Sources of Bias in Systematic Reviews with Or Without Meta-Analysis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pat Croskerry MD Phd
Thinking (and the factors that influence it) Pat Croskerry MD PhD Scottish Intensive Care Society St Andrews, January 2011 RECOGNIZED Intuition Pattern Pattern Initial Recognition Executive Dysrationalia Calibration Output information Processor override T override Repetition NOT Analytical RECOGNIZED reasoning Dual Process Model Medical Decision Making Intuitive Analytical Orthodox Medical Decision Making (Analytical) Rational Medical Decision-Making • Knowledge base • Differential diagnosis • Best evidence • Reviews, meta-analysis • Biostatistics • Publication bias, citation bias • Test selection and interpretation • Bayesian reasoning • Hypothetico-deductive reasoning .„Cognitive thought is the tip of an enormous iceberg. It is the rule of thumb among cognitive scientists that unconscious thought is 95% of all thought – .this 95% below the surface of conscious awareness shapes and structures all conscious thought‟ Lakoff and Johnson, 1999 Rational blind-spots • Framing • Context • Ambient conditions • Individual factors Individual Factors • Knowledge • Intellect • Personality • Critical thinking ability • Decision making style • Gender • Ageing • Circadian type • Affective state • Fatigue, sleep deprivation, sleep debt • Cognitive load tolerance • Susceptibility to group pressures • Deference to authority Intelligence • Measurement of intelligence? • IQ most widely used barometer of intellect and cognitive functioning • IQ is strongest single predictor of job performance and success • IQ tests highly correlated with each other • Population -

A Task-Based Taxonomy of Cognitive Biases for Information Visualization
A Task-based Taxonomy of Cognitive Biases for Information Visualization Evanthia Dimara, Steven Franconeri, Catherine Plaisant, Anastasia Bezerianos, and Pierre Dragicevic Three kinds of limitations The Computer The Display 2 Three kinds of limitations The Computer The Display The Human 3 Three kinds of limitations: humans • Human vision ️ has limitations • Human reasoning 易 has limitations The Human 4 ️Perceptual bias Magnitude estimation 5 ️Perceptual bias Magnitude estimation Color perception 6 易 Cognitive bias Behaviors when humans consistently behave irrationally Pohl’s criteria distilled: • Are predictable and consistent • People are unaware they’re doing them • Are not misunderstandings 7 Ambiguity effect, Anchoring or focalism, Anthropocentric thinking, Anthropomorphism or personification, Attentional bias, Attribute substitution, Automation bias, Availability heuristic, Availability cascade, Backfire effect, Bandwagon effect, Base rate fallacy or Base rate neglect, Belief bias, Ben Franklin effect, Berkson's paradox, Bias blind spot, Choice-supportive bias, Clustering illusion, Compassion fade, Confirmation bias, Congruence bias, Conjunction fallacy, Conservatism (belief revision), Continued influence effect, Contrast effect, Courtesy bias, Curse of knowledge, Declinism, Decoy effect, Default effect, Denomination effect, Disposition effect, Distinction bias, Dread aversion, Dunning–Kruger effect, Duration neglect, Empathy gap, End-of-history illusion, Endowment effect, Exaggerated expectation, Experimenter's or expectation bias, -

Adaptive Clinical Trials: an Introduction
Adaptive clinical trials: an introduction What are the advantages and disadvantages of adaptive clinical trial designs? How and why were Introduction adaptive clinical Adaptive clinical trial design is trials developed? becoming a hot topic in healthcare research, with some researchers In 2004, the FDA published a report arguing that adaptive trials have the on the problems faced by the potential to get new drugs to market scientific community in developing quicker. In this article, we explain new medical treatments.2 The what adaptive trials are and why they report highlighted that the pace of were developed, and we explore both innovation in biomedical science is the advantages of adaptive designs outstripping the rate of advances and the concerns being raised by in the available technologies and some in the healthcare community. tools for evaluating new treatments. Outdated tools are being used to assess new treatments and there What are adaptive is a critical need to improve the effectiveness and efficiency of clinical trials? clinical trials.2 The current process for developing Adaptive clinical trials enable new treatments is expensive, takes researchers to change an aspect a long time and in some cases, the of a trial design at an interim development process has to be assessment, while controlling stopped after significant amounts the rate of type 1 errors.1 Interim of time and resources have been assessments can help to determine invested.2 In 2006, the FDA published whether a trial design is the most a “Critical Path Opportunities -

