Using a Quality Improvement Approach in Facilities and Communities in Ghana: Enhancing Nutrition Within the First 1,000 Days
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cosmetics and Personal Care PRODUCTS CLUSTER Diagnostic
June 2020 1 Readers Guide: This is a combination of two reports on a diagnostic study on the cosmetics and personal care value chains in Ghana. The first part of the report focused on the southern and middle clusters. The scope of the Cosmetics and Personal Care Products (CPCP) CDS was preceded by a complete Value Chain Analysis (VCA) of the sector. The diagnostic assessment was to validate the issues identified from the VCA. The CDS covered two selected clusters (i.e. cosmetics products production and black soap processing) within the middle and southern belts of Ghana. Read details of the Southern and Middle cluster report via link: Southern and Middle Cluster diagnostic report The study on the Northern Cosmetics cluster focuses on the cosmetic value chain that uses as part of its raw materials, shea butter, baobab oil, moringa oil and other indigenous oils to formulate different kinds of cosmetic products. The study was limited to only two regions in northern Ghana namely; Northern Region and Upper East Region although the other northern regions (Upper West, North-East and Savannah) also produce the same quantities and quality of shea nuts and butter. Read details of the Northern Cosmetics Cluster report via the link: Northern cosmetic diagnostic study Thank you. 2 Southern and Middle Cluster Report Southern and Middle Clusters Cosmetics Diagnostic Study Report 3 Table of Contents List of Figures and Tables.......................................................................................................... 6 Table of Abbreviations -
Composite Budget for 2020-2023 Programme Based
Table of Contents PART A: STRATEGIC OVERVIEW ...................................................................................................... 3 1. ESTABLISHMENT OF THE DISTRICT ........................................................................................ 3 2. VISION ................................................................................................................................................ 3 3. MISSION ............................................................................................................................................. 3 REPUBLIC OF GHANA 4. GOALS................................................................................................................................................. 4 5. CORE FUNCTIONS .......................................................................................................................... 4 6. DISTRICT ECONOMY ...................................................................................................................... 5 COMPOSITE BUDGET a. MARKET CENTER ............................................................................................................................ 6 7. KEY ACHIEVEMENTS IN 2019 .................................................................................................... 10 8. REVENUE AND EXPENDITURE PERFORMANCE ................................................................. 11 FOR 2020-2023 a. REVENUE ........................................................................................................................................ -
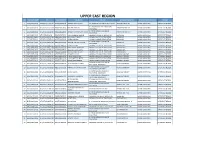
Upper East Region S.No Index Number Ntc Nss Number Full Name College School Posted To: Sponsorship District Region
UPPER EAST REGION S.NO INDEX_NUMBER NTC NSS_NUMBER FULL_NAME COLLEGE SCHOOL POSTED TO: SPONSORSHIP_DISTRICT REGION 1 SACE/0006/2018 NTC/GTLE/11319/18 NSSGTG7079518 ALBERTA ABULISONGA ST. AMBROSE COLLEGE OF EDUCATION ABANDE MEMO JHS BAWKU MUNICIPAL UPPER EAST REGION ST. BOSCO'S COLLEGE EDUCATION, 2 SBCE/0016/2018 NTC/GTLE/11225/18 NSSGTG6354818 RICHARD AKOLGO ABANDE MEMO JHS BAWKU MUNICIPAL UPPER EAST REGION NAVRONGO ST. JOHN BOSCO'S COLLEGE OF 3 SBCE/0058/2018 NTC/GTLE/04330/18 NSSGTG6352618 AYAMGA AKARIYAMBIRE ISAAC ABANDE MEMO JHS BAWKU MUNICIPAL UPPER EAST REGION EDUCATION 4 GBCE/0432/2018 GTLE/NR00580/19 NSSGTG7427018 SAANI ZUMBILA IBRAHIM GBEWAA COLLEGE OF EDUCATION BADOR JHS BAWKU MUNICIPAL UPPER EAST REGION 5 JACE/0197/2018 NTC/GTLE/23474/18 NSSGTG8077018 AHLI SAMUEL KWASI JASIKAN COLLEGE OF EDUCATION BADOR JHS BAWKU MUNICIPAL UPPER EAST REGION 6 JACE/0357/2018 NTC/GTLE/05297/18 NSSGTG6608618 AIKENS OWUANI JASIKAN COLLEGE OF EDUCATION BADOR JHS BAWKU MUNICIPAL UPPER EAST REGION ST. JOHN BOSCO'S COLLEGE OF 7 SBCE/0027/2018 NTC/GTLE/10064/18 NSSGTG6344718 ANYAGRI ABUGBIL ALFRED BADOR JHS BAWKU MUNICIPAL UPPER EAST REGION EDUCATION 8 GBCE/0298/2018 NTC/GTLE/19813/18 NSSGTG7446318 JIBREELA ISSAH GBEWAA COLLEGE OF EDUCATION BARIBARI JHS BAWKU MUNICIPAL UPPER EAST REGION 9 GBCE/0344/2018 NTC/GTLE/09615/18 NSSGTG7431218 MOHAMMED MANSURA GBEWAA COLLEGE OF EDUCATION BARIBARI JHS BAWKU MUNICIPAL UPPER EAST REGION 10 GBCE/0354/2018 NTC/GTLE/04736/18 NSSGTG6637918 ASSAMA-U MUSTAPHA GBEWAA COLLEGE OF EDUCATION BARIBARI JHS BAWKU MUNICIPAL UPPER -

