A Systematic Review of COVID-19 Epidemiology Based on Current Evidence
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adaptive Clinical Trials: an Introduction
Adaptive clinical trials: an introduction What are the advantages and disadvantages of adaptive clinical trial designs? How and why were Introduction adaptive clinical Adaptive clinical trial design is trials developed? becoming a hot topic in healthcare research, with some researchers In 2004, the FDA published a report arguing that adaptive trials have the on the problems faced by the potential to get new drugs to market scientific community in developing quicker. In this article, we explain new medical treatments.2 The what adaptive trials are and why they report highlighted that the pace of were developed, and we explore both innovation in biomedical science is the advantages of adaptive designs outstripping the rate of advances and the concerns being raised by in the available technologies and some in the healthcare community. tools for evaluating new treatments. Outdated tools are being used to assess new treatments and there What are adaptive is a critical need to improve the effectiveness and efficiency of clinical trials? clinical trials.2 The current process for developing Adaptive clinical trials enable new treatments is expensive, takes researchers to change an aspect a long time and in some cases, the of a trial design at an interim development process has to be assessment, while controlling stopped after significant amounts the rate of type 1 errors.1 Interim of time and resources have been assessments can help to determine invested.2 In 2006, the FDA published whether a trial design is the most a “Critical Path Opportunities -

STI Screening Timetable
Patient Education Information from University Health Center’s STI Screening Clinic Page 1 of 1 STI Screening Timetable How long until STI (sexually transmitted infection) screening tests turn positive? How long until STI symptoms might show up? The time between infection and a positive test, or between infection and symptoms, is variable and depends on many factors, including the behavior of the infectious agent, how and where the body is infected, and the state of a person’s immune system and personal health. Many STIs don’t have any symptoms. The incubation period times listed in the chart below are averages only. If you have further questions or concerns, you can schedule an appointment with a clinician at 541-346-2770. STI screening test Window period (time from exposure until Incubation period (time between exposure and screening test turns positive) when symptoms appear) Chlamydia (urine specimen or swab of 1 week most of the time Often no symptoms vagina, rectum, throat) 2 weeks catches almost all 1-3 weeks on average Gonorrhea (urine specimen on swab of 1 week most of the time Often no symptoms, especially vaginal vagina, rectum, throat) 2 weeks catches almost all infections usually within 2-8 days but can be up to 2 weeks Syphilis (blood test, RPR) 1 month catches most Often symptoms too mild to notice 3 months catches almost all 10-90 days average 21 days HIV (oral cheek swab) 1 month catches most Sometimes mild body aches and fever within 1-2 3 months catches almost all weeks then can be months to years HIV (blood test, antigen/antibody -

Estimating the Serial Interval of the Novel Coronavirus Disease (COVID
medRxiv preprint doi: https://doi.org/10.1101/2020.02.21.20026559; this version posted February 25, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-NC-ND 4.0 International license . 1 Estimating the serial interval of the novel coronavirus disease 2 (COVID-19): A statistical analysis using the public data in Hong Kong 3 from January 16 to February 15, 2020 4 Shi Zhao1,2,*, Daozhou Gao3, Zian Zhuang4, Marc KC Chong1,2, Yongli Cai5, Jinjun Ran6, Peihua Cao7, Kai 5 Wang8, Yijun Lou4, Weiming Wang5,*, Lin Yang9, Daihai He4,*, and Maggie H Wang1,2 6 7 1 JC School of Public Health and Primary Care, Chinese University of Hong Kong, Hong Kong, China 8 2 Shenzhen Research Institute of Chinese University of Hong Kong, Shenzhen, China 9 3 Department of Mathematics, Shanghai Normal University, Shanghai, China 10 4 Department of Applied Mathematics, Hong Kong Polytechnic University, Hong Kong, China 11 5 School of Mathematics and Statistics, Huaiyin Normal University, Huaian, China 12 6 School of Public Health, Li Ka Shing Faculty of Medicine, University of Hong Kong, Hong Kong, China 13 7 Clinical Research Centre, Zhujiang Hospital, Southern Medical University, Guangzhou, Guangdong, China 14 8 Department of Medical Engineering and Technology, Xinjiang Medical University, Urumqi, 830011, China 15 9 School of Nursing, Hong Kong Polytechnic University, Hong Kong, China 16 * Correspondence -

