Adaptive Designs in Clinical Trials: Why Use Them, and How to Run and Report Them Philip Pallmann1* , Alun W
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adaptive Clinical Trials: an Introduction
Adaptive clinical trials: an introduction What are the advantages and disadvantages of adaptive clinical trial designs? How and why were Introduction adaptive clinical Adaptive clinical trial design is trials developed? becoming a hot topic in healthcare research, with some researchers In 2004, the FDA published a report arguing that adaptive trials have the on the problems faced by the potential to get new drugs to market scientific community in developing quicker. In this article, we explain new medical treatments.2 The what adaptive trials are and why they report highlighted that the pace of were developed, and we explore both innovation in biomedical science is the advantages of adaptive designs outstripping the rate of advances and the concerns being raised by in the available technologies and some in the healthcare community. tools for evaluating new treatments. Outdated tools are being used to assess new treatments and there What are adaptive is a critical need to improve the effectiveness and efficiency of clinical trials? clinical trials.2 The current process for developing Adaptive clinical trials enable new treatments is expensive, takes researchers to change an aspect a long time and in some cases, the of a trial design at an interim development process has to be assessment, while controlling stopped after significant amounts the rate of type 1 errors.1 Interim of time and resources have been assessments can help to determine invested.2 In 2006, the FDA published whether a trial design is the most a “Critical Path Opportunities -

Evolution of Clinical Trials Throughout History
Evolution of clinical trials throughout history Emma M. Nellhaus1, Todd H. Davies, PhD1 Author Affiliations: 1. Office of Research and Graduate Education, Marshall University Joan C. Edwards School of Medicine, Huntington, West Virginia The authors have no financial disclosures to declare and no conflicts of interest to report. Corresponding Author: Todd H. Davies, PhD Director of Research Development and Translation Marshall University Joan C. Edwards School of Medicine Huntington, West Virginia Email: [email protected] Abstract The history of clinical research accounts for the high ethical, scientific, and regulatory standards represented in current practice. In this review, we aim to describe the advances that grew from failures and provide a comprehensive view of how the current gold standard of clinical practice was born. This discussion of the evolution of clinical trials considers the length of time and efforts that were made in order to designate the primary objective, which is providing improved care for our patients. A gradual, historic progression of scientific methods such as comparison of interventions, randomization, blinding, and placebos in clinical trials demonstrates how these techniques are collectively responsible for a continuous advancement of clinical care. Developments over the years have been ethical as well as clinical. The Belmont Report, which many investigators lack appreciation for due to time constraints, represents the pinnacle of ethical standards and was developed due to significant misconduct. Understanding the history of clinical research may help investigators value the responsibility of conducting human subjects’ research. Keywords Clinical Trials, Clinical Research, History, Belmont Report In modern medicine, the clinical trial is the gold standard and most dominant form of clinical research. -

Quasi-Experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: a Systematic Review
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Infect Control Manuscript Author Hosp Epidemiol Manuscript Author . Author manuscript; available in PMC 2019 November 12. Published in final edited form as: Infect Control Hosp Epidemiol. 2018 February ; 39(2): 170–176. doi:10.1017/ice.2017.296. Quasi-experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: A Systematic Review Rotana Alsaggaf, MS, Lyndsay M. O’Hara, PhD, MPH, Kristen A. Stafford, PhD, MPH, Surbhi Leekha, MBBS, MPH, Anthony D. Harris, MD, MPH, CDC Prevention Epicenters Program Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, Maryland. Abstract OBJECTIVE.—A systematic review of quasi-experimental studies in the field of infectious diseases was published in 2005. The aim of this study was to assess improvements in the design and reporting of quasi-experiments 10 years after the initial review. We also aimed to report the statistical methods used to analyze quasi-experimental data. DESIGN.—Systematic review of articles published from January 1, 2013, to December 31, 2014, in 4 major infectious disease journals. METHODS.—Quasi-experimental studies focused on infection control and antibiotic resistance were identified and classified based on 4 criteria: (1) type of quasi-experimental design used, (2) justification of the use of the design, (3) use of correct nomenclature to describe the design, and (4) statistical methods used. RESULTS.—Of 2,600 articles, 173 (7%) featured a quasi-experimental design, compared to 73 of 2,320 articles (3%) in the previous review (P<.01). Moreover, 21 articles (12%) utilized a study design with a control group; 6 (3.5%) justified the use of a quasi-experimental design; and 68 (39%) identified their design using the correct nomenclature. -

