Maternal Mortality
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -

Ltzt Ul/Alsf Uxgtf -K|Ltzt Affs Nifd0fk'/, G/}Gfk'/, S7s'oof, Sfnfkmf6f
1 2 lhNnfx?sf] ul/aLsf] b/, ul/aLsf] ljifdtf / ul/aLsf] uxgtf @)^* lhNnf uf=lj=;=sf gfd ul/aLsf b/ ul/aLsf ljifdtf ul/aLsf uxgtf -k|ltzt_ -k|ltzt_ -k|ltzt_ afFs nIfd0fk'/, g/}gfk'/, s7s'Oof, sfnfkmf6f 56.46(10.17) 16.88(4.71) 6.8(2.36) afFs kmQ]k'/, lagf}gf 39.35(10.08) 9.88(3.57) 3.53(1.55) afFs d6]lxof, u+ufk'/ 57.98(9.77) 17.65(4.76) 7.2(2.47) afFs a}hfk'/, vf;s'Zdf 33.01(9.93) 7.52(3.07) 2.49(1.22) afFs sGrgk'/ 25.26(8.58) 5.33(2.37) 1.67(0.88) afFs dxfb]jk'/L 18.17(7.47) 3.62(1.9) 1.1(0.67) afFs sf]xnk'/ 12.48(4.8) 2.59(1.25) 0.81(0.45) afFs /em]gf 10.56(4.91) 2.02(1.17) 0.59(0.4) afFs zD;]/u~h 28.96(8.92) 6.92(2.92) 2.4(1.23) afFs u+ufk'/ 41.53(10.17) 10.8(3.7) 3.96(1.64) afFs sDbL 37.03(9.74) 9.65(3.48) 3.57(1.54) afFs dlgsfk'/ 21.98(6.69) 5.21(2.09) 1.8(0.86) afFs ags66L 47.84(9.58) 13.46(4.05) 5.2(1.94) afFs a]txgL 58.1(10.14) 17.37(4.79) 6.98(2.42) afFs xf]lnof 66.99(9.02) 22.33(5.27) 9.66(2.96) afFs k'/}gL, pbok'/ k'/}gf 40.52(9.93) 10.57(3.7) 3.88(1.66) afFs a;'b]jk'/ 23.52(7.13) 5.36(2.11) 1.79(0.83) afFs vf;sf/sf+bf] 9.42(3.62) 1.97(0.96) 0.62(0.35) afFs lkk/xjf, ejfgLk'/ 34.43(9.16) 8.42(3.11) 2.96(1.32) afFs lxl/ldlgof 42.28(10.72) 10.85(3.92) 3.93(1.73) afFs ags6jf 19.47(7.35) 4.12(2.01) 1.31(0.76) afFs lr;fkfgL 18.44(6.32) 3.93(1.72) 1.26(0.65) afFs gf}j:tf 22.23(7.75) 4.8(2.18) 1.55(0.83) afFs l6l6lx/Lof 23.97(8.41) 5.15(2.4) 1.65(0.92) afFs /lgofk'/ 36.22(9.38) 9.01(3.39) 3.2(1.49) afFs l;tfk'/ 11.86(5.22) 2.34(1.28) 0.71(0.45) afFs ;f]gk'/ 36.36(9.79) 8.96(3.35) 3.16(1.43) afFs p9/fk'/ 37.83(10.01) 9.42(3.46) 3.35(1.48) afFs a]nef/, ;fOufpF 45.89(9.99) 12.47(4.01) 4.71(1.87) afFs k/;k'/ 27.7(8.75) 6.62(2.82) 2.3(1.18) afFs /fwfk'/ 5.57(3.21) 0.95(0.63) 0.26(0.2) afFs afu]Zj/L 8.67(3.98) 1.62(0.9) 0.47(0.3) afFs sh'/fv'b{, OGb|k'/, a]nx/L 34.1(8.42) 8.57(2.95) 3.08(1.28) afFs g]kfnu+h gu/kflnsf 9.65(3.35) 2.17(0.93) 0.73(0.36) gf]6 M sf]i7s -_ leq /x]sf] c+sn] ;DalGwt ;"rssf] e|dfz+ -k|ltzt_ nfO{ hgfpF5 . -

