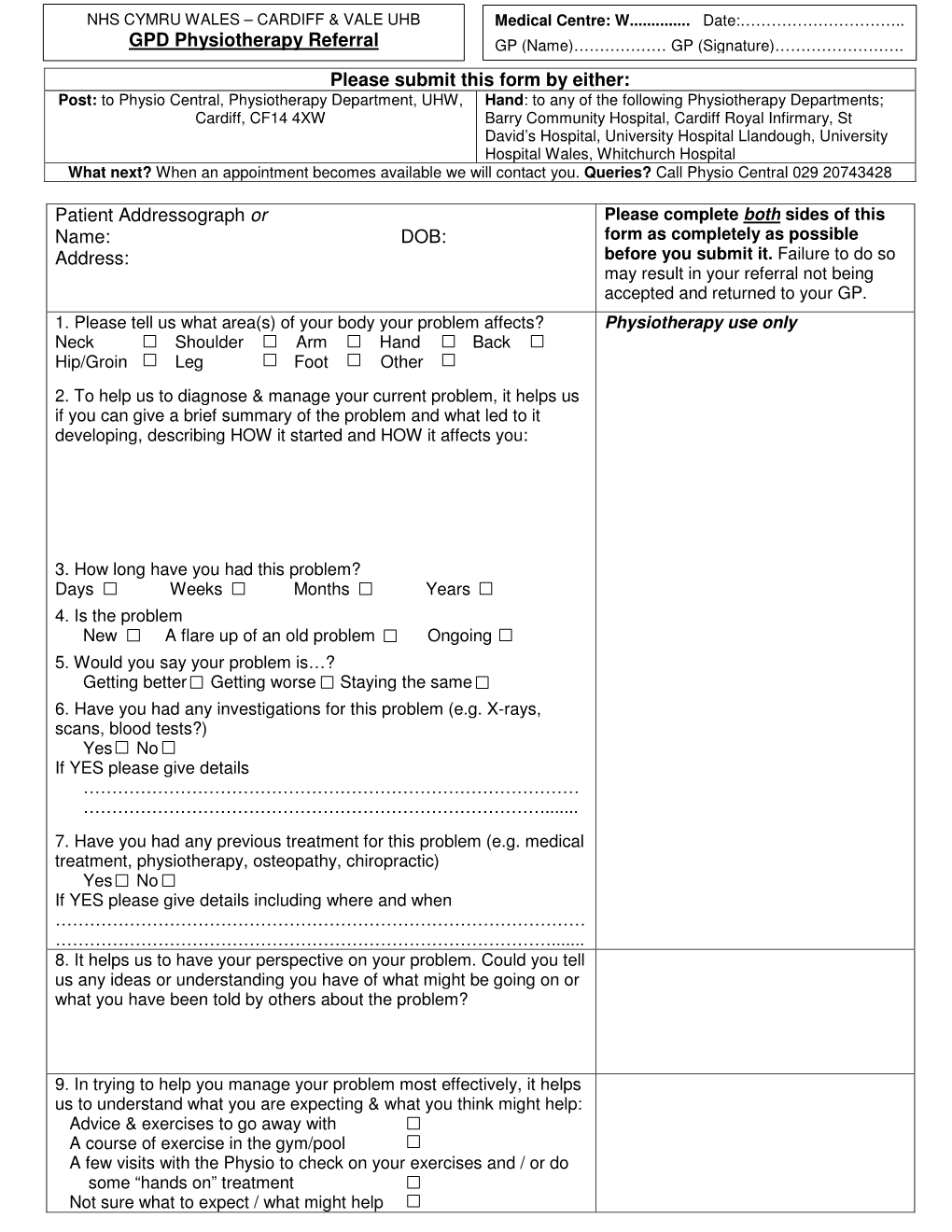
GPD Physiotherapy Referral GP (Name)……………… GP (Signature)……………………
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

29 June CARDIFF UNIVERSITY, GLAMORGAN BUILDING 09.00 Registration and Coffee (Sign up for Afternoon Activities)
29 June CARDIFF UNIVERSITY, GLAMORGAN BUILDING 09.00 Registration and coffee (sign up for afternoon activities) 09.45 COUNCIL CHAMBER: Conference welcome, the Challenging History network 09.50 COUNCIL CHAMBER: Opening Provocation: David Anderson, Director General, Amgueddfa Cymru - National Museum Wales. ‘Avoiding Challenging History’ 10.05 COUNCIL CHAMBER: Keynote: Samantha Heywood, Director, Museum of World War II, Boston. ‘The challenges of challenging history in the ‘real’ world’ [Chair: Sam Cairns] Samantha Heywood worked at Imperial War Museums for twenty years, starting out as an education officer and, by 2015, as the director of public programmes. During this time, she led IWM’s piloting of Inspiring Learning for All and the nation-wide learning programme, Their Past Your Future; worked on the development of IWM North, and led the teams in creating the new Atrium and First World War Galleries at IWM London that opened in 2014. She has worked closely with the ambitions of central government and Lottery funders and yet has delivered thoughtful and focused programmes with their backing. She is currently working in the USA with a project to build a new museum of World War II. 10.50 Coffee in Glamorgan Coffee Shop 11.10 PAPERS 1, CC: Difficult Objects PAPERS 2, 0.85: Re-imagining PAPERS 3, 0.86: Questioning [Chair: Joanne Sayner] commemoration professional practice [Chair: Alex Drago] [Chair: Miranda Stearn] Objects in their rightful place: the case of the potential return of ‘Being There’: an exploration of The Role of Academics in -

GLAMORGAN ARCHIVES JOINT COMMITTEE 11 September 2020 REPORT for the PERIOD 1 May 2020 - REPORT OF: 31 August 2020
THE CITY AND COUNTY OF CARDIFF, COUNTY BOROUGH COUNCILS OF BRIDGEND, CAERPHILLY, MERTHYR TYDFIL, RHONDDA CYNON TAF AND THE VALE OF GLAMORGAN AGENDA ITEM NO THE GLAMORGAN ARCHIVES JOINT COMMITTEE 11 September 2020 REPORT FOR THE PERIOD 1 May 2020 - REPORT OF: 31 August 2020 THE GLAMORGAN ARCHIVIST 1. PURPOSE OF REPORT This report describes the work of Glamorgan Archives for the period 1 May 2020 to 30 August 2020. 2. BACKGROUND As part of the agreed reporting process the Glamorgan Archivist updates the Joint Committee quarterly on the work and achievements of the service. Members are asked to note the content of this report. 3. ISSUES A. MANAGEMENT OF RESOURCES 1. Staff Maintain establishment Virtual tea breaks continue to be held to ensure good communication between staff who have returned to the office and those still working from home. Continue skill sharing and volunteer programme Throughout lockdown regular contact has been maintained with volunteers through weekly emails. Since staff have returned to the office this has been extended to include fortnightly catch ups via Zoom. Zoom video conferencing software was chosen over other available options as it was already being used by the volunteers involved. The annual volunteer feedback sessions have been held, a form being circulated to all volunteers with optional telephone call follow up if requested. The vast majority of responses were positive: I enjoy the atmosphere, the people, the project, and the unlimited coffee I feel valued as a volunteer...All the staff in the Archives are very friendly and helpful, and it is a pleasure to attend every week I have enjoyed all aspects of the project I enjoy the contact with the staff and fellow volunteers and keeping my mind active Can’t think of anything [to improve the placements]. -

