Malaria and COVID-19: Common and Different Findings
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

STI Screening Timetable
Patient Education Information from University Health Center’s STI Screening Clinic Page 1 of 1 STI Screening Timetable How long until STI (sexually transmitted infection) screening tests turn positive? How long until STI symptoms might show up? The time between infection and a positive test, or between infection and symptoms, is variable and depends on many factors, including the behavior of the infectious agent, how and where the body is infected, and the state of a person’s immune system and personal health. Many STIs don’t have any symptoms. The incubation period times listed in the chart below are averages only. If you have further questions or concerns, you can schedule an appointment with a clinician at 541-346-2770. STI screening test Window period (time from exposure until Incubation period (time between exposure and screening test turns positive) when symptoms appear) Chlamydia (urine specimen or swab of 1 week most of the time Often no symptoms vagina, rectum, throat) 2 weeks catches almost all 1-3 weeks on average Gonorrhea (urine specimen on swab of 1 week most of the time Often no symptoms, especially vaginal vagina, rectum, throat) 2 weeks catches almost all infections usually within 2-8 days but can be up to 2 weeks Syphilis (blood test, RPR) 1 month catches most Often symptoms too mild to notice 3 months catches almost all 10-90 days average 21 days HIV (oral cheek swab) 1 month catches most Sometimes mild body aches and fever within 1-2 3 months catches almost all weeks then can be months to years HIV (blood test, antigen/antibody -

Malaria History
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site. Copyright 2006, The Johns Hopkins University and David Sullivan. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed. Malariology Overview History, Lifecycle, Epidemiology, Pathology, and Control David Sullivan, MD Malaria History • 2700 BCE: The Nei Ching (Chinese Canon of Medicine) discussed malaria symptoms and the relationship between fevers and enlarged spleens. • 1550 BCE: The Ebers Papyrus mentions fevers, rigors, splenomegaly, and oil from Balantines tree as mosquito repellent. • 6th century BCE: Cuneiform tablets mention deadly malaria-like fevers affecting Mesopotamia. • Hippocrates from studies in Egypt was first to make connection between nearness of stagnant bodies of water and occurrence of fevers in local population. • Romans also associated marshes with fever and pioneered efforts to drain swamps. • Italian: “aria cattiva” = bad air; “mal aria” = bad air. • French: “paludisme” = rooted in swamp. Cure Before Etiology: Mid 17th Century - Three Theories • PC Garnham relates that following: An earthquake caused destruction in Loxa in which many cinchona trees collapsed and fell into small lake or pond and water became very bitter as to be almost undrinkable. Yet an Indian so thirsty with a violent fever quenched his thirst with this cinchona bark contaminated water and was better in a day or two. -

Incubation Period and Other Epidemiological
Journal of Clinical Medicine Article Incubation Period and Other Epidemiological Characteristics of 2019 Novel Coronavirus Infections with Right Truncation: A Statistical Analysis of Publicly Available Case Data 1, 1, 1 1 Natalie M. Linton y , Tetsuro Kobayashi y, Yichi Yang , Katsuma Hayashi , Andrei R. Akhmetzhanov 1 , Sung-mok Jung 1 , Baoyin Yuan 1, Ryo Kinoshita 1 and Hiroshi Nishiura 1,2,* 1 Graduate School of Medicine, Hokkaido University, Kita 15 Jo Nishi 7 Chome, Kita-ku, Sapporo-shi, Hokkaido 060-8638, Japan; [email protected] (N.M.L.); [email protected] (T.K.); [email protected] (Y.Y.); katsuma5miff[email protected] (K.H.); [email protected] (A.R.A.); [email protected] (S.-m.J.); [email protected] (B.Y.); [email protected] (R.K.) 2 Core Research for Evolutional Science and Technology (CREST), Japan Science and Technology Agency, Honcho 4-1-8, Kawaguchi, Saitama 332-0012, Japan * Correspondence: [email protected]; Tel.: +81-11-706-5066 These authors contributed equally to this work. y Received: 25 January 2020; Accepted: 10 February 2020; Published: 17 February 2020 Abstract: The geographic spread of 2019 novel coronavirus (COVID-19) infections from the epicenter of Wuhan, China, has provided an opportunity to study the natural history of the recently emerged virus. Using publicly available event-date data from the ongoing epidemic, the present study investigated the incubation period and other time intervals that govern the epidemiological dynamics of COVID-19 infections. Our results show that the incubation period falls within the range of 2–14 days with 95% confidence and has a mean of around 5 days when approximated using the best-fit lognormal distribution. -