Cognitive Bias Mitigation: How to Make Decision-Making More Rational?
Cognitive Bias Mitigation: How to make decision-making more rational? Abstract Cognitive biases distort judgement and adversely impact decision-making, which results in economic inefficiencies. Initial attempts to mitigate these biases met with little success. However, recent studies which used computer games and educational videos to train people to avoid biases (Clegg et al., 2014; Morewedge et al., 2015) showed that this form of training reduced selected cognitive biases by 30 %. In this work I report results of an experiment which investigated the debiasing effects of training on confirmation bias. The debiasing training took the form of a short video which contained information about confirmation bias, its impact on judgement, and mitigation strategies. The results show that participants exhibited confirmation bias both in the selection and processing of information, and that debiasing training effectively decreased the level of confirmation bias by 33 % at the 5% significance level. Key words: Behavioural economics, cognitive bias, confirmation bias, cognitive bias mitigation, confirmation bias mitigation, debiasing JEL classification: D03, D81, Y80 1 Introduction Empirical research has documented a panoply of cognitive biases which impair human judgement and make people depart systematically from models of rational behaviour (Gilovich et al., 2002; Kahneman, 2011; Kahneman & Tversky, 1979; Pohl, 2004). Besides distorted decision-making and judgement in the areas of medicine, law, and military (Nickerson, 1998), cognitive biases can also lead to economic inefficiencies. Slovic et al. (1977) point out how they distort insurance purchases, Hyman Minsky (1982) partly blames psychological factors for economic cycles. Shefrin (2010) argues that confirmation bias and some other cognitive biases were among the significant factors leading to the global financial crisis which broke out in 2008. -

THE ROLE of PUBLICATION SELECTION BIAS in ESTIMATES of the VALUE of a STATISTICAL LIFE W
THE ROLE OF PUBLICATION SELECTION BIAS IN ESTIMATES OF THE VALUE OF A STATISTICAL LIFE w. k i p vi s c u s i ABSTRACT Meta-regression estimates of the value of a statistical life (VSL) controlling for publication selection bias often yield bias-corrected estimates of VSL that are substantially below the mean VSL estimates. Labor market studies using the more recent Census of Fatal Occu- pational Injuries (CFOI) data are subject to less measurement error and also yield higher bias-corrected estimates than do studies based on earlier fatality rate measures. These re- sultsareborneoutbythefindingsforalargesampleofallVSLestimatesbasedonlabor market studies using CFOI data and for four meta-analysis data sets consisting of the au- thors’ best estimates of VSL. The confidence intervals of the publication bias-corrected estimates of VSL based on the CFOI data include the values that are currently used by government agencies, which are in line with the most precisely estimated values in the literature. KEYWORDS: value of a statistical life, VSL, meta-regression, publication selection bias, Census of Fatal Occupational Injuries, CFOI JEL CLASSIFICATION: I18, K32, J17, J31 1. Introduction The key parameter used in policy contexts to assess the benefits of policies that reduce mortality risks is the value of a statistical life (VSL).1 This measure of the risk-money trade-off for small risks of death serves as the basis for the standard approach used by government agencies to establish monetary benefit values for the predicted reductions in mortality risks from health, safety, and environmental policies. Recent government appli- cations of the VSL have used estimates in the $6 million to $10 million range, where these and all other dollar figures in this article are in 2013 dollars using the Consumer Price In- dex for all Urban Consumers (CPI-U). -