Incubation Period and Other Epidemiological
Journal of Clinical Medicine Article Incubation Period and Other Epidemiological Characteristics of 2019 Novel Coronavirus Infections with Right Truncation: A Statistical Analysis of Publicly Available Case Data 1, 1, 1 1 Natalie M. Linton y , Tetsuro Kobayashi y, Yichi Yang , Katsuma Hayashi , Andrei R. Akhmetzhanov 1 , Sung-mok Jung 1 , Baoyin Yuan 1, Ryo Kinoshita 1 and Hiroshi Nishiura 1,2,* 1 Graduate School of Medicine, Hokkaido University, Kita 15 Jo Nishi 7 Chome, Kita-ku, Sapporo-shi, Hokkaido 060-8638, Japan; [email protected] (N.M.L.); [email protected] (T.K.); [email protected] (Y.Y.); katsuma5miff[email protected] (K.H.); [email protected] (A.R.A.); [email protected] (S.-m.J.); [email protected] (B.Y.); [email protected] (R.K.) 2 Core Research for Evolutional Science and Technology (CREST), Japan Science and Technology Agency, Honcho 4-1-8, Kawaguchi, Saitama 332-0012, Japan * Correspondence: [email protected]; Tel.: +81-11-706-5066 These authors contributed equally to this work. y Received: 25 January 2020; Accepted: 10 February 2020; Published: 17 February 2020 Abstract: The geographic spread of 2019 novel coronavirus (COVID-19) infections from the epicenter of Wuhan, China, has provided an opportunity to study the natural history of the recently emerged virus. Using publicly available event-date data from the ongoing epidemic, the present study investigated the incubation period and other time intervals that govern the epidemiological dynamics of COVID-19 infections. Our results show that the incubation period falls within the range of 2–14 days with 95% confidence and has a mean of around 5 days when approximated using the best-fit lognormal distribution. -

MMWR Early and Were Reported to Two Respective Local Health Jurisdictions, Release on the MMWR Website (
Morbidity and Mortality Weekly Report High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice — Skagit County, Washington, March 2020 Lea Hamner, MPH1; Polly Dubbel, MPH1; Ian Capron1; Andy Ross, MPH1; Amber Jordan, MPH1; Jaxon Lee, MPH1; Joanne Lynn1; Amelia Ball1; Simranjit Narwal, MSc1; Sam Russell1; Dale Patrick1; Howard Leibrand, MD1 On May 12, 2020, this report was posted as an MMWR Early and were reported to two respective local health jurisdictions, Release on the MMWR website (https://www.cdc.gov/mmwr). without indication of a common source of exposure. On On March 17, 2020, a member of a Skagit County, March 17, the choir director sent a second e-mail stating that Washington, choir informed Skagit County Public Health 24 members reported that they had developed influenza-like (SCPH) that several members of the 122-member choir had symptoms since March 11, and at least one had received test become ill. Three persons, two from Skagit County and one results positive for SARS-CoV-2. The email emphasized the from another area, had test results positive for SARS-CoV-2, importance of social distancing and awareness of symptoms the virus that causes coronavirus disease 2019 (COVID-19). suggestive of COVID-19. These two emails led many members Another 25 persons had compatible symptoms. SCPH to self-isolate or quarantine before a delegated member of the obtained the choir’s member list and began an investigation on choir notified SCPH on March 17. March 18. Among 61 persons who attended a March 10 choir All 122 members were interviewed by telephone either practice at which one person was known to be symptomatic, during initial investigation of the cluster (March 18–20; 53 cases were identified, including 33 confirmed and 20 115 members) or a follow-up interview (April 7–10; 117); most probable cases (secondary attack rates of 53.3% among con- persons participated in both interviews. -