Malaria: Bad for Business Why Investing in Ending Malaria Provides Some of the Highest Economic Returns
Malaria: Bad for business Why investing in ending malaria provides some of the highest economic returns. Malaria’s burden on the health and wealth of nations While huge progress has been made in recent years, one of the most striking signs of the global impact of the 215 million cases of malaria reported last year is that up to 40% of public health spending goes on the disease in the most heavily affected countries. But malaria reaches far beyond public health, taking its toll on households, local and multinational business profits, and national economic development. Critically, annual economic growth in countries with high malaria transmission has historically been lower than in countries without malaria. In some African countries, malaria reduces GDP growth up to an estimated 1.3%. Malaria costs productivity. Adults are forced to be absent from work, children miss school, and households spend disproportionately on health when they can least afford it. But it need not be this way. With developing countries, donors and private sector firms beginning to take real action, we can be the generation that ends malaria for good and boosts prosperity for all. The economic growth penalty Malaria’s impact on national economies Malaria and poverty occupy common ground. Where the burden of malaria is highest, economic prosperity is lowest. We know that poverty can promote malaria transmission, and that malaria causes poverty by blocking economic growth. Research shows that malaria can strain national economics, having a deleterious impact on some nations’ GDP by as much as an estimated 5 - 6%. It keeps households in poverty, discourages domestic and foreign investment and tourism, affects land use patterns, and reduces productivity through lost work days and diminished job performance. -

COVID-19 Surveillance Seminar - July 6, 2020
COVID-19 Surveillance Seminar - July 6, 2020 Leveraging Systems for COVID-19 Surveillance Integrated Disease Surveillance and Response (IDSR), Malaria, and Polio Michelle Sloan, Division of Global Health Protection John Painter, Division of Parasitic Diseases and Malaria Wilbrod Mwanje, African Field Epidemiology Network (AFENET), Uganda cdc.gov coronavirus www.cdc.go /corona irus/2019-nco /global-co id-19 Integrated Disease Surveillance and Response (IDSR) . Integrates common sur eillance acti ities across diseases – Identify, Report, Analyze and Interpret, In estigate and Confirm, Prepare, Respond, Communicate, E aluate – Acti ities linked across community, district, and national le els of the health system . Reporting on country identified priority diseases (e.g. case based, aggregate) . Standardized data collection tools and data reporting to district le el . Thresholds defined for public health response . Impro ed data use through routine data analysis Incorporating COVID-19 into IDSR . Include COVID-19 on country priority disease list . De elop COVID-19 reporting tools – Indi idual case report, aggregate reporting form, contact tracing form . Train sur eillance focal points – Case identification using standard case definition – Immediate reporting of suspect cases . Case-based reporting of cases and deaths (aggregate if resources constrained) . Initiate response strategies based on threshold, for example – In estigation and contact tracing for each indi idual case – Population le el inter entions for clusters and outbreaks Leveraging Other IDSR Data . Monitor existing disease sur eillance for signals – Influenza – Malaria – Other fe er producing diseases . Indicators to analyze – Case and death counts – Trends – Geographical spread – Completeness – Timeliness Leveraging Other Disease Surveillance Strategies . Identify potential signals o erall or by region where there might be missed COVID-19 cases – Malaria sur eillance . -
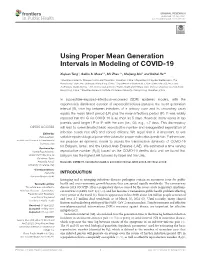
Using Proper Mean Generation Intervals in Modeling of COVID-19
ORIGINAL RESEARCH published: 05 July 2021 doi: 10.3389/fpubh.2021.691262 Using Proper Mean Generation Intervals in Modeling of COVID-19 Xiujuan Tang 1, Salihu S. Musa 2,3, Shi Zhao 4,5, Shujiang Mei 1 and Daihai He 2* 1 Shenzhen Center for Disease Control and Prevention, Shenzhen, China, 2 Department of Applied Mathematics, The Hong Kong Polytechnic University, Hong Kong, China, 3 Department of Mathematics, Kano University of Science and Technology, Wudil, Nigeria, 4 The Jockey Club School of Public Health and Primary Care, Chinese University of Hong Kong, Hong Kong, China, 5 Shenzhen Research Institute of Chinese University of Hong Kong, Shenzhen, China In susceptible–exposed–infectious–recovered (SEIR) epidemic models, with the exponentially distributed duration of exposed/infectious statuses, the mean generation interval (GI, time lag between infections of a primary case and its secondary case) equals the mean latent period (LP) plus the mean infectious period (IP). It was widely reported that the GI for COVID-19 is as short as 5 days. However, many works in top journals used longer LP or IP with the sum (i.e., GI), e.g., >7 days. This discrepancy will lead to overestimated basic reproductive number and exaggerated expectation of Edited by: infection attack rate (AR) and control efficacy. We argue that it is important to use Reza Lashgari, suitable epidemiological parameter values for proper estimation/prediction. Furthermore, Institute for Research in Fundamental we propose an epidemic model to assess the transmission dynamics of COVID-19 Sciences, Iran for Belgium, Israel, and the United Arab Emirates (UAE). -