Gwaith Achos Cangen Benderfyniadau
GWAITH ACHOS CANGEN BENDERFYNIADAU CYNLLUNIO LLYWODRAETH CYMRU WELSH GOVERNMENT PLANNING DECISIONS BRANCH CASEWORK Mae’r tabl isod yn rhoi cofnod o’r gwaith achos cynllunio a gwaith perthnasol sydd o flaen Gweinidogion Cymru ar hyn o bryd. Mae’r tabl yn cynnwys gwaith achos sydd ‘ar- waith’ a heb eu penderfynu, yn ogystal a achosion sydd wedi eu penderfynu yn ddiweddar. Dim ond achosion sydd wedi eu penderfynu o fewn y 6 wythnos diwethaf sydd wedi eu cynnwys. Mae’r achosion wedi eu harddangos yn ôl y math o achos, ac yna yn ôl y drefn gronolegol cafodd yr achos ei dderbyn. Mae geirfa o’r termau a ddefnyddir ar waelod y tabl. The table below records the planning and related casework that is currently before the Welsh Ministers. The table includes ‘live’ cases yet to be determined and also recently determined cases. Only cases that have been determined within the past 6 weeks are included. The cases are shown by case type and thereafter in chronological order of the date the case was received. A glossary of terms used is provided at the end of the table. Dyddiad Rhif Math o Achos / Case Awdurdod Cynnig / Datblygiad Arfaethedig / Proposal / Safle / Site Location Sefyllfa Dyddiad Derbyn / Date Achos Type Cynllunio / LPA Area Proposed Development Bresennol / Cyhoeddwyd Received / Case Current / Date Issued ID Position 02/08/2012 320 Call In Request Carmarthenshire Construction of a New Eco Park, comprising a Land off the Avenue, Awaiting Sight (Planning) network of footpaths, ponds and landscaping Machynys Mound, of LPA including the outlining of the former Machynys Llanelli, Carmarthenshire. -

June 17, 2020 Dear Constituent Thank You Very Much for Taking the Time To
June 17, 2020 Dear constituent Thank you very much for taking the time to write to me about the Velindre Cancer Centre plans and the ‘Save the Northern Meadows’ campaign. As the Member of the Senedd for Cardiff North I have given careful consideration to constituents’ views on the planning application by Cardiff and Vale Health Board (20/00357/MJR) to build housing on the northern meadows in Whitchurch and I have come to the conclusion that I must oppose the extension of this planning permission. I have never believed that there should be housing on this land. I opposed proposals to build housing on it in 1995, in 1997, 1998 and in 1999 I spoke out against building housing on the land at a public inquiry. I have always supported the development of a new cancer hospital and that is still my priority, and I believe it is the priority for the vast majority of my constituents. One in two of us will need treatment for cancer in our lifetimes. Anyone who has ever needed treatment at or visited Velindre knows that the hardworking staff and very ill patients desperately need a new building. I believe supporting it is the right thing to do. Having now seen some of Velindre’s vision for the site, I really believe it will be therapeutic for those patients who are desperately sick to be surrounded by nature in a building which incorporates as many natural elements as possible and blends into the landscape. The design ideas I’ve seen would mean a building akin to the light and calm of Maggie’s (the cancer support centre) – it will be poles apart from the concrete high-rise blocks of UHW at the Heath. -

