Research: Hurricane Katrina Deaths, Louisiana, 2005
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Texas Hurricane History
Texas Hurricane History David Roth National Weather Service Camp Springs, MD Table of Contents Preface 3 Climatology of Texas Tropical Cyclones 4 List of Texas Hurricanes 8 Tropical Cyclone Records in Texas 11 Hurricanes of the Sixteenth and Seventeenth Centuries 12 Hurricanes of the Eighteenth and Early Nineteenth Centuries 13 Hurricanes of the Late Nineteenth Century 16 The First Indianola Hurricane - 1875 21 Last Indianola Hurricane (1886)- The Storm That Doomed Texas’ Major Port 24 The Great Galveston Hurricane (1900) 29 Hurricanes of the Early Twentieth Century 31 Corpus Christi’s Devastating Hurricane (1919) 38 San Antonio’s Great Flood – 1921 39 Hurricanes of the Late Twentieth Century 48 Hurricanes of the Early Twenty-First Century 68 Acknowledgments 74 Bibliography 75 Preface Every year, about one hundred tropical disturbances roam the open Atlantic Ocean, Caribbean Sea, and Gulf of Mexico. About fifteen of these become tropical depressions, areas of low pressure with closed wind patterns. Of the fifteen, ten become tropical storms, and six become hurricanes. Every five years, one of the hurricanes will become reach category five status, normally in the western Atlantic or western Caribbean. About every fifty years, one of these extremely intense hurricanes will strike the United States, with disastrous consequences. Texas has seen its share of hurricane activity over the many years it has been inhabited. Nearly five hundred years ago, unlucky Spanish explorers learned firsthand what storms along the coast of the Lone Star State were capable of. Despite these setbacks, Spaniards set down roots across Mexico and Texas and started colonies. Galleons filled with gold and other treasures sank to the bottom of the Gulf, off such locations as Padre and Galveston Islands. -

Pilotthe Cameron Parish 35¢ June 21, 2007 Vol
PilotThe Cameron Parish 35¢ June 21, 2007 Vol. 50--No. 37 Cameron, La. 70631 THIS HISTORIC photo was taken from the second or third floor of the Cameron Courthouse on June 27, 1957, the day that Hurricane Audrey devastated Cameron Parish. Several hundred persons in the courthouse survived but about 500 others else- where in the parish perished. This photo was taken by the late Hadley Fontenot, who was Cameron’s county agent at the time. Audrey’s 50th anniversary will be observed Wednesday, June 27 in ceremonies at the courthouse. Audrey’s 50th anniversary to be observed here June 27th By CYNDI SELLERS Hurricane Audrey book; Cameron Parish Library - his- Even as Cameron Parish torical photos; Cameron Pilot struggles to recover from the - archival materials including effects of Hurricane Rita, the the first issue after the storm; tragic and devastating impact KPLC-TV - documentaries of Hurricane Audrey in 1957 and film clips; and the has not been forgotten. On National Hurricane Museum Wednesday, June 27, the and Science Center. parish will commemorate the Corporate sponsors of the 50th anniversary of the dead- commemoration are Cheniere ly storm, which claimed over LNG, Sempra Energy, and 400 lives. Cameron Communications. The ceremony will take place at 10 a.m. on the steps of the Cameron Court House, Oak Grove which sheltered hundreds from the fury of the storm. A speaker told light lunch will be served Brigadier General after the program, and dis- plays of hurricane informa- Robert J. LeBlanc Rev. John Reynolds will be tion, books, and memorabilia guest speaker at Oak Grove will be available for viewing. -