Strengthening the Role of Civil Society and Women in Democracy And
HARIYO BAN PROGRAM Monitoring and Evaluation Plan 25 November 2011 – 25 August 2016 (Cooperative Agreement No: AID-367-A-11-00003) Submitted to: UNITED STATES AGENCY FOR INTERNATIONAL DEVELOPMENT NEPAL MISSION Maharajgunj, Kathmandu, Nepal Submitted by: WWF in partnership with CARE, FECOFUN and NTNC P.O. Box 7660, Baluwatar, Kathmandu, Nepal First approved on April 18, 2013 Updated and approved on January 5, 2015 Updated and approved on July 31, 2015 Updated and approved on August 31, 2015 Updated and approved on January 19, 2016 January 19, 2016 Ms. Judy Oglethorpe Chief of Party, Hariyo Ban Program WWF Nepal Baluwatar, Kathmandu Subject: Approval for revised M&E Plan for the Hariyo Ban Program Reference: Cooperative Agreement # 367-A-11-00003 Dear Judy, This letter is in response to the updated Monitoring and Evaluation Plan (M&E Plan) for the Hariyo Program that you submitted to me on January 14, 2016. I would like to thank WWF and all consortium partners (CARE, NTNC, and FECOFUN) for submitting the updated M&E Plan. The revised M&E Plan is consistent with the approved Annual Work Plan and the Program Description of the Cooperative Agreement (CA). This updated M&E has added/revised/updated targets to systematically align additional earthquake recovery funding added into the award through 8th modification of Hariyo Ban award to WWF to address very unexpected and burning issues, primarily in four Hariyo Ban program districts (Gorkha, Dhading, Rasuwa and Nuwakot) and partly in other districts, due to recent earthquake and associated climatic/environmental challenges. This updated M&E Plan, including its added/revised/updated indicators and targets, will have very good programmatic meaning for the program’s overall performance monitoring process in the future. -