Whitchurch Market Town Profile
Whitchurch Market Town Profile Autumn 2017 1 INFORMATION, INTELLI GENCE & INSIGHT TEAM Contents Section Page Introduction 3 Local Politics 5 Demographics 7 Economy 13 Tourism & Leisure 29 Health 32 Housing 36 Education 41 Transport & Infrastructure 42 Community Safety 43 Additional Information 45 2 INFORMATION, INTELLI GENCE & INSIGHT TEAM Phone: 0345 678 9000 Email: [email protected] Market Town Profile Whitchurch Whitchurch is the northern most market town in Shropshire located on the border of Cheshire and Wales. The town has been inhabited since Roman times and is still a thriving market town. This North Shropshire market town has many buildings dating from Medieval ,Tudor and Georgian times. Whitchurch is amongst the oldest continually inhabited towns in the county. Within the town is the wooded Victoria Jubilee Park and picturesque Memorial Garden. Named Mediolanum by the Romans and chosen for its strategic location, Whitchurch soon had legions passing through to reach the outposts of Roman Britain. The town was the heart of the Roman road network, a fact reflected today, and one that makes Whitchurch so central and accessible for visitors. The Whitchurch firm of J B Joyce (tower clock makers) was established in 1690. Whitchurch Heritage Centre hosts information on J B Joyce for visitors. These clocks have an international reputation and can be found on cathedrals and palaces from Singapore to Kabul. Many examples of Joyce’s work can be seen around the town making Whitchurch “the Home of Tower Clocks”. The town is surrounded by beautiful countryside and there are walks along the North Shropshire Canals to Grindley Brook and through the Whitchurch Waterways County Park, also a haven for wildlife and containing Greenfields Nature Reserve managed by The Wildlife Trust. -
Service Framework to Meet the Needs of People with Domestic Abuse and Substance Misuse Problems
Service Framework to meet the needs of people with Domestic Abuse and Substance Misuse Problems ISBN 978 0 7504 5094 2 © Crown copyright April 2009 CMK-22-04-045(251) D7310809 Contents Summary 2 Models of Joint Working between Substance Misuse 3 and Domestic Abuse services Service Aims and Objectives 4 Service Standards 5 Access to Refuges 6 Other Services 6 Child Protection Issues 7 Education and Awareness for Children 7 Protection of Vulnerable Adults 8 Multi Agency Risk Assessment Conference (MARAC) 8 Wales Integrated In-depth Substance Misuse Assessment 9 Toolkit (WIISMAT) Groups with Special Needs 9 Perpetrators 9 Needs Assessment and Service Planning 10 Care Pathway 11 Directory of Services 11 Training and Qualifications 11 Appendices Integrated care pathway referral flow chart 13 Directory of domestic abuse service providers in Wales 15 Directory of substance misuse service providers in Wales 29 Glossary 43 All Wales Domestic Abuse 24 hour free telephone helpline 0808 80 10 800 1 A Service Framework to Meet the Needs of People with Domestic Abuse and Substance Misuse Problems Summary It is the priority of the Welsh Assembly Government to reduce the harm to individuals and their families from the increasing problems of domestic abuse and the misuse of drugs and alcohol. It is the aim of this framework to assist domestic abuse and substance misuse planners, commissioners and providers to establish robust links between Domestic Abuse and Substance Misuse services which will provide a seamless care pathway for all clients. It also makes reference to issues with identified domestic abuse perpetrators. Evidence shows that of the 4391 calls to the Wales Domestic Abuse Helpline 387 (9%) have disclosed substance misuse. -