Quasi-Experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: a Systematic Review
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Infect Control Manuscript Author Hosp Epidemiol Manuscript Author . Author manuscript; available in PMC 2019 November 12. Published in final edited form as: Infect Control Hosp Epidemiol. 2018 February ; 39(2): 170–176. doi:10.1017/ice.2017.296. Quasi-experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: A Systematic Review Rotana Alsaggaf, MS, Lyndsay M. O’Hara, PhD, MPH, Kristen A. Stafford, PhD, MPH, Surbhi Leekha, MBBS, MPH, Anthony D. Harris, MD, MPH, CDC Prevention Epicenters Program Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, Maryland. Abstract OBJECTIVE.—A systematic review of quasi-experimental studies in the field of infectious diseases was published in 2005. The aim of this study was to assess improvements in the design and reporting of quasi-experiments 10 years after the initial review. We also aimed to report the statistical methods used to analyze quasi-experimental data. DESIGN.—Systematic review of articles published from January 1, 2013, to December 31, 2014, in 4 major infectious disease journals. METHODS.—Quasi-experimental studies focused on infection control and antibiotic resistance were identified and classified based on 4 criteria: (1) type of quasi-experimental design used, (2) justification of the use of the design, (3) use of correct nomenclature to describe the design, and (4) statistical methods used. RESULTS.—Of 2,600 articles, 173 (7%) featured a quasi-experimental design, compared to 73 of 2,320 articles (3%) in the previous review (P<.01). Moreover, 21 articles (12%) utilized a study design with a control group; 6 (3.5%) justified the use of a quasi-experimental design; and 68 (39%) identified their design using the correct nomenclature. -

A Guide to Systematic Review and Meta-Analysis of Prediction Model Performance
RESEARCH METHODS AND REPORTING A guide to systematic review and meta-analysis of prediction model performance Thomas P A Debray,1,2 Johanna A A G Damen,1,2 Kym I E Snell,3 Joie Ensor,3 Lotty Hooft,1,2 Johannes B Reitsma,1,2 Richard D Riley,3 Karel G M Moons1,2 1Cochrane Netherlands, Validation of prediction models is diagnostic test accuracy studies. Compared to therapeu- University Medical Center tic intervention and diagnostic test accuracy studies, Utrecht, PO Box 85500 Str highly recommended and increasingly there is limited guidance on the conduct of systematic 6.131, 3508 GA Utrecht, Netherlands common in the literature. A systematic reviews and meta-analysis of primary prognosis studies. 2Julius Center for Health review of validation studies is therefore A common aim of primary prognostic studies con- Sciences and Primary Care, cerns the development of so-called prognostic predic- University Medical Center helpful, with meta-analysis needed to tion models or indices. These models estimate the Utrecht, PO Box 85500 Str 6.131, 3508 GA Utrecht, summarise the predictive performance individualised probability or risk that a certain condi- Netherlands of the model being validated across tion will occur in the future by combining information 3Research Institute for Primary from multiple prognostic factors from an individual. Care and Health Sciences, Keele different settings and populations. This Unfortunately, there is often conflicting evidence about University, Staffordshire, UK article provides guidance for the predictive performance of developed prognostic Correspondence to: T P A Debray [email protected] researchers systematically reviewing prediction models. For this reason, there is a growing Additional material is published demand for evidence synthesis of (external validation) online only. -
Is It Worthwhile Including Observational Studies in Systematic Reviews of Effectiveness?
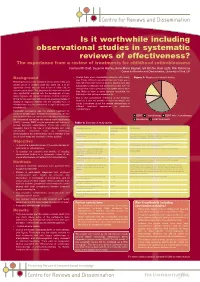
CRD_mcdaid05_Poster.qxd 13/6/05 5:12 pm Page 1 Is it worthwhile including observational studies in systematic reviews of effectiveness? The experience from a review of treatments for childhood retinoblastoma Catriona Mc Daid, Suzanne Hartley, Anne-Marie Bagnall, Gill Ritchie, Kate Light, Rob Riemsma Centre for Reviews and Dissemination, University of York, UK Background • Overall there were considerable problems with quality Figure 1: Mapping of included studies (see Table). Without randomised allocation there was a Retinoblastoma is a rare malignant tumour of the retina and high risk of selection bias in all studies. Studies were also usually occurs in children under two years old. It is an susceptible to detection and performance bias, with the aggressive tumour that can lead to loss of vision and, in retrospective studies particularly susceptible as they were extreme cases, death. The prognoses for vision and survival less likely to have a study protocol specifying the have significantly improved with the development of more intervention and outcome assessments. timely diagnosis and improved treatment methods. Important • Due to the considerable limitations of the evidence clinical factors associated with prognosis are age and stage of identified, it was not possible to make meaningful and disease at diagnosis. Patients with the hereditary form of robust conclusions about the relative effectiveness of retinoblastoma may be predisposed to significant long-term different treatment approaches for childhood complications. retinoblastoma. Historically, enucleation was the standard treatment for unilateral retinoblastoma. In bilateral retinoblastoma, the eye ■ ■ ■ with the most advanced tumour was commonly removed and EBRT Chemotherapy EBRT with Chemotherapy the contralateral eye treated with external beam radiotherapy ■ Enucleation ■ Local Treatments (EBRT). -

