh through its Secretary, Government of Sindh, Revenue Department. -
Copy of Compiled List Phone Nos BISP ALL Regions Dated 21.05
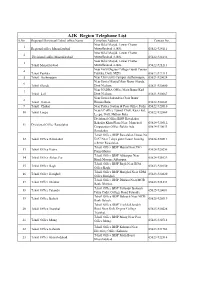
AJK Region Telephone List S.No Regioanl/Divisioanl/Tehsil office Name Complete Address Contact No. Near Bilal Masjid, Lower Chatter 1 Regional office Muzaffarabad Muzaffarabad AJ&K. 05822-924111 Near Bilal Masjid, Lower Chatter 2 Divisional office Muzaffarabad Muzaffarabad AJ&K. 05822-924132 Near Bilal Masjid, Lower Chatter 3 Tehsil Muzaffarabad Muzaffarabad AJ&K. 05822-921213 Near Girls Degree College Gandi Peeran 4 Tehsil Patikka Patikka, Distt. MZD. 05822-922113 5 Tehsil Authmaqam Near University Campus Authamaqam, 05821-920024 Near Jamia Masjid Main Bazar Sharda, 6 Tehsil Sharda Distt Neelum. 05821-920800 Near NADRA Office Main Bazar Kail 7 Tehsil kail Distt Neelum. 05821-920667 Near Jamia Sakandria Chok Bazar 8 Tehsil Hattian Hattian Bala. 05822-922643 9 Tehsil Chakar Near Police Station & Post Office Pothi 05822-922010 NearAC office Tunnel Chok, Kaser kot, 10 Tehsil Leepa 05822-922869 Leepa, Distt. Hattian Bala. Divisional Office BISP Rawalakot Bahadar Khan Plaza Near Muncipal 05824-920512, 11 Divisional Office Rawalakot Corporation Office Baldia Ada 05824-920033 Rawalakot. Tehsil Office BISP Rawalakot House No 12 Tehsil Office Rawalakot D-97 Near 7 days guest house housing 05824-920511 scheme Rawalakot. Tehsil Office BISP Hajira Near PSO 13 Tehsil Office Hajira 05824-920256 Pump Hajira. Tehsil Office BISP Abbaspur Near 14 Tehsil Office Abbas Pur 05824-921029 Hanfi Mosque Abbaspur. Tehsil Office BISP Bagh Near BDA 15 Tehsil Office Bagh 05823-920150 Office Bagh. Tehsil Office BISP Harighel Near SDM 16 Tehsil Office Harighel 05823-920820 Office Harighel. Tehsil Office BISP Dhirkot Near MCB 17 Tehsil Office Dhirkot 05823-921233 Bank Dhirkot. Tehsil Office BISP Pallandri Balouch 18 Tehsil Office Palandri 05825-920081 Palza Cadet College Road Palandri.