Statute Law Repeals: Nineteenth Report
The Law Commission and The Scottish Law Commission (LAW COM No 333) (SCOT LAW COM No 227) STATUTE LAW REPEALS: NINETEENTH REPORT DRAFT STATUTE LAW (REPEALS) BILL Presented to the Parliament of the United Kingdom by the Lord Chancellor and Secretary of State for Justice by Command of Her Majesty Laid before the Scottish Parliament by the Scottish Ministers April 2012 Cm 8330 £xx.xx SG/2012/39 ii The Law Commission and the Scottish Law Commission were set up by the Law Commissions Act 1965 for the purpose of promoting the reform of the law. The Law Commissioners are: The Right Honourable Lord Justice Munby, Chairman Professor Elizabeth Cooke Mr David Hertzell Professor David Ormerod Miss Frances Patterson QC. The Chief Executive of the Law Commission is Elaine Lorimer. The Law Commission is located at Steel House, 11 Tothill Street, London SW1H 9LJ The Scottish Law Commissioners are: Laura J Dunlop QC Patrick Layden QC, TD Professor Hector L MacQueen Dr Andrew J M Steven The Chief Executive of the Scottish Law Commission is Malcolm McMillan. The Scottish Law Commission is located at 140 Causewayside, Edinburgh, EH9 1PR. The terms of this report were agreed on 7 March 2012. The text of this report is available on the Internet at: http://www.lawcom.gov.uk (See Publications > Statute Law Repeals reports) http://www.scotlawcom.gov.uk/law-reform-projects/joint-projects/statute-law-repeals iii LAW COMMISSION SCOTTISH LAW COMMISSION STATUTE LAW REPEALS: NINETEENTH REPORT DRAFT STATUTE LAW (REPEALS) BILL CONTENTS Paragraph Page REPORT 1 APPENDIX -
1 Listados Provisionales De Los Puntos De Acceso
LISTADOS PROVISIONALES DE LOS PUNTOS DE ACCESO NORMALIZADOS DE ENTIDADES CORPORATIVAS, ENTIDADES GEOGRÁFICAS, ONOMÁSTICOS, PRODUCTORES DE DOCUMENTOS, DESTINATARIOS DE SERIES DOCUMENTALES EPISTOLARES Y MATERIAS EN EL SISTEMA DE DESCRIPCIÓN DEL FONDO DOCUMENTAL "JUAN NEGRÍN LÓPEZ". CENTRO DE ARCHIVO "FUNDACIÓN JUAN NEGRÍN". LAS PALMAS DE GRAN CANARIA, ESPAÑA. Listado de entidades. 7 Fechas (revista) ABC (diario) Abeilles (Escuela, Francia) Academía de Ciencias de la Unión Socialista de Repúblicas Soviéticas Academia Nacional de Medicina de Venezuela Academia Nacional de Medicina de Venezuela. Cátedra de Fisiología Acció Catalana Acció Catalana (en el exilio) Acción Católica Española Acción Católica Española. Ecclesia Acción Católica Italiana Acción Nacionalista Vasca Aceros comerciales y construcciones, Sociedad Anónima Acuerdos de Múnich Adlerd Berthold (compañía) Aéroplanes Morane-Saulnier Aeropuerto de Gando Aeropuerto de Madrid-Cuatro Vientos African Mariner (barco) Agence Espagne Agence France-Presse Agencia Aduanal Noguerira Mendoza Agencia EFE Agencia Navas Agencia Tass Agenzia Stefani Agfa-Gevaert Agfa-Lupex Agrupación de Socialistas Españoles en México Agrupación de Socialistas Españoles en México. Presidente Agrupación de Socialistas Españoles en México. Secretario Agrupación de Socialistas Españoles en México. Vicepresidente Agrupación de Socialistas Españoles en México. Vocal 1 Agrupación de Universitarios Españoles Agrupación de Universitarios Españoles. Junta Directiva Central Agrupación de Universitarios Españoles. Presidente Agrupación de Universitarios Españoles. Secretario General Agrupación de Universitarios Españoles. Tesorero Agrupación de Universitarios Españoles. Vice-secretario Agrupación de Universitarios Españoles. Vocal de estudios políticos Agrupación de Universitarios Españoles. Vocal de organización Agrupación de Universitarios Españoles. Vocal de propaganda Agrupación de Universitarios Españoles. Vocal de relaciones Agrupación Nacional de Abogados Socialistas de España Agrupación Nacional de Abogados Socialistas de España. -