The Serial Interval of COVID-19 from Publicly Reported Confirmed Cases
medRxiv preprint doi: https://doi.org/10.1101/2020.02.19.20025452; this version posted March 13, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-NC-ND 4.0 International license . Title: The serial interval of COVID-19 from publicly reported confirmed cases Running Head: The serial interval of COVID-19 1,+ 2+ 3,4+ 5, 6 Authors: Zhanwei Du , Xiaoke Xu , Ye Wu , Lin Wang , Benjamin J. Cowling , and Lauren Ancel Meyers1,7* Affiliations: 1. The University of Texas at Austin, Austin, Texas 78712, The United States of America 2. Dalian Minzu University, Dalian 116600, China 3. Computational Communication Research Center, Beijing Normal University, Zhuhai, 519087, China 4. School of Journalism and Communication, Beijing Normal University, Beijing, 100875, China 5. Institut Pasteur, 28 rue du Dr Roux, Paris 75015, France 6. The University of Hong Kong, Hong Kong SAR, China 7. Santa Fe Institute, Santa Fe, New Mexico, The United States of America Corresponding author: Lauren Ancel Meyers Corresponding author email: [email protected] + These first authors contributed equally to this article Short Abstract (50 words) We estimate the distribution of serial intervals for 468 confirmed cases of COVID-19 reported in 93 Chinese cities by February 8, 2020. The mean and standard deviation are 3.96 NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. -