A Guide to Systematic Review and Meta-Analysis of Prediction Model Performance
RESEARCH METHODS AND REPORTING A guide to systematic review and meta-analysis of prediction model performance Thomas P A Debray,1,2 Johanna A A G Damen,1,2 Kym I E Snell,3 Joie Ensor,3 Lotty Hooft,1,2 Johannes B Reitsma,1,2 Richard D Riley,3 Karel G M Moons1,2 1Cochrane Netherlands, Validation of prediction models is diagnostic test accuracy studies. Compared to therapeu- University Medical Center tic intervention and diagnostic test accuracy studies, Utrecht, PO Box 85500 Str highly recommended and increasingly there is limited guidance on the conduct of systematic 6.131, 3508 GA Utrecht, Netherlands common in the literature. A systematic reviews and meta-analysis of primary prognosis studies. 2Julius Center for Health review of validation studies is therefore A common aim of primary prognostic studies con- Sciences and Primary Care, cerns the development of so-called prognostic predic- University Medical Center helpful, with meta-analysis needed to tion models or indices. These models estimate the Utrecht, PO Box 85500 Str 6.131, 3508 GA Utrecht, summarise the predictive performance individualised probability or risk that a certain condi- Netherlands of the model being validated across tion will occur in the future by combining information 3Research Institute for Primary from multiple prognostic factors from an individual. Care and Health Sciences, Keele different settings and populations. This Unfortunately, there is often conflicting evidence about University, Staffordshire, UK article provides guidance for the predictive performance of developed prognostic Correspondence to: T P A Debray [email protected] researchers systematically reviewing prediction models. For this reason, there is a growing Additional material is published demand for evidence synthesis of (external validation) online only. -