Bias and Fairness in NLP
Bias and Fairness in NLP Margaret Mitchell Kai-Wei Chang Vicente Ordóñez Román Google Brain UCLA University of Virginia Vinodkumar Prabhakaran Google Brain Tutorial Outline ● Part 1: Cognitive Biases / Data Biases / Bias laundering ● Part 2: Bias in NLP and Mitigation Approaches ● Part 3: Building Fair and Robust Representations for Vision and Language ● Part 4: Conclusion and Discussion “Bias Laundering” Cognitive Biases, Data Biases, and ML Vinodkumar Prabhakaran Margaret Mitchell Google Brain Google Brain Andrew Emily Simone Parker Lucy Ben Elena Deb Timnit Gebru Zaldivar Denton Wu Barnes Vasserman Hutchinson Spitzer Raji Adrian Brian Dirk Josh Alex Blake Hee Jung Hartwig Blaise Benton Zhang Hovy Lovejoy Beutel Lemoine Ryu Adam Agüera y Arcas What’s in this tutorial ● Motivation for Fairness research in NLP ● How and why NLP models may be unfair ● Various types of NLP fairness issues and mitigation approaches ● What can/should we do? What’s NOT in this tutorial ● Definitive answers to fairness/ethical questions ● Prescriptive solutions to fix ML/NLP (un)fairness What do you see? What do you see? ● Bananas What do you see? ● Bananas ● Stickers What do you see? ● Bananas ● Stickers ● Dole Bananas What do you see? ● Bananas ● Stickers ● Dole Bananas ● Bananas at a store What do you see? ● Bananas ● Stickers ● Dole Bananas ● Bananas at a store ● Bananas on shelves What do you see? ● Bananas ● Stickers ● Dole Bananas ● Bananas at a store ● Bananas on shelves ● Bunches of bananas What do you see? ● Bananas ● Stickers ● Dole Bananas ● Bananas -

Quasi-Experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: a Systematic Review
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Infect Control Manuscript Author Hosp Epidemiol Manuscript Author . Author manuscript; available in PMC 2019 November 12. Published in final edited form as: Infect Control Hosp Epidemiol. 2018 February ; 39(2): 170–176. doi:10.1017/ice.2017.296. Quasi-experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: A Systematic Review Rotana Alsaggaf, MS, Lyndsay M. O’Hara, PhD, MPH, Kristen A. Stafford, PhD, MPH, Surbhi Leekha, MBBS, MPH, Anthony D. Harris, MD, MPH, CDC Prevention Epicenters Program Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, Maryland. Abstract OBJECTIVE.—A systematic review of quasi-experimental studies in the field of infectious diseases was published in 2005. The aim of this study was to assess improvements in the design and reporting of quasi-experiments 10 years after the initial review. We also aimed to report the statistical methods used to analyze quasi-experimental data. DESIGN.—Systematic review of articles published from January 1, 2013, to December 31, 2014, in 4 major infectious disease journals. METHODS.—Quasi-experimental studies focused on infection control and antibiotic resistance were identified and classified based on 4 criteria: (1) type of quasi-experimental design used, (2) justification of the use of the design, (3) use of correct nomenclature to describe the design, and (4) statistical methods used. RESULTS.—Of 2,600 articles, 173 (7%) featured a quasi-experimental design, compared to 73 of 2,320 articles (3%) in the previous review (P<.01). Moreover, 21 articles (12%) utilized a study design with a control group; 6 (3.5%) justified the use of a quasi-experimental design; and 68 (39%) identified their design using the correct nomenclature. -