The Nepal Smallholder Irrigation Market Initiative (SIMI) WINROCK/IDE/CEAPRED/SAPPROS
Increasing Rural Income through Micro Irrigation & Market Integration The Nepal Smallholder Irrigation Market Initiative (SIMI) WINROCK/IDE/CEAPRED/SAPPROS USAID Cooperative Agreement No. 367-A-00-03-00116-00 Nepal SIMI Annual (Fourth Quarter) Performance Report 2005 July 1, 2004 – June 30, 2005 (F.Y. 2004/5) Nepal SIMI Performance Report No. 8 Mailing Address GPO 8975, EPC 2560, Bakhundol, Lalitpur Tel: (977-1) 5535565 Fax: 5520846 E-mail: [email protected] Table of Contents 1.0 Background…………………………………………………………………………..1 1.1 SIMI goals………………………………………………………………………...2 1.2 Partners…………………………………………………………………………...2 2.0 Expected Results (Output or Indicators)……...……………………………………3 3.0 SIMI Indicator Target Performance………..……………………………….……..3 3.1 Activities………………………………………………………………………..5 3.1.1 Program Mobilization…………………………………………………5 3.1.2 Supply Chain Development……………………………………………5 3.1.3 Social Marketing……………………………………………………….7 3.1.4 Market Development…………………………………………………..7 3.1.5 Collaborative Partnerships and Linkages with Government……….8 3.1.6 Water Source Development…………………………………………...8 3.1.7 Gender Program……………………………………………………….8 3.1.8 Monitoring and Evaluation……………………………………………9 3.1.9 Success Stories………………………………………………………...10 3.1.10 Component wise Highlighted Program……………………………...18 3.2 Activities Planned for the Next Three Months……………………………...30 4.0 Statement of Work………………………………………………………………….31 5.0 Administrative Information………………………………………………………..31 6.0 Financial Information………………………………………………………………33 Annex A Nepal SIMI Project Areas…………………………………………………...34 -
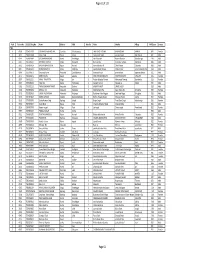
TSLC PMT Result
Page 62 of 132 Rank Token No SLC/SEE Reg No Name District Palika WardNo Father Mother Village PMTScore Gender TSLC 1 42060 7574O15075 SOBHA BOHARA BOHARA Darchula Rithachaupata 3 HARI SINGH BOHARA BIMA BOHARA AMKUR 890.1 Female 2 39231 7569013048 Sanju Singh Bajura Gotree 9 Gyanendra Singh Jansara Singh Manikanda 902.7 Male 3 40574 7559004049 LOGAJAN BHANDARI Humla ShreeNagar 1 Hari Bhandari Amani Bhandari Bhandari gau 907 Male 4 40374 6560016016 DHANRAJ TAMATA Mugu Dhainakot 8 Bali Tamata Puni kala Tamata Dalitbada 908.2 Male 5 36515 7569004014 BHUVAN BAHADUR BK Bajura Martadi 3 Karna bahadur bk Dhauli lawar Chaurata 908.5 Male 6 43877 6960005019 NANDA SINGH B K Mugu Kotdanda 9 Jaya bahadur tiruwa Muga tiruwa Luee kotdanda mugu 910.4 Male 7 40945 7535076072 Saroj raut kurmi Rautahat GarudaBairiya 7 biswanath raut pramila devi pipariya dostiya 911.3 Male 8 42712 7569023079 NISHA BUDHa Bajura Sappata 6 GAN BAHADUR BUDHA AABHARI BUDHA CHUDARI 911.4 Female 9 35970 7260012119 RAMU TAMATATA Mugu Seri 5 Padam Bahadur Tamata Manamata Tamata Bamkanda 912.6 Female 10 36673 7375025003 Akbar Od Baitadi Pancheswor 3 Ganesh ram od Kalawati od Kalauti 915.4 Male 11 40529 7335011133 PRAMOD KUMAR PANDIT Rautahat Dharhari 5 MISHRI PANDIT URMILA DEVI 915.8 Male 12 42683 7525055002 BIMALA RAI Nuwakot Madanpur 4 Man Bahadur Rai Gauri Maya Rai Ghodghad 915.9 Female 13 42758 7525055016 SABIN AALE MAGAR Nuwakot Madanpur 4 Raj Kumar Aale Magqar Devi Aale Magar Ghodghad 915.9 Male 14 42459 7217094014 SOBHA DHAKAL Dolakha GhangSukathokar 2 Bishnu Prasad Dhakal -
STRIDE Service Coverage Assessment USAID, Nepal
STRIDE Service Coverage Assessment USAID, Nepal Order number: AID-367-O-16-00004 March 12, 2017 Anders Eklund Worldwide Rehabilitation Ltd. EXECUTIVE SUMMARY Nepal, like other countries in the region, has a substantial number of people who need physical rehabilitation. The 10-year civil conflict and the earthquake in April 2015 contributed to increasing that need. The Strengthening Rehabilitation in District Environs (STRIDE) program seeks to ensure that sustainable, accessible and quality physical rehabilitation services and community-based follow-up are provided for people with physical disabilities. The program is funded by the United States Agency for International Development (USAID) and implemented by Handicap International (HI) with sub-awards to five physical rehabilitation centers (PRCs) in four of the country's five regions. It was launched in January 2010 and is now in its second three-year extension (ending in January 2019). STRIDE plays an important role in the Nepali rehabilitation sector. To date, STRIDE PRCs have successfully provided physical rehabilitation services to more than 40,000 persons, including the delivery of more than 7200 prostheses and orthoses, 1200 wheelchairs and 4300 mobility aids. Services are normally center-based, but are also provided through outreach rehabilitation camps and field visits (so far reaching 52 of Nepal's 75 districts), with community disability workers (CDWs) conducting follow-up in the field. The main question that the present service coverage assessment sets out to answer is to what degree the physical rehabilitation services in Nepal, and in particular those of the five STRIDE PRCs, are able to meet the country's rehabilitation needs. -

Hariyo Ban Program Ii Threats and Vulnerabilities
HARIYO BAN PROGRAM II (2016-2021) THREATS AND VULNERABILITIES ASSESSMENT OF PARKS AND CORRIDORS OF TERAI ARC LANDSCAPE Prepared by: WWF in partnership with CARE, FECOFUN and NTNC P.O. Box 7660 Kathmandu, Nepal 21 April 2017 © WWF 2017 All rights reserved Any reproduction of this publication in full or in part must mention the title and credit WWF. Published by WWF Nepal PO Box: 7660 Baluwatar, Kathmandu, Nepal T: +977 1 4434820, F: +977 1 4438458 [email protected] , www.wwfnepal.org/hariyobanprogram Disclaimer This Threats and Vulnerabilities Assessment of Parks and Corridors in Terai Arc Landscape is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government. Contents INTRODUCTION ........................................................................................................................................................5 METHODOLOGY ........................................................................................................................................................6 Chitwan National Park and Buffer Zone ...................................................................................................................7 Threat Ratings of Chitwan National Park and Buffer Zone...................................................................................8 Barandabhar Corridor ........................................................................................................................................... -

