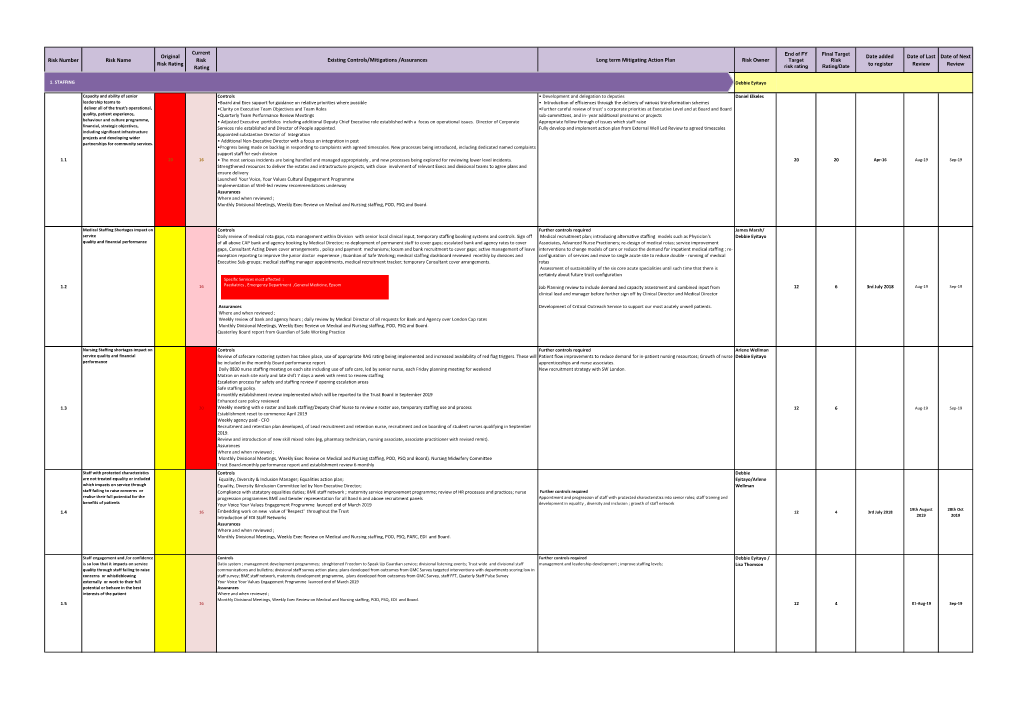
5.1B Corporate Risk Register
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Harvey Tercentenary WILLIAM HARVEY: the MAN and the COLLEGE of PHYSICIANS
Harvey Tercentenary WILLIAM HARVEY: THE MAN AND THE COLLEGE OF PHYSICIANS By K. D. KEELE, M.D., F.R.C.P. Consultant Physician, Ashford Hospital and Staines Hospital IN I578, on i April, Thomas Harvey of Folkestone, and his wife Joan, were blessed with their firstborn often children, William Harvey. This birth took place in a 'faire stone-built house' which later became the post office. At the age of ten the young William was sent to the Grammar School (now the King's School), Canterbury, for his elementary education, whence, at the age of sixteen he was entered as a pensioner of Caius College, Cambridge, taking his Arts degree in 1597 and departing the following year, aged nineteen, for Padua, to receive his medical education from the best medical school in Europe. Here he learnt anatomy from Fabricius ab Aquapendente for whom only four years before a new anatomical theatre had been built, in the form of six narrow concentric galleries below which was placed a table for the body. The whole theatre was windowless, and lighting was from two candelabra of three candles each, and eight lamps held by students. During the five years Harvey spent in Padua Fabricius ab Aqua- pendente was producing for publication his work, De Venarum Osteolis, on the valves in the veins, which was published in I603. One may be quite sure, under these circumstances, that these valves were thoroughly demonstrated and discussed in the presence of the student Harvey, and that in conditions of darkness which he found particularly favourable for contemplation of their significance. -