U.S. Investments in Medical and Health Research and Development 2013 - 2017 Advocacy Has Helped Bring About Five Years of Much-Needed Growth in U.S
Fall 2018 U.S. Investments in Medical and Health Research and Development 2013 - 2017 Advocacy has helped bring about five years of much-needed growth in U.S. medical and health research investment. More advocacy is critical now to ensure our nation steps up in response to health threats that we can—we must—overcome. More Than Half Favor Doubling Federal Spending on Medical Research Do you favor or oppose doubling federal spending on medical research over the next five years? 19% Not Sure 23% 8% Strongly favor Strongly oppose 16% 35% Somewhat oppose Somewhat favor Source: A Research!America survey of U.S. adults conducted in partnership with Zogby Analytics in January 2018. Research!America 3 Introduction Investment1 in medical and health research and development (R&D) in the U.S. grew by $38.8 billion or 27% from 2013 to 2017. Industry continues to invest more than any other sector, accounting for 67% of total spending in 2017, followed by the federal government at 22%. Federal investments increased from 2016 to 2017, the second year of growth after a dip from 2014 to 2015. Overall, federal investment increased by $6.1 billion or 18.4% from 2013 to 2017, but growth has been uneven across federal health agencies. Investment by other sectors, including academic and research institutions, foundations, state and local governments, and voluntary health associations and professional societies, also increased from 2013 to 2017. Looking ahead, medical and health R&D spending is expected to move in an upward trajectory in 2018 but will continue to fall short relative to the health and economic impact of major health threats. -
Is It Worthwhile Including Observational Studies in Systematic Reviews of Effectiveness?
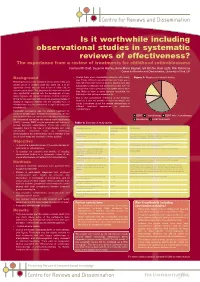
CRD_mcdaid05_Poster.qxd 13/6/05 5:12 pm Page 1 Is it worthwhile including observational studies in systematic reviews of effectiveness? The experience from a review of treatments for childhood retinoblastoma Catriona Mc Daid, Suzanne Hartley, Anne-Marie Bagnall, Gill Ritchie, Kate Light, Rob Riemsma Centre for Reviews and Dissemination, University of York, UK Background • Overall there were considerable problems with quality Figure 1: Mapping of included studies (see Table). Without randomised allocation there was a Retinoblastoma is a rare malignant tumour of the retina and high risk of selection bias in all studies. Studies were also usually occurs in children under two years old. It is an susceptible to detection and performance bias, with the aggressive tumour that can lead to loss of vision and, in retrospective studies particularly susceptible as they were extreme cases, death. The prognoses for vision and survival less likely to have a study protocol specifying the have significantly improved with the development of more intervention and outcome assessments. timely diagnosis and improved treatment methods. Important • Due to the considerable limitations of the evidence clinical factors associated with prognosis are age and stage of identified, it was not possible to make meaningful and disease at diagnosis. Patients with the hereditary form of robust conclusions about the relative effectiveness of retinoblastoma may be predisposed to significant long-term different treatment approaches for childhood complications. retinoblastoma. Historically, enucleation was the standard treatment for unilateral retinoblastoma. In bilateral retinoblastoma, the eye ■ ■ ■ with the most advanced tumour was commonly removed and EBRT Chemotherapy EBRT with Chemotherapy the contralateral eye treated with external beam radiotherapy ■ Enucleation ■ Local Treatments (EBRT). -

Clinical Research Services
Clinical Research Services Conducting efficient, innovative clinical research from initial planning to closeout WHY LEIDOS LIFE SCIENCES? In addition to developing large-scale technology programs for U.S. federal f Leidos has expertise agencies with a focus on health, Leidos provides a broad range of clinical supporting all product services and solutions to researchers, product sponsors, U.S. government development phases agencies, and other biomedical enterprises, hospitals, and health systems. for vaccines, drugs, and Our broad research experience enables us to support programs throughout biotherapeutics the development life cycle: from concept through the exploratory, f Leidos understands the development, pre-clinical, and clinical phases, as well as with product need to control clinical manufacturing and launching. Leidos designs and develops customized project scope, timelines, solutions that support groundbreaking medical research, optimize business and cost while remaining operations, and expedite the discovery of safe and effective medical flexible amidst shifting products. We apply our technical knowledge and experience in selecting research requirements institutions, clinical research organizations, and independent research f Leidos remains vendor- facilities to meet the specific needs of each clinical study. We also manage neutral while fostering and team integration, communication, and contracts throughout the project. managing collaborations Finally, Leidos has a proven track record of ensuring that research involving with -

How to Get Started with a Systematic Review in Epidemiology: an Introductory Guide for Early Career Researchers
Denison et al. Archives of Public Health 2013, 71:21 http://www.archpublichealth.com/content/71/1/21 ARCHIVES OF PUBLIC HEALTH METHODOLOGY Open Access How to get started with a systematic review in epidemiology: an introductory guide for early career researchers Hayley J Denison1*†, Richard M Dodds1,2†, Georgia Ntani1†, Rachel Cooper3†, Cyrus Cooper1†, Avan Aihie Sayer1,2† and Janis Baird1† Abstract Background: Systematic review is a powerful research tool which aims to identify and synthesize all evidence relevant to a research question. The approach taken is much like that used in a scientific experiment, with high priority given to the transparency and reproducibility of the methods used and to handling all evidence in a consistent manner. Early career researchers may find themselves in a position where they decide to undertake a systematic review, for example it may form part or all of a PhD thesis. Those with no prior experience of systematic review may need considerable support and direction getting started with such a project. Here we set out in simple terms how to get started with a systematic review. Discussion: Advice is given on matters such as developing a review protocol, searching using databases and other methods, data extraction, risk of bias assessment and data synthesis including meta-analysis. Signposts to further information and useful resources are also given. Conclusion: A well-conducted systematic review benefits the scientific field by providing a summary of existing evidence and highlighting unanswered questions. For the individual, undertaking a systematic review is also a great opportunity to improve skills in critical appraisal and in synthesising evidence. -