Initial Environmental Examination
Initial Environmental Examination May 2017 NEP: Regional Urban Development Project Drainage and Road Construction and Improvement Works at Nepalgunj Sub- metropolitan City CURRENCY EQUIVALENTS as of 28 January 2017 Currency unit – Nepalese Rupee (NRS) NRe1.00 = $ 0.0092 $1.00 = NRs108.67 ABBREVIATIONS 3R reduce, reuse, and recycle AAPA Aquatic Animals Protection Act ADB Asian Development Bank CBS Central Bureau of Statistics CFUG Community Forest Users Group CITES Convention on International Trade of Endangered Species of Wild Fauna and Flora DADO District Agriculture Development Office DDC District Development Committee DEECCU District Energy, Environment and Climate Change Unit DFO District Forest Office DIZ Direct Impact Zone DMC Developing Member Country DSC Design and Supervision Consultants DUDBC Department of Urban Development and Building Construction DWEC Daily WAGE Execution Committee EARF Environmental Assessment and Review Framework EHS Environment, Health and Safety EIA Environmental Impact Assessment EMAP Environmental Management Action Plan EMEP Environmental Mitigation Execution Plan EMP Environmental Management Plan EPA Environment Protection Act EPM Environmental Protection Measures EPR Environment Protection Rules FGD Focused Group Discussion FWR Far Western Region FWRN Far Western Region of Nepal GDP gross domestic product GFP Grievance Focal Points GHG greenhouse gas GRC Grievance Redress Committee GRC Grievance Redress Cell HDPE High Density Polyethylene Pipe IEC information, education, and communication IEE Initial -

POPULATION STATUS and HABITAT SUITABILITY of SARUS CRANE (Antigone Antigone, Linnaeus, 1758) in BANKE DISTRICT, NEPAL
POPULATION STATUS AND HABITAT SUITABILITY OF SARUS CRANE (Antigone antigone, Linnaeus, 1758) IN BANKE DISTRICT, NEPAL SHRADDHA TIWARI T.U. Registration No. 5-1-33-471-2005 T.U. Examination Roll No: 050 Batch: 2070/2071 A thesis submitted in partial fulfillment of the requirements for the award of the degree of Master of Science in Zoology with special paper Ecology and Environment. Submitted to Central Department of Zoology Institute of Science and Technology Tribhuvan University Kirtipur, Kathmandu Nepal December, 2016 DECLARATION I hereby declare that the work presented in this thesis has been done by myself, and has not been submitted elsewhere for the award of any degree. All sources of information have been specifically acknowledged by references to the author(s) or institution(s). ……………………… Date: ................................. Ms. Shraddha Tiwari i TRIBHUVAN UNIVERSITY CENTRAL DEPARTMENT OF ZOOLOGY Kirtipur, Kathmandu, Nepal RECOMMENDATION This is to recommend that the thesis entitled “POPULATION STATUS AND HABITAT SUITABILITY OF SARUS CRANE (Antigone antigone, Linnaeus 1758) IN BANKE DISTRICT, NEPAL” has been carried out by Ms. Shraddha Tiwari for the partial fulfillment of Master’s Degree of Science in Zoology with special paper Ecology and Environment. This is her original work and has been carried out under my supervision. To the best of our knowledge, this thesis work has not been submitted for any other degree in any institutions. Date:-………………………………. ………………………………….. Supervisor Nanda Bahadur Singh, PhD Professor Central Department of Zoology Tribhuvan University ii TRIBHUVAN UNIVERSITY CENTRAL DEPARTMENT OF ZOOLOGY Kirtipur, Kathmandu, Nepal RECOMMENDATION This is to recommend that the thesis entitled “POPULATION STATUS AND HABITAT SUITABILITY OF SARUS CRANE (Antigone antigone, Linnaeus 1758) IN BANKE DISTRICT, NEPAL” has been carried out by Ms. -

Nepal EGRP-RFP-FY19-P006
Request for Proposal (RFP) - Nepal EGRP-RFP-FY19-P006 Amendment #1 Commodity/Service Required: Endline Assessment of Early Grade Reading Program (EGRP) Type of Procurement: One Time Purchase Order Type of Contract: Firm Fixed Price Term of Contract: December 01, 2019- April 15, 2020 Contract Funding: AID-367-TO-15-00002 This Procurement supports: USAID’s Early Grade Reading Program (EGRP) Submit Proposal to: The Selection Committee RTI- USAID Early Grade Reading Program House no. 46/64, Uttar Dhoka, Lazimpat, Kathmandu, Nepal Original Date of Issue of RFP: Tuesday, July 23, 2019 Date Questions from Supplier Due: Wednesday, July 31, 2019 11:00 a.m. Nepal Standard Time email [email protected] Note:- Q&A will be posted on RTI website Pre-submission conference on RFP Thursday, August 01, 2019, 10:00 to 11:00 AM at EGRP meeting hall, Lazimpat. Date Proposal Due: Thursday, August 22, 2019, 11:00 a.m. Nepal Standard Time Approximate Purchase Order effective date to December 01, 2019 Successful Bidder(s): Method of Submittal: Hard Copy of proposal along with the soft copy in a CD or pen drive. Proposal documents should be submitted in a closed envelope with wax seal (laah chhap) and clearly marked with the solicitation number to the following address: The Selection Committee RTI-USAID Early Grade Reading Program House no. 46/64, Uttar Dhoka, Lazimpat, Kathmandu, Nepal. Bidder’s quote must be printed on the organization’s letterhead, signed, stamped, dated and must include all items and/or services. In addition, each and every pages of the proposal documents needs to be signed and stamped by the authorized person in order to be considered for evaluation. -