Hurricane Audrey Storm Tide
QC9¥f 0 7^-2 3 39 NAL HURRICANE RESEARCH PROJECT ATSL REPORT NO. 23 Hurricane Audrey Storm Tide *•*'• U. S. DEPARTMENT OF COMMERCE Sinclair Weeks, Secretary WEATHER BUREAU F. W. Reichelderfer, Chief NATIONAL HURRICANE RESEARCH PROJECT REPORT NO. 23 Hurricane Audrey Storm Tide by D. Lee Harris U. S. Weather Bureau, Washington, D. C. Washington, D. C. October 1958 UlfiMOl 0b0b32^ NATIONAL HURRICANE RESEARCH PROJECT REPORTS Reports by Weather Bureau units, contractors, and coopera- tors working on the hurricane problem are pre-printed in this series to facilitate immediate distribution of the information among the workers and other interested units. As this limited < reproduction and distribution in this form do not constitute formal scientific publication, reference to a paper in the . series should identify it as a pre-printed report. 1. Objectives and basic desigu of the National Hurricane Research Pro- ? No. ject. March 1956. ^ T , inR^ I P Numerical weather prediction of hurricane motion. July 195©. No. SementTError analysis of prognostic 500-mb. maps made for numer ical weather prediction of hurricane motion. March 195 (> 3. Rainfall associated with hurricanes. July 195&. i] No. I. %m problems involved in the study of storm surges. December 1956. is No. 5. Survey of meteorological factors pertinent to reduction of loss of life and property in hurricane situations. March 1957. ; No 6. A mean atmosphere for the West Indies area. May 1957. j No. 7. An index of tide gages and tide gage records for the Atlantic and Gulf coasts of the United States. May 1957- \ Nmo ft PartE£ Ili. ^exchangeHurricanes andoftheenergysea betweensurface temperaturethe sea and thefield.atmosphere ?j in relation to hurricane behavior. -
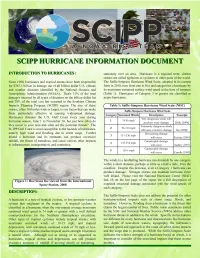
Hurricanes Are a Regular Threat to the SCIPP Gulf Coast and Average Amount of Time That Passes Between Hurricane Events at Should Be Planned for Each Season
SCIPP HURRICANE CLIMATOLOGY: The NHC defines the Atlantic hurricane season as the period from part of the hurricane season, landfall occurrences shift from the June 1 to November 30. Tropical cyclones occur with greatest Gulf Coast to the U.S. east coast. frequency during that time period, which is when the sea surface temperatures are warmest, but can still occur outside of the The relative return frequency of hurricane landfalls can give us a official season. statistical idea of just how often we can expect a hurricane at a specific spot along the Gulf Coast. A return period represents the Hurricanes are a regular threat to the SCIPP Gulf Coast and average amount of time that passes between hurricane events at should be planned for each season. Of the top 10 deadliest and any one location based on the historical record. Figure 3 depicts top 10 costliest (adjusted for inflation, 2006) tropical cyclones to the return frequency for some notable beaches in the SCIPP make U.S. landfall, five in each list have occurred along the domain, from 1900-2005 records. For all of the beaches analyzed SCIPP coast. From 1851-2006 128 hurricanes have affected the in the study, a tropical cyclone can by expected every 3-5 years Texas, Louisiana, or Mississippi coastline, 58 of them have been and a hurricane every 7-15 years. Major hurricanes are much major hurricanes of Category 3 or greater. more rare and, based on past storm events, have a return period of 26 or 52 years for most of the beaches. -

Houston Resiliency
*¤ ű lţţţ Fd9 * Bl&l* *|l& G *C*:&*ũ Celebrating 75 Years of Excellence IN 2017, THE AMERICAN SOCIETY OF CIVIL ENGINEERS TEXAS SECTION GRADED SEVEN CATEGORIES IN ITS G.P.A. REPORT CARD FOR TEXAS INFRASTRUCTURE: AVIATION, BRIDGES, DAMS, DRINKING WATER, FLOOD CONTROL, HIGHWAYS/ROADS AND WASTEWATER. THESE GRADES 76% OF TEXAS INFRASTRUCTURE IGH WERE DEVISED FROM KEY FACTS AND DATA POINTS 1,212 H EDERAL PPROACHING THE ABOUT EACH AREA OF INFRASTRUCTURE. FLOOD F A CONTROL AND DAMS, TWO CATEGORIES OF RISK DAMS DISTASERS ARE END OF ITS SERVICE INFRASTRUCTURE CRITICAL TO RESILIENCY AND STORM C- MANAGEMENT, RECEIVED GRADES OF D, MEANING THE FLOOD RELATED LIFE INFRASTRUCTURE IS POOR AND AT RISK. W HY LEADERSHIP & PLANNING PREPARING FOR THE FUTURE FLOOD CONTROL DAMS INVESTMENT SMART INVESTMENT WILL ONLY BE WE HAVE TO UTILIZE NEW WE CAN NO LONGER AFFORD TO POSSIBLE WITH LEADERSHIP, APPROACHES, MATERIALS, AND DEFER INVESTMENT IN OUR NATION’S PLANNING, AND A CLEAR VISION FOR TECHNOLOGIES TO ENSURE OUR CRITICAL INFRASTRUCTURE SYSTEMS. OUR NATION’S INFRASTRUCTURE. INFRASTRUCTURE IS MORE RESILIENT. W H A T D D FOR MORE INFORMATION ABOUT THE TEXAS REPORT CARD, PLEASE VISIT infrastructurereportcard.org/Texas TELL CONGRESS TALK ABOUT THE ASK FOR FUNDING TELL CONGRESS TO MAKE LARGE-SCALE REPORT CARD GRADE WRITE YOUR MEMBERS OF CONGRESS FEDERAL INVESTMENTS IN WHILE WE HAVE MADE SOME PROGRESS, AND ASK THEM TO FUND THE NATIONAL INFRASTRUCTURE. THIS WILL ALLOW REVERSING THE TRAJECTORY AFTER DAM REHABILITATION PROGRAM SO STATES TO LEVERAGE LOCAL AND PRIVATE DECADES OF UNDERINVESTMENT IN OUR THAT OUR STATE’S “D” DAMS CAN FUNDING AND RAISE THE CURRENT INFRASTRUCTURE REQUIRES RECEIVE THE INVESTMENT THEY NEED. -

