Physiotherapy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WCN19 Journal Posters Part 2 Revised V1
JNS-0000116542; No. of Pages 131 ARTICLE IN PRESS Journal of the Neurological Sciences (2019) xxx–xxx Contents lists available at ScienceDirect Journal of the Neurological Sciences journal homepage: www.elsevier.com/locate/jns WCN19 Journal Posters Part 2 revised_V1 WCN19-2260 WCN19-2269 Poster shift 01 - Channelopathies /neuroethics /neurooncology / Poster shift 01 - Channelopathies /neuroethics /neurooncology / pain - Part I /sleep disorders - Part I /stem cells and gene therapy - pain - Part I /sleep disorders - Part I /stem cells and gene therapy - Part I /stroke /training in neurology - Part I and traumatic brain Part I /stroke /training in neurology - Part I and traumatic brain injury injury Numb chin syndrome- The first finding in metastatic malignancy Results of surgical treatment in patients with moyamoya disease considering CT-perfusion imaging study N. Mustafayev, A. Bayrakoglu, F. Ilgen Uslu, M. Kolukısa Bezmialem University, Neurology, Istanbul, Turkey O. Harmatinaa, V. Morozb, I. Skorokhodab, I. Tyshb, N. Shahinb,R. Hanemb, U. Maliarb a Numb chin syndrome (NCS) is a sensory neuropathy of the SI «Romodanov Institute of Neurosurgery of NAMS of Ukraine», mental nerve, which is accompanied by hypoesthesia and paresthe- Neuroradiology Department, Kyiv, Ukraine b sia of the jaw and lower lip. Although being well known in neurology SI «Romodanov Institute of Neurosurgery of NAMS of Ukraine», practice, most of the physicians who have not experienced this Emergency Department of Vascular Neurosurgery, Kyiv, Ukraine phenomenon are unaware of this phenomenon since it is rare and can be confused with somatic complaints. This case report aims to Aim point out that NCS may be the first sign and symptom of metastatic To improve the results of surgical treatment of patients with cancers in patients who are not diagnosed. -

Dural Venous Channels: Hidden in Plain Sight–Reassessment of an Under-Recognized Entity
Published July 16, 2020 as 10.3174/ajnr.A6647 ORIGINAL RESEARCH INTERVENTIONAL Dural Venous Channels: Hidden in Plain Sight–Reassessment of an Under-Recognized Entity M. Shapiro, K. Srivatanakul, E. Raz, M. Litao, E. Nossek, and P.K. Nelson ABSTRACT BACKGROUND AND PURPOSE: Tentorial sinus venous channels within the tentorium cerebelli connecting various cerebellar and su- pratentorial veins, as well as the basal vein, to adjacent venous sinuses are a well-recognized entity. Also well-known are “dural lakes” at the vertex. However, the presence of similar channels in the supratentorial dura, serving as recipients of the Labbe, super- ficial temporal, and lateral and medial parieto-occipital veins, among others, appears to be underappreciated. Also under-recog- nized is the possible role of these channels in the angioarchitecture of certain high-grade dural fistulas. MATERIALS AND METHODS: A retrospective review of 100 consecutive angiographic studies was performed following identification of index cases to gather data on the angiographic and cross-sectional appearance, location, length, and other features. A review of 100 consecutive dural fistulas was also performed to identify those not directly involving a venous sinus. RESULTS: Supratentorial dural venous channels were found in 26% of angiograms. They have the same appearance as those in the tentorium cerebelli, a flattened, ovalized morphology owing to their course between 2 layers of the dura, in contradistinction to a rounded cross-section of cortical and bridging veins. They are best appreciated on angiography and volumetric postcontrast T1- weighted images. Ten dural fistulas not directly involving a venous sinus were identified, 6 tentorium cerebelli and 4 supratentorial. -