How to Get Started with a Systematic Review in Epidemiology: an Introductory Guide for Early Career Researchers
Denison et al. Archives of Public Health 2013, 71:21 http://www.archpublichealth.com/content/71/1/21 ARCHIVES OF PUBLIC HEALTH METHODOLOGY Open Access How to get started with a systematic review in epidemiology: an introductory guide for early career researchers Hayley J Denison1*†, Richard M Dodds1,2†, Georgia Ntani1†, Rachel Cooper3†, Cyrus Cooper1†, Avan Aihie Sayer1,2† and Janis Baird1† Abstract Background: Systematic review is a powerful research tool which aims to identify and synthesize all evidence relevant to a research question. The approach taken is much like that used in a scientific experiment, with high priority given to the transparency and reproducibility of the methods used and to handling all evidence in a consistent manner. Early career researchers may find themselves in a position where they decide to undertake a systematic review, for example it may form part or all of a PhD thesis. Those with no prior experience of systematic review may need considerable support and direction getting started with such a project. Here we set out in simple terms how to get started with a systematic review. Discussion: Advice is given on matters such as developing a review protocol, searching using databases and other methods, data extraction, risk of bias assessment and data synthesis including meta-analysis. Signposts to further information and useful resources are also given. Conclusion: A well-conducted systematic review benefits the scientific field by providing a summary of existing evidence and highlighting unanswered questions. For the individual, undertaking a systematic review is also a great opportunity to improve skills in critical appraisal and in synthesising evidence. -
Using Proper Mean Generation Intervals in Modeling of COVID-19
ORIGINAL RESEARCH published: 05 July 2021 doi: 10.3389/fpubh.2021.691262 Using Proper Mean Generation Intervals in Modeling of COVID-19 Xiujuan Tang 1, Salihu S. Musa 2,3, Shi Zhao 4,5, Shujiang Mei 1 and Daihai He 2* 1 Shenzhen Center for Disease Control and Prevention, Shenzhen, China, 2 Department of Applied Mathematics, The Hong Kong Polytechnic University, Hong Kong, China, 3 Department of Mathematics, Kano University of Science and Technology, Wudil, Nigeria, 4 The Jockey Club School of Public Health and Primary Care, Chinese University of Hong Kong, Hong Kong, China, 5 Shenzhen Research Institute of Chinese University of Hong Kong, Shenzhen, China In susceptible–exposed–infectious–recovered (SEIR) epidemic models, with the exponentially distributed duration of exposed/infectious statuses, the mean generation interval (GI, time lag between infections of a primary case and its secondary case) equals the mean latent period (LP) plus the mean infectious period (IP). It was widely reported that the GI for COVID-19 is as short as 5 days. However, many works in top journals used longer LP or IP with the sum (i.e., GI), e.g., >7 days. This discrepancy will lead to overestimated basic reproductive number and exaggerated expectation of Edited by: infection attack rate (AR) and control efficacy. We argue that it is important to use Reza Lashgari, suitable epidemiological parameter values for proper estimation/prediction. Furthermore, Institute for Research in Fundamental we propose an epidemic model to assess the transmission dynamics of COVID-19 Sciences, Iran for Belgium, Israel, and the United Arab Emirates (UAE). -

Epidemiology of and Risk Factors for COVID-19 Infection Among Health Care Workers: a Multi-Centre Comparative Study
International Journal of Environmental Research and Public Health Article Epidemiology of and Risk Factors for COVID-19 Infection among Health Care Workers: A Multi-Centre Comparative Study Jia-Te Wei 1, Zhi-Dong Liu 1, Zheng-Wei Fan 2, Lin Zhao 1,* and Wu-Chun Cao 1,2,* 1 Institute of EcoHealth, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan 250012, Shandong, China; [email protected] (J.-T.W.); [email protected] (Z.-D.L.) 2 State Key Laboratory of Pathogen and Biosecurity, Beijing Institute of Microbiology and Epidemiology, Beijing 100071, China; [email protected] * Correspondence: [email protected] (L.Z.); [email protected] (W.-C.C.) Received: 31 August 2020; Accepted: 28 September 2020; Published: 29 September 2020 Abstract: Healthcare workers (HCWs) worldwide are putting themselves at high risks of coronavirus disease 2019 (COVID-19) by treating a large number of patients while lacking protective equipment. We aim to provide a scientific basis for preventing and controlling the COVID-19 infection among HCWs. We used data on COVID-19 cases in the city of Wuhan to compare epidemiological characteristics between HCWs and non-HCWs and explored the risk factors for infection and deterioration among HCWs based on hospital settings. The attack rate (AR) of HCWs in the hospital can reach up to 11.9% in Wuhan. The time interval from symptom onset to diagnosis in HCWs and non-HCWs dropped rapidly over time. From mid-January, the median time interval of HCW cases was significantly shorter than in non-HCW cases.