Guidelines for Reporting Meta-Epidemiological Methodology Research
EBM Primer Evid Based Med: first published as 10.1136/ebmed-2017-110713 on 12 July 2017. Downloaded from Guidelines for reporting meta-epidemiological methodology research Mohammad Hassan Murad, Zhen Wang 10.1136/ebmed-2017-110713 Abstract The goal is generally broad but often focuses on exam- Published research should be reported to evidence users ining the impact of certain characteristics of clinical studies on the observed effect, describing the distribu- Evidence-Based Practice with clarity and transparency that facilitate optimal tion of research evidence in a specific setting, exam- Center, Mayo Clinic, Rochester, appraisal and use of evidence and allow replication Minnesota, USA by other researchers. Guidelines for such reporting ining heterogeneity and exploring its causes, identifying are available for several types of studies but not for and describing plausible biases and providing empirical meta-epidemiological methodology studies. Meta- evidence for hypothesised associations. Unlike classic Correspondence to: epidemiological studies adopt a systematic review epidemiology, the unit of analysis for meta-epidemio- Dr Mohammad Hassan Murad, or meta-analysis approach to examine the impact logical studies is a study, not a patient. The outcomes Evidence-based Practice Center, of certain characteristics of clinical studies on the of meta-epidemiological studies are usually not clinical Mayo Clinic, 200 First Street 6–8 observed effect and provide empirical evidence for outcomes. SW, Rochester, MN 55905, USA; hypothesised associations. The unit of analysis in meta- In this guide, we adapt the items used in the PRISMA murad. mohammad@ mayo. edu 9 epidemiological studies is a study, not a patient. The statement for reporting systematic reviews and outcomes of meta-epidemiological studies are usually meta-analysis to fit the setting of meta- epidemiological not clinical outcomes. -