Cerebellar Disease in the Dog and Cat
CEREBELLAR DISEASE IN THE DOG AND CAT: A LITERATURE REVIEW AND CLINICAL CASE STUDY (1996-1998) b y Diane Dali-An Lu BVetMed A thesis submitted for the degree of Master of Veterinary Medicine (M.V.M.) In the Faculty of Veterinary Medicine University of Glasgow Department of Veterinary Clinical Studies Division of Small Animal Clinical Studies University of Glasgow Veterinary School A p ril 1 9 9 9 © Diane Dali-An Lu 1999 ProQuest Number: 13815577 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest ProQuest 13815577 Published by ProQuest LLC(2018). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLC. ProQuest LLC. 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106- 1346 GLASGOW UNIVERSITY lib ra ry ll5X C C ^ Summary SUMMARY________________________________ The aim of this thesis is to detail the history, clinical findings, ancillary investigations and, in some cases, pathological findings in 25 cases of cerebellar disease in dogs and cats which were presented to Glasgow University Veterinary School and Hospital during the period October 1996 to June 1998. Clinical findings were usually characteristic, although the signs could range from mild tremor and ataxia to severe generalised ataxia causing frequent falling over and difficulty in locomotion. -

SŁOWNIK ANATOMICZNY (ANGIELSKO–Łacinsłownik Anatomiczny (Angielsko-Łacińsko-Polski)´ SKO–POLSKI)
ANATOMY WORDS (ENGLISH–LATIN–POLISH) SŁOWNIK ANATOMICZNY (ANGIELSKO–ŁACINSłownik anatomiczny (angielsko-łacińsko-polski)´ SKO–POLSKI) English – Je˛zyk angielski Latin – Łacina Polish – Je˛zyk polski Arteries – Te˛tnice accessory obturator artery arteria obturatoria accessoria tętnica zasłonowa dodatkowa acetabular branch ramus acetabularis gałąź panewkowa anterior basal segmental artery arteria segmentalis basalis anterior pulmonis tętnica segmentowa podstawna przednia (dextri et sinistri) płuca (prawego i lewego) anterior cecal artery arteria caecalis anterior tętnica kątnicza przednia anterior cerebral artery arteria cerebri anterior tętnica przednia mózgu anterior choroidal artery arteria choroidea anterior tętnica naczyniówkowa przednia anterior ciliary arteries arteriae ciliares anteriores tętnice rzęskowe przednie anterior circumflex humeral artery arteria circumflexa humeri anterior tętnica okalająca ramię przednia anterior communicating artery arteria communicans anterior tętnica łącząca przednia anterior conjunctival artery arteria conjunctivalis anterior tętnica spojówkowa przednia anterior ethmoidal artery arteria ethmoidalis anterior tętnica sitowa przednia anterior inferior cerebellar artery arteria anterior inferior cerebelli tętnica dolna przednia móżdżku anterior interosseous artery arteria interossea anterior tętnica międzykostna przednia anterior labial branches of deep external rami labiales anteriores arteriae pudendae gałęzie wargowe przednie tętnicy sromowej pudendal artery externae profundae zewnętrznej głębokiej -

High-Yield Neuroanatomy, FOURTH EDITION
LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page i Aptara Inc. High-Yield TM Neuroanatomy FOURTH EDITION LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page ii Aptara Inc. LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page iii Aptara Inc. High-Yield TM Neuroanatomy FOURTH EDITION James D. Fix, PhD Professor Emeritus of Anatomy Marshall University School of Medicine Huntington, West Virginia With Contributions by Jennifer K. Brueckner, PhD Associate Professor Assistant Dean for Student Affairs Department of Anatomy and Neurobiology University of Kentucky College of Medicine Lexington, Kentucky LWBK110-3895G-FM[i-xviii].qxd 8/14/08 5:57 AM Page iv Aptara Inc. Acquisitions Editor: Crystal Taylor Managing Editor: Kelley Squazzo Marketing Manager: Emilie Moyer Designer: Terry Mallon Compositor: Aptara Fourth Edition Copyright © 2009, 2005, 2000, 1995 Lippincott Williams & Wilkins, a Wolters Kluwer business. 351 West Camden Street 530 Walnut Street Baltimore, MD 21201 Philadelphia, PA 19106 Printed in the United States of America. All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appearing in this book prepared by individuals as part of their official duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Lippincott Williams & Wilkins at 530 Walnut Street, Philadelphia, PA 19106, via email at [email protected], or via website at http://www.lww.com (products and services). -