THE AMERICAN P Founded in 1887 for the Purpose of Promo Ting the in Crease of Physiologica I Knowledge and Its U Tilization
THE AMERICAN P Founded in 1887 for the purpose of promo ting the in crease of physiologica I knowledge and its u tilization. President Earl H. Wood, Mayo Med. Sch., Rochester, MN President- Elect Francis J. Haddy, Uniformed Services Univ. of Hlth. Sci., Bethesda, MD Volume 24, No. 1, February 1981 Past President TA BNTENT Ernst Knobil, Univ. of Pittsburgh Council BCIETY AFFAIRS Earl H. Wood, Francis J. Haddy, Ernst Knobil, Jack L. Kostyo, Eugene Markley Landis ............................... 1 S. McD. McCann, Paul C. Johnson, Leon Farhi Past President’s Address ... Ernst Knobil ................ 3 Pulmonary Physiology and Function Testing in Small Executive Secretary-Treasurer Laboratory Animals ................................ 8 Orr E. Reynolds, 9650 Rockville Pike, Bethesda, Maryland Physiology Career Opportunities Symposium ............ 8 20014 Notes from Capitol Hill. ............................... 8 Meeting of the Section on Cellular and General Physiology . 9 Honors and Awards ................................... 9 Member Contributions. ............................... 10 CIBA Geigy Corp. Application and Instructions. .......................... 15 Grass Instrument Co. A.H. Robins Co., Inc. Hoechst-Roussel Pharmaceu- IST0RICAL ARTICLES Arlie V. Bock - Physiologist . D. B. Dill . 11 ANMQUNCEMENTS ICI Americas Inc. Oxygen Transport to Human Tissues .................... 7 Eli Lilly and Co. NEH 1981 Humanities Seminars. ....................... 9 McNeil Labor Life Sciences Research Office ......................... 10 Merck Sharp Pharmacology -

Slater V. Baker and Stapleton (C.B. 1767): Unpublished Monographs by Robert D. Miller
SLATER V. BAKER AND STAPLETON (C.B. 1767): UNPUBLISHED MONOGRAPHS BY ROBERT D. MILLER ROBERT D. MILLER, J.D., M.S. HYG. HONORARY FELLOW MEDICAL HISTORY AND BIOETHICS DEPARTMENT SCHOOL OF MEDICINE AND PUBLIC HEALTH UNIVERSITY OF WISCONSIN - MADISON PRINTED BY AUTHOR MADISON, WISCONSIN 2019 © ROBERT DESLE MILLER 2019 BOUND BY GRIMM BOOK BINDERY, MONONA, WI AUTHOR’S INTRODUCTION These unpublished monographs are being deposited in several libraries. They have their roots in my experience as a law student. I have been interested in the case of Slater v. Baker and Stapleton since I first learned of it in law school. I was privileged to be a member of the Yale School Class of 1974. I took an elective course with Dr. Jay Katz on the protection of human subjects and then served as a research assistant to Dr. Katz in the summers of 1973 and 1974. Dr. Katz’s course used his new book EXPERIMENTATION WITH HUMAN BEINGS (New York: Russell Sage Foundation 1972). On pages 526-527, there are excerpts from Slater v. Baker. I sought out and read Slater v. Baker. It seemed that there must be an interesting backstory to the case, but it was not accessible at that time. I then practiced health law for nearly forty years, representing hospitals and doctors, and writing six editions of a textbook on hospital law. I applied my interest in experimentation with human beings by serving on various Institutional Review Boards (IRBs) during that period. IRBs are federally required committees that review and approve experiments with humans at hospitals, universities and other institutions. -

The Dissenting Tradition in English Medicine of the Seventeenth and Eighteenth Centuries
Medical History, 1995, 39: 197-218 The Dissenting Tradition in English Medicine of the Seventeenth and Eighteenth Centuries WILLIAM BIRKEN* In England, medicine has always been something of a refuge for individuals whose lives have been dislocated by religious and political strife. This was particularly true in the seventeenth century when changes in Church and State were occurring at a blinding speed. In his book The experience of defeat, Christopher Hill has described the erratic careers of a number of radical clergy and intellectuals who studied and practised medicine in times of dislocation. A list pulled together from Hill's book would include: John Pordage, Samuel Pordage, Henry Stubbe, John Webster, John Rogers, Abiezer Coppe, William Walwyn and Marchamont Nedham.1 Medicine as a practical option for a lost career, or to supplement and subsidize uncertain careers, can also be found among Royalists and Anglicans when their lives were similarly disrupted during the Interregnum. Among these were the brilliant Vaughan twins, Thomas, the Hermetic philosopher, and Henry, the metaphysical poet and clergyman; the poet, Abraham Cowley; and the mercurial Nedham, who was dislocated both as a republican and as a royalist. The Anglicans Ralph Bathurst and Mathew Robinson were forced to abandon temporarily their clerical careers for medicine, only to return to the Church when times were more propitious. In the middle of the eighteenth century the political and religious disabilities of non-juring Anglicanism were still potent enough to impel Sir Richard Jebb to a successful medical career. But by and large the greatest impact on medicine came from the much larger group of the displaced, the English Dissenters, whose combination of religion and medicine were nothing short of remarkable. -