Adaptive Design: a Review of the Technical, Statistical, and Regulatory Aspects of Implementation in a Clinical Trial
Adaptive Design: A Review of the Technical, Statistical, and Regulatory Aspects of Implementation in a Clinical Trial 1,2 1 Franck Pires Cerqueira, MSc , Angelo Miguel Cardoso Jesus, PhD , and Maria Dulce 2 Cotrim, PhD 1 Polytechnic Institute of Porto School of Health, Department of Pharmacy Porto, Portugal 2 Pharmacy Faculty of the University of Coimbra, Department of Pharmacology Coimbra, Portugal Abstract Background: In an adaptive trial, the researcher may have the option of responding to interim safety and efficacy data in a number of ways, including narrowing the study focus or increasing the number of subjects, balancing treatment allocation or different forms of randomization based on responses of subjects prior to treatment. This research aims at compiling the technical, statistical, and regulatory implications of the employment of adaptive design in a clinical trial. Methods: Review of adaptive design clinical trials in Medline, PubMed, EU Clinical Trials Register, and ClinicalTrials.gov. Phase I and seamless phase I/II trials were excluded. We selected variables extracted from trials that included basic study characteristics, adaptive design features, size and use of inde- pendent data-monitoring committees (DMCs), and blinded interim analysis. Results: The research retrieved 336 results, from which 78 were selected for analysis. Sixty-seven were published articles, and 11 were guidelines, papers, and regulatory bills. The most prevalent type of adaptation was the seamless phase II/III design 23.1%, followed by adaptive dose progression 19.2%, pick the winner / drop the loser 16.7%, sample size re-estimation 10.3%, change in the study objective 9.0%, adaptive sequential design 9.0%, adaptive randomization 6.4%, biomarker adaptive design 3.8%, and endpoint adaptation 2.6%. -
3 Regulatory Aspects in Using Surrogate Markers in Clinical Trials
3 Regulatory Aspects in Using Surrogate Markers in Clinical Trials Aloka Chakravarty 3.1 Introduction and Motivation Surrogate marker plays an important role in the regulatory decision pro- cesses in drug approval. The possibility of reduced sample size or trial duration when a distal clinical endpoint is replaced by a more proximal one hold real benefit in terms of reaching the intended patient population faster, cheaper, and safer as well as a better characterization of the efficacy profile. In situations where endpoint measurements have competing risks or are invasive in nature, certain latitude in measurement error can be accepted by deliberately choosing an alternate endpoint in compensation for a better quality of life or for ease of measurement. 3.1.1 Definitions and Their Regulatory Ramifications Over the years, many authors have given various definitions for a surrogate marker. Some of the operational ramifications of these definitions will be examined in their relationship to drug development. Wittes, Lakatos, and Probstfield (1989) defined surrogate endpoint sim- ply as “an endpoint measured in lieu of some so-called ‘true’ endpoint.” While it provides the core, this definition does not provide any operational motivation. Ellenberg and Hamilton (1989) provides this basis by stating: “investigators use surrogate endpoints when the endpoint of interest is too difficult and/or expensive to measure routinely and when they can define some other, more readily measurable endpoint, which is sufficiently well correlated with the first to justify its use as a substitute.” This paved the way to a statistical definition of a surrogate endpoint by Prentice (1989): 14 Aloka Chakravarty “a response variable for which a test of null hypothesis of no relationship to the treatment groups under comparison is also a valid test of the cor- responding null hypothesis based on the true endpoint.” This definition, also known as the Prentice Criteria, is often very hard to verify in real-life clinical trials. -

Good Statistical Practices for Contemporary Meta-Analysis: Examples Based on a Systematic Review on COVID-19 in Pregnancy
Review Good Statistical Practices for Contemporary Meta-Analysis: Examples Based on a Systematic Review on COVID-19 in Pregnancy Yuxi Zhao and Lifeng Lin * Department of Statistics, Florida State University, Tallahassee, FL 32306, USA; [email protected] * Correspondence: [email protected] Abstract: Systematic reviews and meta-analyses have been increasingly used to pool research find- ings from multiple studies in medical sciences. The reliability of the synthesized evidence depends highly on the methodological quality of a systematic review and meta-analysis. In recent years, several tools have been developed to guide the reporting and evidence appraisal of systematic reviews and meta-analyses, and much statistical effort has been paid to improve their methodological quality. Nevertheless, many contemporary meta-analyses continue to employ conventional statis- tical methods, which may be suboptimal compared with several alternative methods available in the evidence synthesis literature. Based on a recent systematic review on COVID-19 in pregnancy, this article provides an overview of select good practices for performing meta-analyses from sta- tistical perspectives. Specifically, we suggest meta-analysts (1) providing sufficient information of included studies, (2) providing information for reproducibility of meta-analyses, (3) using appro- priate terminologies, (4) double-checking presented results, (5) considering alternative estimators of between-study variance, (6) considering alternative confidence intervals, (7) reporting predic- Citation: Zhao, Y.; Lin, L. Good tion intervals, (8) assessing small-study effects whenever possible, and (9) considering one-stage Statistical Practices for Contemporary methods. We use worked examples to illustrate these good practices. Relevant statistical code Meta-Analysis: Examples Based on a is also provided.