A Guide to Systematic Review and Meta-Analysis of Prediction Model Performance
RESEARCH METHODS AND REPORTING A guide to systematic review and meta-analysis of prediction model performance Thomas P A Debray,1,2 Johanna A A G Damen,1,2 Kym I E Snell,3 Joie Ensor,3 Lotty Hooft,1,2 Johannes B Reitsma,1,2 Richard D Riley,3 Karel G M Moons1,2 1Cochrane Netherlands, Validation of prediction models is diagnostic test accuracy studies. Compared to therapeu- University Medical Center tic intervention and diagnostic test accuracy studies, Utrecht, PO Box 85500 Str highly recommended and increasingly there is limited guidance on the conduct of systematic 6.131, 3508 GA Utrecht, Netherlands common in the literature. A systematic reviews and meta-analysis of primary prognosis studies. 2Julius Center for Health review of validation studies is therefore A common aim of primary prognostic studies con- Sciences and Primary Care, cerns the development of so-called prognostic predic- University Medical Center helpful, with meta-analysis needed to tion models or indices. These models estimate the Utrecht, PO Box 85500 Str 6.131, 3508 GA Utrecht, summarise the predictive performance individualised probability or risk that a certain condi- Netherlands of the model being validated across tion will occur in the future by combining information 3Research Institute for Primary from multiple prognostic factors from an individual. Care and Health Sciences, Keele different settings and populations. This Unfortunately, there is often conflicting evidence about University, Staffordshire, UK article provides guidance for the predictive performance of developed prognostic Correspondence to: T P A Debray [email protected] researchers systematically reviewing prediction models. For this reason, there is a growing Additional material is published demand for evidence synthesis of (external validation) online only. -
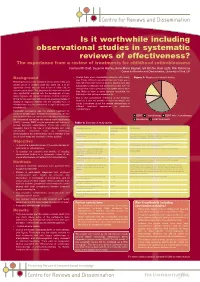
Is It Worthwhile Including Observational Studies in Systematic Reviews of Effectiveness?
CRD_mcdaid05_Poster.qxd 13/6/05 5:12 pm Page 1 Is it worthwhile including observational studies in systematic reviews of effectiveness? The experience from a review of treatments for childhood retinoblastoma Catriona Mc Daid, Suzanne Hartley, Anne-Marie Bagnall, Gill Ritchie, Kate Light, Rob Riemsma Centre for Reviews and Dissemination, University of York, UK Background • Overall there were considerable problems with quality Figure 1: Mapping of included studies (see Table). Without randomised allocation there was a Retinoblastoma is a rare malignant tumour of the retina and high risk of selection bias in all studies. Studies were also usually occurs in children under two years old. It is an susceptible to detection and performance bias, with the aggressive tumour that can lead to loss of vision and, in retrospective studies particularly susceptible as they were extreme cases, death. The prognoses for vision and survival less likely to have a study protocol specifying the have significantly improved with the development of more intervention and outcome assessments. timely diagnosis and improved treatment methods. Important • Due to the considerable limitations of the evidence clinical factors associated with prognosis are age and stage of identified, it was not possible to make meaningful and disease at diagnosis. Patients with the hereditary form of robust conclusions about the relative effectiveness of retinoblastoma may be predisposed to significant long-term different treatment approaches for childhood complications. retinoblastoma. Historically, enucleation was the standard treatment for unilateral retinoblastoma. In bilateral retinoblastoma, the eye ■ ■ ■ with the most advanced tumour was commonly removed and EBRT Chemotherapy EBRT with Chemotherapy the contralateral eye treated with external beam radiotherapy ■ Enucleation ■ Local Treatments (EBRT). -
Why So Confident? the Influence of Outcome Desirability on Selective Exposure and Likelihood Judgment
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by The University of North Carolina at Greensboro Archived version from NCDOCKS Institutional Repository http://libres.uncg.edu/ir/asu/ Why so confident? The influence of outcome desirability on selective exposure and likelihood judgment Authors Paul D. Windschitl , Aaron M. Scherer a, Andrew R. Smith , Jason P. Rose Abstract Previous studies that have directly manipulated outcome desirability have often found little effect on likelihood judgments (i.e., no desirability bias or wishful thinking). The present studies tested whether selections of new information about outcomes would be impacted by outcome desirability, thereby biasing likelihood judgments. In Study 1, participants made predictions about novel outcomes and then selected additional information to read from a buffet. They favored information supporting their prediction, and this fueled an increase in confidence. Studies 2 and 3 directly manipulated outcome desirability through monetary means. If a target outcome (randomly preselected) was made especially desirable, then participants tended to select information that supported the outcome. If made undesirable, less supporting information was selected. Selection bias was again linked to subsequent likelihood judgments. These results constitute novel evidence for the role of selective exposure in cases of overconfidence and desirability bias in likelihood judgments. Paul D. Windschitl , Aaron M. Scherer a, Andrew R. Smith , Jason P. Rose (2013) "Why so confident? The influence of outcome desirability on selective exposure and likelihood judgment" Organizational Behavior and Human Decision Processes 120 (2013) 73–86 (ISSN: 0749-5978) Version of Record available @ DOI: (http://dx.doi.org/10.1016/j.obhdp.2012.10.002) Why so confident? The influence of outcome desirability on selective exposure and likelihood judgment q a,⇑ a c b Paul D. -