George Abbot 1562-1633 Archbishop of Canterbury
English Book Owners in the Seventeenth Century: A Work in Progress Listing How much do we really know about patterns and impacts of book ownership in Britain in the seventeenth century? How well equipped are we to answer questions such as the following?: • What was a typical private library, in terms of size and content, in the seventeenth century? • How does the answer to that question vary according to occupation, social status, etc? • How does the answer vary over time? – how different are ownership patterns in the middle of the century from those of the beginning, and how different are they again at the end? Having sound answers to these questions will contribute significantly to our understanding of print culture and the history of the book more widely during this period. Our current state of knowledge is both imperfect, and fragmented. There is no directory or comprehensive reference source on seventeenth-century British book owners, although there are numerous studies of individual collectors. There are well-known names who are regularly cited in this context – Cotton, Dering, Pepys – and accepted wisdom as to collections which were particularly interesting or outstanding, but there is much in this area that deserves to be challenged. Private Libraries in Renaissance England and Books in Cambridge Inventories have developed a more comprehensive approach to a particular (academic) kind of owner, but they are largely focused on the sixteenth century. Sears Jayne, Library Catalogues of the English Renaissance, extends coverage to 1640, based on book lists found in a variety of manuscript sources. Evidence of book ownership in this period is manifested in a variety of ways, which need to be brought together if we are to develop that fuller picture. -

Annotated Bibliography of the Works of Walter Charleton1
ANNOTATED BIBLIOGRAPHY OF THE WORKS OF WALTER CHARLETON1 Published works Chorea Gigantum, or, The Most Famous Antiquity of Great-Britan [sic], Vulgarly called Stone-Heng, Standing on Salisbury Plain, Restored to the Danes, London, Printed for Henry Herringman, 1663. The Most Notable Antiquity of Great-Britain, Vulgarly called Stone-Heng, on Salisbury Plain, Restored, by Inigo Jones . to which are added Chorea Gigantum and Mr Webb’s Vindication, London, Printed for D. Browne Junior, and J. Woodman and D. Lyon, 1725. A facsimile edition of the 1725 edition has been produced, introduced by Stuart Piggot, Farnborough, Gregg, 1971. Charleton dedicated Chorea ‘to the King’s Most Excellent Majesty’, and referred to the monarch’s personal interest in the matter. In July 1663, when the physician presented his observations on Stonehenge to the Society, Aubrey was asked to look into the matter.2 He indicated that the King was quite taken with Charleton’s theory about Stonehenge. Charleton and Aubrey attended the King and the Duke and Duchess of York when they visited the area in 1663.3 Chorea contributed to contemporary debate about the origins of the mon- ument. It criticised Inigo Jones’ The Most Notable Antiquity of Great Britain, vulgarly called Stone-heng, restored, which argued for the Roman origin of the stone monuments. Charleton claimed that Stonehenge was in fact the construction of ancient Danes. This initiated considerable contro- versy, and was ill-received in London. Wood claims Charleton’s text was ‘exploded by most persons when t’was published’. Chorea garnered a severe retaliation from Jones’s son-in-law, John Webb.4 1 The works are organised alphabetically, and are designed to provide a quick reference while read- ing the main body of the book. -

Download 1 File
WELLCOME INSTITUTE FOR THE HISTORY OF MEDICINE 183 Euston Road, London NW1 2BP 22501691489 HUGUENOTS IN THE MEDICAL WORLD Digitized by the Internet Archive in 2014 https://archive.org/details/b20456918 WELLCOME INSTITUTE FOR THE HISTORY OF MEDICINE 183 Euston Road, London NW1 HUGUENOTS IN THE MEDICAL WORLD AN EXHIBITION 23 September to 18 December 1985 Monday to Friday 9.45 a.m. to 5.15 p.m. WELLCOME COLLECTION Introduction This exhibition has been arranged at the suggestion of the Huguenot Society of London as part of the Huguenot Heritage celebrations commemorating the contribution of the Huguenot refugees to British life. The year 1985 marks the third centenary of the Revocation of the Edict of Nantes, which by removing the right to freedom of worship stimulated a mass migration of the French Protestant community, and is also the centenary of the foundation of the Huguenot Society of London. The Religious Background The term Huguenot, of doubtful etymology, had become established by the 1560s as a popular name for the French Protestants, or, more accurately, Calvinists. In England, however, it has customarily been used in a wider sense as a generic term to cover all Protestant refugees , including those from the Low Countries; this usage has been followed for the purposes of this exhibition. It has seemed reasonable to include refugees who arrived from the 16th century onwards, preceding the main wave of the late 17th century, and to say something about Protestant medical men who never left France, including some who eventually abjured their faith. Protestant emigration from the Low Countries in the late 16th century was in reaction to persecution by the Spanish rulers of the provinces. -