Useful Information for You and Your Visitors
Information folder if Useful information for you and your visitors Please leave this folder for the next patient Contents About Cardiff and Vale University Health Board 1. Your stay in hospital • Care, dignity and respect • Who is who? • Uniforms • Giving consent • Mental capacity • Patient confidentiality • Your Health Records • Good communication • Personal safety • Volunteers 2. What you will need in hospital 3. What NOT to bring into hospital 4. On the ward • Ward rounds • Nurse rounds • Visiting hours • Moving Wards • Phones and other electronic devices • Free Wi-Fi 5. Keeping well in hospital • Preventing infections • Medication • Eating and drinking well • Sleeping • Slips, trips and falls • Flowers • Smoke free hospitals 1 6. Hospital Facilities • Trolley Service • Restaurants • Spiritual and Pastoral Support • Help for Carers • Information and Support Centres • Cash Points 7. Going home 8. How was your stay? • Paying a compliment • Making a complaint 9. Charitable Gifts 10. Car parking 11. Travel information 2 About Cardiff and Vale University Health Board Welcome to Cardiff and Vale University Health Board. Cardiff and Vale University Health Board is one of the largest NHS organisations in Wales. We provide day to day health services to a population of around 478,900 people living in Cardiff and the Vale of Glamorgan. This includes emergency and planned hospital treatment, care in people's homes and community clinics and mental health care. We also serve a wider population across South and Mid Wales for a range of specialties. We are a teaching health board so during your stay students may be involved in your care. If you are concerned about this or any aspect of your stay with us please ask any of the clinical staff looking after you. -

University of Wales Trinity Saint David the Development of the Glamorgan
University of Wales Trinity Saint David The Development of the Glamorgan County Lunatic Asylum and Mental Hospital 1830-1930 Denzil Jones MPhil 2017 DECLARATION SHEET This sheet MUST be signed and included within the thesis This work has not previously been accepted in substance for any degree and is not being currently submitted in candidature for any degree. Signed……D H Jones…………………………………………………………… (student) Date………24 July 2017………………………………………………………… STATEMENT 1 This thesis is the result of my own investigations, except where otherwise stated. Where correction services have been used the extent and nature of the correction is clearly marked in a footnote(s). Other sources are acknowledged by footnotes giving explicit references. A bibliography is appended. Signed………D H Jones…………………………………………………………… (student) Date…………24 July 2017……………………………………………………… STATEMENT 2 I hereby give consent for my thesis, if accepted, to be available for photocopying and for inter library loan, and for the title and summary to be made available to outside organisations. Signed………D H Jones………………………………………………………….. (student) Date…………24 July 2017…………………………………………………… STATEMENT 3 I hereby give consent for my dissertation, if accepted, to be available for deposit in the University’s digital repository. Signed…………D H Jones……………………………………………… ………. (student) Date……………24 July 2017…………………………………………………………………………………………… NB Students on whose behalf a bar on access has been approved by the University, should use the following version of Statement 2: I hereby give consent for my -