Strengthening Malaria Surveillance for Data- Driven Decision Making in Mozambique
MALARIA CONSORTIUM PROJECT BRIEF Strengthening malaria surveillance for data- driven decision making in Mozambique Accelerating efforts to reduce the malaria burden by improving data quality and use across all transmission strata Background Country Mozambique Although Mozambique has made some progress in scaling up malaria control activities and aligning its malaria elimination efforts with neighbouring countries Donor Bill & Melinda Gates Foundation in southern Africa over the last decade, it remains the fourth largest contributor of malaria cases globally.[1] Length of project May 2019 – May 2022 To accelerate efforts to reduce the malaria burden, Mozambique urgently needs a fit-for-purpose surveillance system to provide the necessary intelligence to identify Partners bottlenecks in malaria control and elimination activities, target interventions more Clinton Health Access Initiative efficiently and respond when the impact of National Malaria Control Programme Goodbye Malaria/LSDI2 activities is jeopardised. Manhica Health Research Centre Ministry of Health A malaria surveillance system is considered functional and responsive when it World Health Organization can produce evidence-based information from quality data that is routinely used Collaborator for planning and decision making. The 2018 national malaria surveillance system U.S. President’s Malaria Initiative assessment identified the following main obstacles: • poor malaria data quality (DQ) and data use (DU) • lack of an integrated malaria information storage system (iMISS) • -

Prediction of the Incubation Period for COVID-19 and Future Virus Disease Outbreaks Ayal B
Gussow et al. BMC Biology (2020) 18:186 https://doi.org/10.1186/s12915-020-00919-9 RESEARCH ARTICLE Open Access Prediction of the incubation period for COVID-19 and future virus disease outbreaks Ayal B. Gussow†, Noam Auslander*†, Yuri I. Wolf and Eugene V. Koonin* Abstract Background: A crucial factor in mitigating respiratory viral outbreaks is early determination of the duration of the incubation period and, accordingly, the required quarantine time for potentially exposed individuals. At the time of the COVID-19 pandemic, optimization of quarantine regimes becomes paramount for public health, societal well- being, and global economy. However, biological factors that determine the duration of the virus incubation period remain poorly understood. Results: We demonstrate a strong positive correlation between the length of the incubation period and disease severity for a wide range of human pathogenic viruses. Using a machine learning approach, we develop a predictive model that accurately estimates, solely from several virus genome features, in particular, the number of protein-coding genes and the GC content, the incubation time ranges for diverse human pathogenic RNA viruses including SARS-CoV-2. The predictive approach described here can directly help in establishing the appropriate quarantine durations and thus facilitate controlling future outbreaks. Conclusions: The length of the incubation period in viral diseases strongly correlates with disease severity, emphasizing the biological and epidemiological importance of the incubation period. Perhaps, surprisingly, incubation times of pathogenic RNA viruses can be accurately predicted solely from generic features of virus genomes. Elucidation of the biological underpinnings of the connections between these features and disease progression can be expected to reveal key aspects of virus pathogenesis. -

Sexually Transmitted Infections Treatment Guidelines, 2021
Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 70 / No. 4 July 23, 2021 Sexually Transmitted Infections Treatment Guidelines, 2021 U.S. Department of Health and Human Services Centers for Disease Control and Prevention Recommendations and Reports CONTENTS Introduction ............................................................................................................1 Methods ....................................................................................................................1 Clinical Prevention Guidance ............................................................................2 STI Detection Among Special Populations ............................................... 11 HIV Infection ......................................................................................................... 24 Diseases Characterized by Genital, Anal, or Perianal Ulcers ............... 27 Syphilis ................................................................................................................... 39 Management of Persons Who Have a History of Penicillin Allergy .. 56 Diseases Characterized by Urethritis and Cervicitis ............................... 60 Chlamydial Infections ....................................................................................... 65 Gonococcal Infections ...................................................................................... 71 Mycoplasma genitalium .................................................................................... 80 Diseases Characterized -