How to Get Started with a Systematic Review in Epidemiology: an Introductory Guide for Early Career Researchers
Denison et al. Archives of Public Health 2013, 71:21 http://www.archpublichealth.com/content/71/1/21 ARCHIVES OF PUBLIC HEALTH METHODOLOGY Open Access How to get started with a systematic review in epidemiology: an introductory guide for early career researchers Hayley J Denison1*†, Richard M Dodds1,2†, Georgia Ntani1†, Rachel Cooper3†, Cyrus Cooper1†, Avan Aihie Sayer1,2† and Janis Baird1† Abstract Background: Systematic review is a powerful research tool which aims to identify and synthesize all evidence relevant to a research question. The approach taken is much like that used in a scientific experiment, with high priority given to the transparency and reproducibility of the methods used and to handling all evidence in a consistent manner. Early career researchers may find themselves in a position where they decide to undertake a systematic review, for example it may form part or all of a PhD thesis. Those with no prior experience of systematic review may need considerable support and direction getting started with such a project. Here we set out in simple terms how to get started with a systematic review. Discussion: Advice is given on matters such as developing a review protocol, searching using databases and other methods, data extraction, risk of bias assessment and data synthesis including meta-analysis. Signposts to further information and useful resources are also given. Conclusion: A well-conducted systematic review benefits the scientific field by providing a summary of existing evidence and highlighting unanswered questions. For the individual, undertaking a systematic review is also a great opportunity to improve skills in critical appraisal and in synthesising evidence. -

Guidelines for Reporting Meta-Epidemiological Methodology Research
EBM Primer Evid Based Med: first published as 10.1136/ebmed-2017-110713 on 12 July 2017. Downloaded from Guidelines for reporting meta-epidemiological methodology research Mohammad Hassan Murad, Zhen Wang 10.1136/ebmed-2017-110713 Abstract The goal is generally broad but often focuses on exam- Published research should be reported to evidence users ining the impact of certain characteristics of clinical studies on the observed effect, describing the distribu- Evidence-Based Practice with clarity and transparency that facilitate optimal tion of research evidence in a specific setting, exam- Center, Mayo Clinic, Rochester, appraisal and use of evidence and allow replication Minnesota, USA by other researchers. Guidelines for such reporting ining heterogeneity and exploring its causes, identifying are available for several types of studies but not for and describing plausible biases and providing empirical meta-epidemiological methodology studies. Meta- evidence for hypothesised associations. Unlike classic Correspondence to: epidemiological studies adopt a systematic review epidemiology, the unit of analysis for meta-epidemio- Dr Mohammad Hassan Murad, or meta-analysis approach to examine the impact logical studies is a study, not a patient. The outcomes Evidence-based Practice Center, of certain characteristics of clinical studies on the of meta-epidemiological studies are usually not clinical Mayo Clinic, 200 First Street 6–8 observed effect and provide empirical evidence for outcomes. SW, Rochester, MN 55905, USA; hypothesised associations. The unit of analysis in meta- In this guide, we adapt the items used in the PRISMA murad. mohammad@ mayo. edu 9 epidemiological studies is a study, not a patient. The statement for reporting systematic reviews and outcomes of meta-epidemiological studies are usually meta-analysis to fit the setting of meta- epidemiological not clinical outcomes.