Smt. B.K. Shah Medical Institute & Research Center Academic Programme Attended (Cme/Conference) : Faculty from : 01/01/2017
SUMANDEEP VIDYAPEETH DECLARED AS AN INSTITUTION DEEMED TO BE UNIVERSITY U/S 3 OF UGC ACT OF 1956 ACCREDITED - NAAC 'A' GRADE SMT. B.K. SHAH MEDICAL INSTITUTE & RESEARCH CENTER ACADEMIC PROGRAMME ATTENDED (CME/CONFERENCE) : FACULTY FROM : 01/01/2017 TO 31/12/2017 Sr. Name of Date of Venue of Level of Designation Department Name of Event Organizing Body No. Faculty Event Event Event Department of Auditorium Psychiatry Mr.K.M Assistant CME on Managing strss- SBKSMIRC 1 Anatomy 1/13/2017 SBKSMIRC State Parmar Professor defeating depression Sumandeep Sumandeep Vidyapeeth Vidyapeeth Department of Auditorium Psychiatry CME on Managing strss- SBKSMIRC 2 Mrs. Priyanka Tutor Anatomy 1/13/2017 SBKSMIRC State defeating depression Sumandeep Sumandeep Vidyapeeth Vidyapeeth Department of Auditorium Psychiatry Dr. J.M. Professor & CME on Managing strss- SBKSMIRC 3 Physiology 13/01/2017 SBKSMIRC State Harsoda Head defeating depression Sumandeep Sumandeep Vidyapeeth Vidyapeeth Department of Auditorium Psychiatry Associate CME on Managing strss- SBKSMIRC 4 Dr. Puja Dullo Physiology 13/01/2017 SBKSMIRC State Professor defeating depression Sumandeep Sumandeep Vidyapeeth Vidyapeeth Sr. Name of Date of Venue of Level of Designation Department Name of Event Organizing Body No. Faculty Event Event Event Department of Auditorium Psychiatry Mrs. G Assistant CME on Managing strss- SBKSMIRC 5 Physiology 13/01/2017 SBKSMIRC State Purohit Professor defeating depression Sumandeep Sumandeep Vidyapeeth Vidyapeeth Department of Auditorium Psychiatry Mrs. Hiral CME on Managing -
MEDICAL DOCTORS International Appeal to Stop 5G on Earth and In
International Appeal to Stop 5G on Earth and in Space MEDICAL DOCTORS ALBANIA Belkez Dedolli Ferri, Medecine, Physician, Prishtina, Kosova Erjet Malaj, Medicine, Tirana ANDORRA Vladimir Laudanovic, MD - Maxillofacial surgeon, Dr, Surgeon, Escaldes ARGENTINA Medardo Ávila-Vazquez, Medico, Salud ambiental, Docente en catedra de clínica Pediátrica, Facultad de ciencias médicas de universidad nacional de Córdoba, Córdoba, cordoba Valentina Battistino, Medica, Doctor, Universidad Nacional de Cordoba, Cordoba, Cordoba Yainol Blanco, Physician, Doctor, Buenos Aires, Buenos Aires Virginia Cambero, Medicina Preventiva, Buenos Aires Nancy Domínguez, Médica, Endomedicina, Teo, Chubut Celia Dorra, University, Family practice, Córdoba, Cordoba Carol Golini, Medica Pediatra, Ciudad Autónoma de Buenos Aires Alfredo Layna, Medico, UBA, Buenos Aires Mariana Mampaey, Doctor, Argentinien, Misiones Beatriz Rauber, Especialista en Medicina Biologica, Medico, Directora internacional de Ozonoterapia de la Academia de Ciencias,Tecnología, Medicina y Terapias Alternativas de México., Cordoba, Cordoba Ester Szlit, Gynecology, University Buenos Aires, Buenos Aires, Buenos Aires ARMENIA Sinerik Ayrapetyan, Neuroscince, Yerevan AUSTRALIA Robert Adler, MBBS RACP, Sydney, NSW Liana Arestia, Korumburra, Victoria Angela Baklis, Melbourne, Victoria David Bird, MBCHB, FRACGP, FACNEM, General Practice, Nutritional and Environmental Medicine, Melbourne, Victoria Hilton Blauensteiner, Brisbane, Queensland Helen Broom, MBBS, Brisbane, QLD Julia Bruce-Thomson, BSc ( Hons) MBChB -
The Harveian Oration I Desire, Sir, to Record My Any Enmity
OCTOBER 21, 1922. exists in support of tho contention, it is impossible to Oration believe tl’at some <.<.Ho of the fierce political and The Harveian religious passions then raging in England was not ON heard within the walls of College. For the (’ollege THE CENTURY contained in it,s body men ready to clie for the king. MEDICINE IN and rnon just as ready to send that king to a shameful BEFORE HARVEY. death ; men to wholll the was an abomina- tion, and men who sighed for the days of universal BY ARNOLD CHAPLIN, M.D.CAMB., orthodoxy, before King llenry VIII. had raised his F.R.C.P. LOND., destroying hand. All honour, then, to this College for the restraint it was able to exercise, so that, while LIBRARIAN OF THE ROYAL COLLEGE OF PHYSICIANS HARVEIAN were a OF LONDON. Puritan and Iloyalist engaged in deadly struggle, the Fellows, holding the same divergent opinions, were able to meet and conduct their business with FELLOws, LADIES, AND CJENTLEMEN. MR. PBESJDENT, such that has been unable to record -In the command of to decorum history obeying your predecessor overt act of The amount of control deliver the Harveian Oration I desire, Sir, to record my any enmity. needed be when men like John Bathurst sense of the honour bestowed upon me, and may imagined deep great and Laurence both in Cromwell’s service and of the diffidence I in approaching a task Wright, experience in his took their seats at the Comitia that has the abilities of so many distinguished high favour, occupied side side with and Sir Charles men in the past. -