Naturopathic Physical Medicine
Naturopathic Physical Medicine Publisher: Sarena Wolfaard Commissioning Editor: Claire Wilson Associate Editor: Claire Bonnett Project Manager: Emma Riley Designer: Charlotte Murray Illustration Manager: Merlyn Harvey Illustrator: Amanda Williams Naturopathic Physical Medicine THEORY AND PRACTICE FOR MANUAL THERAPISTS AND NATUROPATHS Co-authored and edited by Leon Chaitow ND DO Registered Osteopath and Naturopath; Former Senior Lecturer, University of Westminster, London; Honorary Fellow, School of Integrated Health, University of Westminster, London, UK; Fellow, British Naturopathic Association With contributions from Additional contributions from Eric Blake ND Hal Brown ND DC Nick Buratovich ND Paul Orrock ND DO Michael Cronin ND Matthew Wallden ND DO Brian Isbell PhD ND DO Douglas C. Lewis ND Co-authors of Chapter 1: Benjamin Lynch ND Pamela Snider ND Lisa Maeckel MA CHT Jared Zeff ND Carolyn McMakin DC Foreword by Les Moore ND Joseph Pizzorno Dean E. Neary Jr ND Jr ND Roger Newman Turner ND DO David Russ DC David J. Shipley ND DC Brian K. Youngs ND DO Edinburgh London New York Oxford Philadelphia St Louis Sydney Toronto 2008 © 2008, Elsevier Limited. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior per- mission of the Publishers. Permissions may be sought directly from Elsevier’s Health Sciences Rights Department, 1600 John F. Kennedy Boulevard, Suite 1800, Philadelphia, PA 19103-2899, USA: phone: (+1) 215 239 3804; fax: (+1) 215 239 3805; or, e-mail: [email protected]. You may also com- plete your request on-line via the Elsevier homepage (http://www.elsevier.com), by selecting ‘Support and contact’ and then ‘Copyright and Permission’. -

Special Report Vein of Galen Aneurysms
Special Report Vein of Galen Aneurysms: A Review and Current Perspective Michael Bruce Horowitz, Charles A. Jungreis, Ronald G. Quisling, and lan Pollack The term vein of Galen aneurysm encom the internal cerebral vein to form the vein of passes a diverse group of vascular anomalies Galen (4). sharing a common feature, dilatation of the vein Differentiation of the venous sinuses occurs of Galen. The name, therefore, is a misnomer. concurrently with development of arterial and Although some investigators speculate that vein venous drainage systems. By week 4, a primi of Galen aneurysms comprise up to 33% of gi tive capillary network is drained by anterior, ant arteriovenous malformations in infancy and middle, and posterior meningeal plexi (3, 4). childhood ( 1), the true incidence of this a nom Each plexus has a stem that drains into one of aly remains uncertain. A review of the literature the paired longitudinal head sinuses, which in reveals fewer than 300 reported cases since turn drain into the jugular veins ( 3, 4). Atresia of Jaeger et al 's clinical description in 1937 (2). the longitudinal sinuses leads to the develop As we will outline below, our understanding of ment of the transverse and sigmoid sinuses by the embryology, anatomy, clinical presentation, week 7 (3, 4). At birth only the superior and and management of these difficult vascular inferior sagittal, straight, transverse, occipital, malformations has progressed significantly and sigmoid sinuses remain, along with a still over the past 50 years. plexiform torcula (3, 4). On occasion, a tran sient falcine sinus extending from the vein of Embryology and Vascular Anatomy of the Galen to the superior sagittal sinus is seen ( 4). -