Footfalls Echo in the Memory
Verner C. Bickley, after the University of Cardiff and service in the Royal Navy in India and Ceylon (Sri Lanka), joined the British Colonial Service and served as an Education Officer in Singapore before joining the British Council in Burma and Indonesia. He later returned to the Overseas Service as Director of the Hong Kong Government’s Institute of Language. He is an Honorary Research Fellow at the University of Hong Kong and Chairman of the English-Speaking Union, Hong Kong. FOOTFALLS ECHO IN THE MEMORY A Life with the Colonial Education Service and the British Council in Asia Verner C. Bickley The Radcliffe Press LONDON • NEW YORK To Gillian for her patience and love Supported by Hong Kong Arts Development Council fully supports freedom of artistic expression. The views and opinions expressed in this project do not represent the stand of the Council. Published in 2010 by Radcliffe Press An Imprint of I.B.Tauris & Co. Ltd 6 Salem Road, London W2 4BU 175 Fifth Avenue, New York NY 10010 www.ibtauris.com Distributed in the United States and Canada Exclusively by Palgrave Macmillan, 175 Fifth Avenue, New York NY 10010 Copyright © Verner C. Bickley 2010 All illustrations © Verner C. Bickley 2010, except the photographs of the staff of Altrincham Grammar School and of the School Scout Hut The right of Verner C. Bickley to be identified as the author of this work has been asserted by him in accordance with the Copyright, Designs and Patents Act, 1988. All rights reserved. Except for brief quotations in a review, this book, or any part thereof, may not be reproduced, stored in or introduced into a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior written permission of the publisher. -
Statute Law Repeals: Nineteenth Report
The Law Commission and The Scottish Law Commission (LAW COM No 333) (SCOT LAW COM No 227) STATUTE LAW REPEALS: NINETEENTH REPORT DRAFT STATUTE LAW (REPEALS) BILL Presented to the Parliament of the United Kingdom by the Lord Chancellor and Secretary of State for Justice by Command of Her Majesty Laid before the Scottish Parliament by the Scottish Ministers April 2012 Cm 8330 £xx.xx SG/2012/39 ii The Law Commission and the Scottish Law Commission were set up by the Law Commissions Act 1965 for the purpose of promoting the reform of the law. The Law Commissioners are: The Right Honourable Lord Justice Munby, Chairman Professor Elizabeth Cooke Mr David Hertzell Professor David Ormerod Miss Frances Patterson QC. The Chief Executive of the Law Commission is Elaine Lorimer. The Law Commission is located at Steel House, 11 Tothill Street, London SW1H 9LJ The Scottish Law Commissioners are: Laura J Dunlop QC Patrick Layden QC, TD Professor Hector L MacQueen Dr Andrew J M Steven The Chief Executive of the Scottish Law Commission is Malcolm McMillan. The Scottish Law Commission is located at 140 Causewayside, Edinburgh, EH9 1PR. The terms of this report were agreed on 7 March 2012. The text of this report is available on the Internet at: http://www.lawcom.gov.uk (See Publications > Statute Law Repeals reports) http://www.scotlawcom.gov.uk/law-reform-projects/joint-projects/statute-law-repeals iii LAW COMMISSION SCOTTISH LAW COMMISSION STATUTE LAW REPEALS: NINETEENTH REPORT DRAFT STATUTE LAW (REPEALS) BILL CONTENTS Paragraph Page REPORT 1 APPENDIX