Geology and Hurricane- Protection Strategies in the Greater New Orleans Area
Geology and Hurricane- Protection Strategies in the Greater New Orleans Area PUBLIC INFORMATION SERIES NO. 11 SUMMER 2006 Louisiana Geological Survey 3079 Energy, Coast & Environment Building Baton Rouge, Louisiana 70803 Tel: 225 578 5320 Fax: 225 578 3662 Richard P. McCulloh, Paul V. Heinrich, and Bill Good www.lgs.lsu.edu Geology and Hurricane-Protection Strategies in the Greater New Orleans Area State of Louisiana Kathleen B. Blanco, Governor Louisiana State University, Baton Rouge Sean O’Keefe, Chancellor Louisiana Geological Survey Chacko J. John, Director and State Geologist Front cover: Canal Street, New Orleans, Louisiana, September 005 by Rocky Beach. This public information document is part of a series published periodically by the Louisiana Geological Survey, whose offices are located at Louisiana State University, Room 3079 Energy, Coast & Environment Building, Baton Rouge, LA 70803-40. This information is distrib- uted free of charge. The publisher does not guarantee the accuracy or correctness of any information. Contact the LGS business office at (5) 578-530 for extra copies or for more information, or visit the web site at http://www.lgs.lsu.edu. This public document was published at a total cost of $3589.6. One thousand copies of this document were published in this printing at a cost of $493.00. This document was published by the Louisiana Geological Survey, 3079 Energy, Coast and Environment, Louisiana State University, Baton Rouge, Louisiana, 70803, to aid in public understanding of the geology of Louisiana under the authority of R.S. 30:06. This material was printed in accordance with standards for printing by state agencies established pursuant to R.S. -

Storm Flooding Sensitivity to Sea Level Rise for Galveston Bay, Texas
Ocean Engineering 44 (2012) 23–32 Contents lists available at SciVerse ScienceDirect Ocean Engineering journal homepage: www.elsevier.com/locate/oceaneng Storm flooding sensitivity to sea level rise for Galveston Bay, Texas Natalya N. Warner a,n, Philippe E. Tissot b a Department of Mathematics and Statistics, Texas A&M University–Corpus Christi, Corpus Christi, TX 78412, USA b Conrad Blucher Institute, Texas A&M University–Corpus Christi, Corpus Christi, TX 78412, USA article info abstract Article history: The combination of sea level rise and population growth in coastal regions makes it essential to Received 24 June 2010 continue improving flood management strategies. Flooding estimates must take into account both local Accepted 2 January 2012 vertical land motion and estimated rates of sea level rise linked to global climate change. Several Editor-in-Chief: A.I. Incecik extreme value distributions are compared using multiple statistical measures for the modeling of Available online 14 February 2012 maximum annual storm surges based on the 105-year record of Galveston Pier 21, Texas. Increases in Keywords: inundation frequencies are computed based on two possible sea level rise scenarios, a conservative Coastal flooding linear continuation of the past century trend, and a scenario based on the upper limit of the sea level Exceedance probability of flooding range in the IPCC AR4 report, i.e. the A1FI scenario. The research shows that by the year 2100 Galveston Bay exceedance probabilities may double for the impact of the largest storms such as Hurricane Ike, but GEV probability distribution may increase by 6–7 times for the smaller surges associated locally with the impact of storms such as Gulf of Mexico Hurricane Hurricanes Cindy, Alicia, and Rita. -