A Dictionary of Neurological Signs.Pdf
A DICTIONARY OF NEUROLOGICAL SIGNS THIRD EDITION A DICTIONARY OF NEUROLOGICAL SIGNS THIRD EDITION A.J. LARNER MA, MD, MRCP (UK), DHMSA Consultant Neurologist Walton Centre for Neurology and Neurosurgery, Liverpool Honorary Lecturer in Neuroscience, University of Liverpool Society of Apothecaries’ Honorary Lecturer in the History of Medicine, University of Liverpool Liverpool, U.K. 123 Andrew J. Larner MA MD MRCP (UK) DHMSA Walton Centre for Neurology & Neurosurgery Lower Lane L9 7LJ Liverpool, UK ISBN 978-1-4419-7094-7 e-ISBN 978-1-4419-7095-4 DOI 10.1007/978-1-4419-7095-4 Springer New York Dordrecht Heidelberg London Library of Congress Control Number: 2010937226 © Springer Science+Business Media, LLC 2001, 2006, 2011 All rights reserved. This work may not be translated or copied in whole or in part without the written permission of the publisher (Springer Science+Business Media, LLC, 233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection with reviews or scholarly analysis. Use in connection with any form of information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed is forbidden. The use in this publication of trade names, trademarks, service marks, and similar terms, even if they are not identified as such, is not to be taken as an expression of opinion as to whether or not they are subject to proprietary rights. While the advice and information in this book are believed to be true and accurate at the date of going to press, neither the authors nor the editors nor the publisher can accept any legal responsibility for any errors or omissions that may be made. -
27. Veins of the Head and Neck
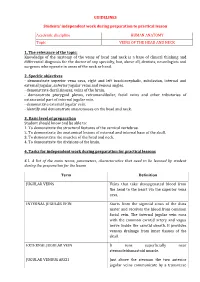
GUIDELINES Students’ independent work during preparation to practical lesson Academic discipline HUMAN ANATOMY Topic VEINS OF THE HEAD AND NECK 1. The relevance of the topic: Knowledge of the anatomy of the veins of head and neck is a base of clinical thinking and differential diagnosis for the doctor of any specialty, but, above all, dentists, neurologists and surgeons who operate in areas of the neck or head. 2. Specific objectives - demonstrate superior vena cava, right and left brachiocephalic, subclavian, internal and external jugular, anterior jugular veins and venous angles. - demonstrate dural sinuses, veins of the brain. - demonstrate pterygoid plexus, retromandibular, facial veins and other tributaries of extracranial part of internal jugular vein. - demonstrate external jugular vein. - identify and demonstrate anastomoses on the head and neck. 3. Basic level of preparation Student should know and be able to: 1. To demonstrate the structural features of the cervical vertebrae. 2. To demonstrate the anatomical lesions of external and internal base of the skull. 3. To demonstrate the muscles of the head and neck. 4. To demonstrate the divisions of the brain. 4. Tasks for independent work during preparation for practical lessons 4.1. A list of the main terms, parameters, characteristics that need to be learned by student during the preparation for the lesson Term Definition JUGULAR VEINS Veins that take deoxygenated blood from the head to the heart via the superior vena cava. INTERNAL JUGULAR VEIN Starts from the sigmoid sinus of the dura mater and receives the blood from common facial vein. The internal jugular vein runs with the common carotid artery and vagus nerve inside the carotid sheath. -

Controversies in the Assessment of Bodily Injury. Institute of Legal Medicine of Catalonia
Controversies in the assessment of bodily injury. Institute of Legal Medicine of Catalonia Centre d’Estudis Jurídics i Formació Especialitzada Institut de Medicina Legal de Catalunya Acknowledgement As ever the contribution of senior management at the Centre for Legal Studies and Specialised Training and the highly professional staff at the Centre’s Legal and Forensic Training Unit has been essen- tial and made it possible to publish the papers about the controversial issues presented below. I would also like to express my appreciation for the enthusiastic collaboration of all the authors referred to in their relevant sections and the computer support provided by Mr. Gabriel Martí Agustí, a psychologist in the Barcelona Forensic Medicine Clin- ic Service, which has made it possible to unify the work of the various authors. All of this has been done at the Institute of Legal Medicine of Catalonia under the supervision of Dr. Jordi Medallo Muñiz who has encouraged, supported and taken part in this project. Finally I would like to mention in particular the ongoing assistance of Dr. Amadeu Pu- jol Robinat, Head of the Forensic Medicine Clinic Service of IMLC. My sincere thanks go to all of them. Dr. Lluïsa Puig Coordinator CONTROVERSIES IN THE ASSESSMENT OF BODILY INJURY. INSTITUTE OF LEGAL MEDICINE OF CATALONIA COORDINATION: DRA. LLUÏSA PUIG BAUSILI Centre d’Estudis Jurídics i Formació Especialitzada Institut de Medicina Legal de Catalunya CONTROVERSIES IN THE ASSESSMENT OF BODILY INJURY. INSTITUTE OF LEGAL MEDICINE OF CATALONIA Centre d’Estudis Jurídics i Formació Especialitzada Institut de Medicina Legal de Catalunya 5 © Generalitat de Catalunya Centre d’Estudis Jurídics i Formació Especialitzada Disclaimer: The contents of this work are licensed under a Attribution-NonCommercial- NoDerivs 3.0 Creative Commons. -