Saath-Saath Project
Saath-Saath Project Saath-Saath Project THIRD ANNUAL REPORT August 2013 – July 2014 September 2014 0 Submitted by Saath-Saath Project Gopal Bhawan, Anamika Galli Baluwatar – 4, Kathmandu Nepal T: +977-1-4437173 F: +977-1-4417475 E: [email protected] FHI 360 Nepal USAID Cooperative Agreement # AID-367-A-11-00005 USAID/Nepal Country Assistance Objective Intermediate Result 1 & 4 1 Table of Contents List of Acronyms .................................................................................................................................................i Executive Summary ............................................................................................................................................ 1 I. Introduction ........................................................................................................................................... 4 II. Program Management ........................................................................................................................... 6 III. Technical Program Elements (Program by Outputs) .............................................................................. 6 Outcome 1: Decreased HIV prevalence among selected MARPs ...................................................................... 6 Outcome 2: Increased use of Family Planning (FP) services among MARPs ................................................... 9 Outcome 3: Increased GON capacity to plan, commission and use SI ............................................................ 14 Outcome -

Download [PDF, 944.81
DIRECTORY OF NATIONAL CENSUS OF MANUFACTURING ESTABLISHMENTS - 2069 S.No. NSIC Name of Establishments VDC/Municipality Name Ward Tole Contact Telephone Code District : 1 Taplejung 1 1701 Chiring Nepali Hate Kagaj Udhyog Phungling 6 Dandabari 9742607349 2 1701 Gorujure Nepali Hate Kagaj Udhyog Sangu 8 Sanghu 3 3100 Mechi Furniture Udhyog Phungling 5 Nayoudang Chok 9842660709 4 3100 Mousami Furniture Udhyog Phungling 4 Naya Road 024-460032 5 3100 Shrestha Furniture Udhyog Phungling 5 Birendrachowk 9842660095 6 1701 Timbung Pokhari Nepali Hate Kagaj Udhyog Kalikhola 9 Syatar 9752608262 District : 2 Panchthar 1 1621 Annapurna Veniar Udhyog Phidim 2 Pallotar 9807937312 2 1079 Kanchangjanga Tea Estate and Research Center Pvt. Ltd. Phidim 3 Suntalabari 024-520169 3 1621 Kanchanjanga Veniar Udhyog Phidim 2 Pallotar 024-520318 4 1312 Pratima Dhaka Kapada Udhyoug Phidim 1 Bazar 9842636831 5 1312 Seling Dhaka Kapada Udhyog Phidim 4 Gadhi 024-520043 6 2391 Shibakala Itta Udhyog Phidim 2 Pallotar 024520357 District : 3 Ilam 1 1079 Aayus Tea Processing Pvt. Ltd. Phikalbazar 6 Phikkal 9842628561 2 1079 Him Shikhar Chiya Prasodhan Udhyog Pvt. Ltd. Mangalbare 1 Manglebare 027400071 3 1079 Himalayan Range Tea Udhyog Pvt. Ltd. Phikalbazar 2 Fikal 027540165 4 1079 Himalayan Sangrila Tea Producers Pvt. Ltd. Sakhejung 7 Nepaltar 027-690111 5 1079 Ilam Chiyabari Pvt. Ltd. Panchakanya 7 Aitebare 027-555180 Page 1 of 183 S.No. NSIC Name of Establishments VDC/Municipality Name Ward Tole Contact Telephone Code 6 1079 Ilam Tea Producers Pvt. Ltd. Panchakanya 2 Aitebare 026-555027/28 7 1621 Ima Jagadamba Industries Sakhejung 7 Nepaltar 9816018342 8 1621 Jaya Bhawani Veniyar Udhyog Maipokhari 2 Puwakhola 9815901263 9 1079 Mechi Valley Chiya Udhyog Pvt.