REPORT on HURRICANE BETSY 8-11 SEPTEMBER 1965 in the U
------_k_ '" , ......... - ," -' .S.ARMY ~NGINEER DISTRICT, NEW 0 ~ ~ORPS OF ,ENGINEERS NEW ORLEANS, 'lA . .'. " ," ~th~ ~~ \\SRf.,RY • aMY fNGINEER '#l\r-~' :(~ EXPERIMEHTSTATlQJl SERIAL NO. "'\:! 'tHlK!1BHf'u, MISSISSH>P1 .~. REPORT ON HURRICANE BETSY 8-11 SEPTEMBER 1965 IN THE u. S. ARMY ENGINEER DISTRICT, NEW ORLEANS u. S. ARMY ENGINEER DISTRICT, NEW ORLEANS CORPS OF ENGINEERS NEW ORLEANS, LOUISIANA NOVEMBER 1965 • REPORT 7:>f' p, ON HURRICANE BETSY 8-11 SEPTEMBER 1965 IN THE U. S. ARMY ENGINEER DISTRICT, NEW ORLEANS TABLE OF CONTENTS Paragraph Description FOREWORD I - AUTHORITY 1-01 Authority 1 1-02 Scope 1 II - HISTORY OF HURRICANE 3 III - EMERGENCY OPERATIONS 3-01 New Orleans District 7 3-14 Activity of other agencies 11 3-26 Evacuation 13 IV - POST STORM COLLECTION OF DATA 4-01 General 15 4-03 Collection of hydrologic data 15 4-05 Accuracy of the hydrology survey 15 4-07 Collection of storm damage data 16 4-09 Accuracy of damage survey 16 4-10 Collection of engineering data 17 V - SUMMARY OF DATA 5-01 General 19 5-02 Hydrologic and meteorologic data 19 5-03 Barometric pressures 19 5-04 Winds 19 5-05 Rainfall 19 5-06 Storm tide heights 20 5-12 Hurricane surge overflow 21 5-14 Salt water intrusion 22 5-11 Economic data 23 TABLE OF CONTENTS (Cont'd) Paragraph Description v - SUMMARY OF DATA (Cont'd) 5-19 General storm data (by parish) 23 Orleans Parish 24 Plaquemines Parish 31 St. Bernard Parish 32 Jefferson Parish 35 St. Tammany Parish 37 Lafourche Parish 37 Terrebonne Parish 38 Livingston, St. -

Characteristics of Tornadoes Associated with Land-Falling Gulf
CHARACTERISTICS OF TORNADOES ASSOCIATED WITH LAND-FALLING GULF COAST TROPICAL CYCLONES by CORY L. RHODES DR. JASON SENKBEIL, COMMITTEE CHAIR DR. DAVID BROMMER DR. P. GRADY DIXON A THESIS Submitted in partial fulfillment of the requirements for the degree of Master of Science in the Department of Geography in the Graduate School of The University of Alabama TUSCALOOSA, ALABAMA 2012 Copyright Cory L. Rhodes 2012 ALL RIGHTS RESERVED ABSTRACT Tropical cyclone tornadoes are brief and often unpredictable events that can produce fatalities and create considerable economic loss. Given these uncertainties, it is important to understand the characteristics and factors that contribute to tornado formation within tropical cyclones. This thesis analyzes this hazardous phenomenon, examining the relationships among tropical cyclone intensity, size, and tornado output. Furthermore, the influences of synoptic and dynamic parameters on tornado output near the time of tornado formation were assessed among two phases of a tropical cyclone’s life cycle; those among hurricanes and tropical storms, termed tropical cyclone tornadoes (TCT), and those among tropical depressions and remnant lows, termed tropical low tornadoes (TLT). Results show that tornado output is affected by tropical cyclone intensity, and to a lesser extent size, with those classified as large in size and ‘major’ in intensity producing a greater amount of tornadoes. Increased values of storm relative helicity are dominant for the TCT environment while CAPE remains the driving force for TLT storms. ii ACKNOWLEDGMENTS I would like to thank my advisor and committee chair, Dr. Jason Senkbeil, and fellow committee members Dr. David Brommer and Dr. P. Grady Dixon for their encouragement, guidance and tremendous support throughout the entire thesis process. -