The Columbian Exchange: a History of Disease, Food, and Ideas
Journal of Economic Perspectives—Volume 24, Number 2—Spring 2010—Pages 163–188 The Columbian Exchange: A History of Disease, Food, and Ideas Nathan Nunn and Nancy Qian hhee CColumbianolumbian ExchangeExchange refersrefers toto thethe exchangeexchange ofof diseases,diseases, ideas,ideas, foodfood ccrops,rops, aandnd populationspopulations betweenbetween thethe NewNew WorldWorld andand thethe OldOld WWorldorld T ffollowingollowing thethe voyagevoyage ttoo tthehe AAmericasmericas bbyy ChristoChristo ppherher CColumbusolumbus inin 1492.1492. TThehe OldOld WWorld—byorld—by wwhichhich wwee mmeanean nnotot jjustust EEurope,urope, bbutut tthehe eentirentire EEasternastern HHemisphere—gainedemisphere—gained fromfrom tthehe CColumbianolumbian EExchangexchange iinn a nnumberumber ooff wways.ays. DDiscov-iscov- eeriesries ooff nnewew ssuppliesupplies ofof metalsmetals areare perhapsperhaps thethe bestbest kknown.nown. BButut thethe OldOld WWorldorld aalsolso ggainedained newnew staplestaple ccrops,rops, ssuchuch asas potatoes,potatoes, sweetsweet potatoes,potatoes, maize,maize, andand cassava.cassava. LessLess ccalorie-intensivealorie-intensive ffoods,oods, suchsuch asas tomatoes,tomatoes, chilichili peppers,peppers, cacao,cacao, peanuts,peanuts, andand pineap-pineap- pplesles wwereere aalsolso iintroduced,ntroduced, andand areare nownow culinaryculinary centerpiecescenterpieces inin manymany OldOld WorldWorld ccountries,ountries, namelynamely IItaly,taly, GGreece,reece, andand otherother MediterraneanMediterranean countriescountries (tomatoes),(tomatoes), -
Intersecting Infections of Public Health Significance Page I Intersecting Infections of Public Health Significance
Intersecting Infections of Public Health Significance Page i Intersecting Infections of Public Health Significance The Epidemiology of HIV, Viral Hepatitis, Sexually Transmitted Diseases, and Tuberculosis in King County 2008 Intersecting Infections of Public Health Significance was supported by a cooperative agreement from the Centers for Disease Control and Prevention Published December 2009 Alternate formats of this report are available upon request Intersecting Infections of Public Health Significance Page ii David Fleming, MD, Director Jeffrey Duchin, MD, Director, Communicable Disease Epidemiology & Immunization Program Matthew Golden, MD, MPH, Director, STD Program Masa Narita, MD, Director, TB Program Robert Wood, MD, Director, HIV/AIDS Program Prepared by: Hanne Thiede, DVM, MPH Elizabeth Barash, MPH Jim Kent, MS Jane Koehler, DVM, MPH Other contributors: Amy Bennett, MPH Richard Burt, PhD Susan Buskin, PhD, MPH Christina Thibault, MPH Roxanne Pieper Kerani, PhD Eyal Oren, MS Shelly McKeirnan, RN, MPH Amy Laurent, MSPH Cover design and formatting by Tanya Hunnell The report is available at www.kingcounty.gov/health/hiv For additional copies of this report contact: HIV/AIDS Epidemiology Program Public Health – Seattle & King County 400 Yesler Way, 3rd Floor Seattle, WA 98104 206-296-4645 Intersecting Infections of Public Health Significance Page iii Table of Contents INDEX OF TABLES AND FIGURES ········································································ vi EXECUTIVE SUMMARY ······················································································ -

Chlamydial Genital Infection(Chlamydia Trachomatis)
Chlamydial Genital Infection (Chlamydia trachomatis) February 2003 1) THE DISEASE AND ITS EPIDEMIOLOGY A. Etiologic Agent Chlamydial genital infection (CGI) is caused by the obligate, intracellular bacterium Chlamydia trachomatis immunotypes D through K. B. Clinical Description and Laboratory Diagnosis A sexually transmitted genital infection that manifests in males primarily as urethritis and in females as mucopurulent cervicitis. Clinical manifestations are difficult to distinguish from gonorrhea. Males may present with a mucopurulent discharges of scanty to moderate quantity, urethral itching and dysuria. Asymptomatic infection may be found in 1%-25% of sexually active men. Possible complications include epididymitis, infertility and Reiter syndrome. Anorectal intercourse may result in chlamydial proctitis. Women frequently present with a mucopurulent endocervical discharge including edema, erythema and easily induced endocervical bleeding. However, most women with endocervical or urethral infections are asymptomatic. Possible complications include salpingitis with subsequent risk of infertility and ectopic pregnancy. Asymptomatic chronic infections of the endometrium and fallopian tubes may lead to the same outcomes. Less frequent manifestations include bartholinitis, urethral syndrome with dysuria and pyuria, perihepatitis (Fitz-Hugh-Curtis syndrome), and proctitis. Infection during pregnancy may result in premature rupture of membranes and preterm delivery and conjunctival and pneumonic infection of the newborn. Laboratory diagnosis is based upon the identification of Chlamydia in intraurethral or endocervical smear by direct immunofluorescence test, enzyme immunoassay, DNA probe, and nucleic acid amplification test (NAAT) or cell culture. NAAT can be used with urine specimens. C. Vectors and Reservoirs Humans. D. Modes of Transmission By sexual contact and through perinatal exposure to the mother’s infected cervix.