MR Evaluation of Developmental Venous Anomalies: Medullary Venous Anatomy of Venous Angiomas
MR Evaluation of Developmental Venous Anomalies: Medullary Venous Anatomy of Venous Angiomas Charles Lee, Michael A. Pennington, and Charles M. Kenney III PURPOSE: To present characteristic MR findings of developmental venous anomalies (DVAs) in terms of location of caput and draining veins, to correlate these findings with normal medullary venous anatomy, and to suggest an approach to the evaluation of DVAs by means of MR imaging. METHODS: We reviewed the contrast-enhanced MR examinations of 61 patients with DVA, which were selected from 4624 consecutive cranial MR examinations. Site of the DVA and size and direction of draining veins were recorded. RESULTS: Seventy-two DVAs with 78 draining veins were located: 18 were juxtacortical, 13 were subcortical, and 41 were periventricular or deep. Twenty-six of the DVA caputs were frontal, 16 were parietal, 13 were in the brachium pontis/ dentate, seven were in the temporal lobe, three were in the cerebellar hemisphere, three were in the occipital lobe, three were in the basal ganglia, and one was in the pons. The draining veins were superficial in 29 cases and deep in 49. Of the 36 supratentorial deep draining veins, 16 were in the trigone/occipital horn, 11 were in the mid-body of the lateral ventricle, seven were in the frontal horn, and two were in the temporal horn. Among the 14 infratentorial deep draining veins, five were in the lateral recess of the fourth ventricle, four were anterior transpontine veins, three were lateral transpontine veins, and two were precentral cerebellar veins. CONCLUSION: The DVA caputs and their draining veins occurred in typical locations that could be predicted from the normal medullary venous anatomy, with the frontal, parietal, and brachium pontis/dentate being the most common locations. -

Cerebellar Arteriovenous Malformations: Anatomic Subtypes, Surgical Results, and Increased Predictive Accuracy of the Supplementary Grading System
RESEARCH—HUMAN—CLINICAL STUDIES TOPIC RESEARCH—HUMAN—CLINICAL STUDIES Cerebellar Arteriovenous Malformations: Anatomic Subtypes, Surgical Results, and Increased Predictive Accuracy of the Supplementary Grading System BACKGROUND: Anatomic diversity among cerebellar arteriovenous malformations Ana Rodrı´guez-Herna´ndez, (AVMs) calls for a classification that is intuitive and surgically informative. Selection tools MD* like the Spetzler-Martin grading system are designed to work best with cerebral AVMs Helen Kim, MPH, PhD‡§¶ but have shortcomings with cerebellar AVMs. Tony Pourmohamad, MA‡¶ OBJECTIVE: To define subtypes of cerebellar AVMs that clarify anatomy and surgical William L. Young, MD*‡¶k management, to determine results according to subtypes, and to compare predictive Michael T. Lawton, MD*¶ accuracies of the Spetzler-Martin and supplementary systems. METHODS: From a consecutive surgical series of 500 patients, 60 had cerebellar AVMs, for the University of California, 39 had brainstem AVMs and were excluded, and 401 had cerebral AVMs. San Francisco Arteriovenous RESULTS: Cerebellar AVM subtypes were as follows: 18 vermian, 13 suboccipital, Malformation Study Project 12 tentorial, 12 petrosal, and 5 tonsillar. Patients with tonsillar and tentorial AVMs fared , *Department of Neurological Surgery; ‡De- best. Cerebellar AVMs presented with hemorrhage more than cerebral AVMs (P .001). partments of Anesthesia and Perioperative Cerebellar AVMs were more likely to drain deep (P = .04) and less likely to be eloquent Care; §Department of Epidemiology and (P , .001). The predictive accuracy of the supplementary grade was better than that of Biostatistics; ¶Center for Cerebrovascular Research; kDepartment of Neurology, Uni- the Spetzler-Martin grade with cerebellar AVMs (areas under the receiver-operating versity of California, San Francisco, San characteristic curve, 0.74 and 0.59, respectively).