Some Effects of Hurricanes on the Terrestrial Biota, with Special Reference to Camille
Gulf and Caribbean Research Volume 3 Issue 2 January 1971 Some Effects of Hurricanes on the Terrestrial Biota, With Special Reference to Camille Gordon Gunter Gulf Coast Research Laboratory Lionel N. Eleuterius Gulf Coast Research Laboratory Follow this and additional works at: https://aquila.usm.edu/gcr Part of the Marine Biology Commons Recommended Citation Gunter, G. and L. N. Eleuterius. 1971. Some Effects of Hurricanes on the Terrestrial Biota, With Special Reference to Camille. Gulf Research Reports 3 (2): 283-289. Retrieved from https://aquila.usm.edu/gcr/vol3/iss2/9 DOI: https://doi.org/10.18785/grr.0302.09 This Article is brought to you for free and open access by The Aquila Digital Community. It has been accepted for inclusion in Gulf and Caribbean Research by an authorized editor of The Aquila Digital Community. For more information, please contact [email protected]. SOME EFFECTS OF HURRICANES ON THE TERRESTRIAL BIOTA, WITH SPECIAL REFERENCE TO CAMILLE by Gordon Gunter and Lionel N. Eleuterius Gulf Coast Research Laboratory Ocean Springs, Mississippi INTRODUCTION There have been very few articles concerning the effects of hurricanes upon marine and shore organisms. Some effects on fishes have been described by Hubbs (1962) and in that paper he reviewed some of the previous references. Information on animals killed or injured by hurricanes is scarce because potential observers in areas where they strike are generally more concerned with practical personal matters than biological studies right after a bad storm. The senior author has been in or very close to seven West India hurricanes as they came ashore. -

Hurricane Ike Damage Assessment
HARRIS COUNTY DAMAGE ASSESSMENT Helping Harris County Communities Recover from Hurricane Ike February 2009 Table of Contents Executive Summary Acknowledgements Section 1 Introduction 1.1 Hurricane Ike's Toll on Harris County .................................................................... 1-1 1.2 Scope and Purpose ............................................................................................... 1-2 1.3 Data Collection ...................................................................................................... 1-2 1.3.1 Housing ................................................................................................. 1-2 1.3.1.1 Planning and Initiating Housing Inspections ........................... 1-2 1.3.1.2 Selecting and Refining the Sample Size ................................. 1-3 1.3.1.3 Conducting Damage Assessment Inspections ....................... 1-4 1.3.1.4 Developing Extrapolation Model to Estimate Residential Damage ............................................................... 1-4 1.3.1.5 Calculating Damage Percentage and Estimating Damage Cost ........................................................................................ 1-5 1.3.1.6 Identifying Displaced Households ........................................... 1-6 1.3.1.7 Reporting ................................................................................ 1-6 1.3.2 Non-Housing ......................................................................................... 1-6 1.3.2.1 Infrastructure ......................................................................... -

1956 Atlantic Hurricane Database Reanalysis – Sandy Delgado and Chris Landsea
1956 Atlantic Hurricane Database Reanalysis – Sandy Delgado and Chris Landsea Red indicates wind changes of 15 kt or greater Yellow indicates a deletion Green indicates a new entry Blue indicates lat/lon changes greater than 1º “Minor” intensity changes are less than 20 kt “Minor” position changes are less than 2 degrees Unnamed Tropical Storm 1 [June 12-15, 1956] – AL011956 39285 06/12/1956 M= 4 1 SNBR= 858 NOT NAMED XING=1 SSS=0 39290 06/12*220 915 25 0*225 913 30 0*231 912 30 1009*240 910 35 0* 39290 06/12*200 915 25 0*203 915 25 0*208 915 30 0*216 915 35 0* *** *** *** ** *** *** **** *** *** 39295 06/13*253 907 40 0*264 907 50 0*275 909 50 1004*290 908 45 0* 39295 06/13*230 915 40 0*251 913 45 0*275 909 50 1004*294 906 50 0* *** *** *** *** ** *** *** ** 39300 06/14*306 905 40 0*322 910 35 0*338 917 25 1006*347 928 25 0* 39300 06/14*310 906 35 1001*324 910 30 0*338 917 25 1006*345 928 25 0* *** *** ** **** *** ** *** 39305 06/15*349 933 25 0*352 938 20 0* 0 0 0 0* 0 0 0 0* 39310 TS U.S. Tropical Storm Landfall ------------------------------------- 06/13 17Z 29.1N 90.7W 50 kt LA Major changes to the track and minor changes to the intensity shown in McAdie et al. (2009). Evidence for these alterations comes from the NHC microfilm maps, the Historical Weather Maps series, the COADS ship database, Monthly Weather Review, the Local Climatological Data, Surface Weather Observations, Connor (1956), Navy reconnaissance book (ATSR), and Mexican synoptic maps.