Dr. John King (1614-1681) and Dr. Assuerus Regemorter
DR. JOHN KING (1614-1681) AND DR. ASSUERUS REGEMORTER (1615-1650) BRETHREN IN THE DUTCH CHURCH AND IN THE ROYAL COLLEGE OF PHYSICIANS OF LONDON, WITH ADDED REFERENCES TO OTHER "DUTCH" CONGREGANTS IN THE ROYAL COLLEGE, DR. BALDWIN HAMEY AND DR. GEORGE ENT by WILLIAM BIRKEN* This paper is principally concerned with the life and background of the hitherto obscure Dr. John King. However, in telling his story aspects of Dr. Assuerus Regemorter and, to a lesser extent, Dr. Baldwin Hamey and Dr. George Ent, inevitably appear. Between 1634 and 1648, all these men were admitted as Fellows to the Royal College ofPhysicians ofLondon. During the same period as well, their names appeared on the membership lists of the Dutch Church in London, at Austin Friars. In the cases of both Dr. King and Dr. Regemorter this relationship to the Dutch Church and its community was both intimate and lifelong. Coincidentally, it was also during a similar period, 1634 to 1643, that the Dutch Church faced the greatest threat to its existence in all its 425-year history in England. As Dr. Johannes Lindeboom has written in his history ofAustin Friars: Never has the relationship of the foreigners to the State Church been more difficult and more in the nature of a rope that hurts through being drawn too tightly, than in the days of Archbishop Laud, during the reign ofCharles I. The image ofthe too tightly drawn rope is actually too mild. The attitude of the State Church developed into an effort to strangle the life of the Community entirely, and thus to cause its eventual extinction." The details of this struggle can be found in a number of sources.2 Its real significance was in firmly joining the interests of the Dutch Church with the Parliamentary opposi- tion to the Laudian-Caroline State. -

The Aquinas Review, Vol. HI, No. T, 1996
The Aquinas Review, VoL. HI, No. t, 1996 WILUAM HARVEY, M.D.: MoDERN oR ANciENT SciENTisT? Herbert Albert Ratner, M.D. William Harvey was born in Englaud in 1578 and died in r657. He received his grammar school education at the fa mous King's School in Canterbury. In 1593 he entered Caius College, Cambridge, and received hisB.A. degree in 1597. In this period, it was not unusual for English Protestants in terested in a scientific education to seek it in a continental Catholic university. Harvey chose the Universitas ]uristarum, the more influential of the two universities which constituted the University of Padua in Italy and which had been attended by Thomas Linacre and John Caius, and where, incidentally, the Dominican priests were associated with University func tions. Competency in the traditional studies of the day was char acteristic of William Harvey's intellectual development. The degree of Doctor of Physic was awarded to Harvey in r6o2 with the unusual testimonial that "he had conducted himself so wonderfully well in the examination, and had shown such skill, memory, and learning that he had far surpassed even the great hopes which his examiners had formed of him. They decided therefore that he was skilled, expert, and most effi ciently qualified both in arts aud medicine, and to this they Dr. Ratner, a philosopher ofmedicine, is Visiting Professor of Com munity and Preventive Medicine, New York Medical College, and ed itor of Child and Family. This article was originally published as one of a series in a special issue of The Thomist, Volume XXIV, Nos.