2021 PES Field Officer's Manual Download
2021 POPULATION AND HOUSING CENSUS POST ENUMERATION SURVEY (PES) FIELD OFFICER’S MANUAL STATISTICAL SERVICE, ACCRA July, 2021 1 Table of Content LIST OF ABBREVIATIONS ..................................................................................... 11 INTRODUCTION ........................................................................................................ 12 CHAPTER 1 ................................................................................................................. 13 1. THE CONCEPT OF PES AND OVERVIEW OF CENSUS EVALUATION ........................ 13 1.1 What is a Population census? .................................................................................................. 13 1.2 Why are we conducting the Census? ...................................................................................... 13 1.3. Census errors .............................................................................................................................. 13 1.3.1. Omissions ................................................................................................................................. 14 1.3.2. Duplications ............................................................................................................................. 14 1.3.3. Erroneous inclusions ............................................................................................................... 15 1.3.4. Gross versus net error ............................................................................................................ -

USAID ADVANCE FY16 Q2 Report
Agricultural Development and Value Chain Enhancement Project (ADVANCE) FY16 Quarterly Report – Q2 SUBMITTED TO: Pearl Ackah AOR, USAID/GHANA P.O. Box 1630 Accra, Ghana [email protected] SUBMITTED BY: ACDI/VOCA Emmanuel Dormon Chief of Party P.O. Box KD 138 Accra, Ghana [email protected] WITH: Association of Church Development Projects (ACDEP) PAB Consult TechnoServe May 3, 2016 This report covers activities under USAID Cooperative Agreement No. AID-641-A-14-00001 Contents Acronyms................................................................................................................................................ iii Executive summary ................................................................................................................................. 1 1 Introduction .................................................................................................................................... 2 2 Collaboration with Other Programs and MoFA ............................................................................... 2 2.1 Collaboration with Projects and Organizations ....................................................................... 2 2.2 Collaboration with Ministry of Food and Agriculture (MOFA) ................................................. 5 3 Key Results ...................................................................................................................................... 5 3.1 Direct Project Beneficiaries .................................................................................................... -

Analysis of Anti-Poverty Interventions in Northern Ghana
Participatory Monitoring and Evaluation: A Meta- Analysis of Anti-Poverty Interventions in Northern Ghana By Obure, Jerim Otieno (Student No. 5762936) A Thesis submitted to the International School of Humanities and Social Sciences in partial fulfillment of the requirements for the Degree of Master of Science (International Development Studies) of The University of Amsterdam University of Amsterdam August, 2008 i DECLARATION This Thesis is my original work and has not been presented for examination in any study programme of any institution or University. No part of this Thesis may be reproduced without permission of the author and/ or that of The University of Amsterdam. __________________________ ________________________________ OBURE JERIM OTIENO DATE This Thesis has been submitted for examination with my approval as the University Supervisor. _________________________ ___________________________ PROF. TON DIETZ Date (First Supervisor) _________________________ ____________________________ DR. FRED ZAAL Date (Second Supervisor) ii DEDICATION Dedicated to my brother, Frankline Obure and my fianceé Patricia Ong’wen, in recognition of their special perseverance, encouragements and support during my times away from home as I pursued this degree. My special respect and love to both of you!! “Courage and Perseverance have a magical talisman before which difficulties disappear and obstacles vanish into the air” John Quincy Adams (1767 – 1848) iii ACKNOWLEDGEMENTS First and foremost, I express my gratitude to the Almighty God for His providences that have made me get to this accomplishment. The programme has been demanding with enormous resource requirements, but by God’s unfailing blessings I have made it through. Great is Thy faithfulness! I am profoundly grateful to Prof. Ton Dietz and Dr. -

Regreening Africa Ghana News 2019 Edition Brief from Project Manager
Regreening Africa Ghana News 2019 edition Brief from Project Manager Over the years, acute and prolonged dry farmer groups on regreening approaches and seasons, overgrazing, rampant bush fires and introducing the same to new .members and indiscreet felling of trees have translated to communities in targeted districts. increased decline in forest cover, loss of indigenous biodiversity and decreased soil 2. Interactions with policy makers through fertility. multi-stakeholder and advocacy campaigns The second approach encourages champion Thankfully, simple restoration practices promoted farmers and community leaders to communicate by the Regreening Africa project are improving the benefits enjoyed since adopting regreening livelihoods, food security and resilience to approaches to policy makers. This is to facilitate climate change for smallholder farmers in Garu advancement of environmental policies to favour Tempane, Bawku and Mion Districts. land restoration, especially with beneficiaries in mind. An example is a multi-level stakeholder The two implementing partners, World Vision workshop held in Tamale from 26 to 28 Ghana and Catholic Relief Services (CRS) made November 2018, courtesy of ICRAF's SHARED giant strides in the second year of (Stakeholder Engagement to Risk-Informed implementation. With technical support from Decision Making) team. World Agroforestry (ICRAF), the ambitious target of restoring 90,000 hectares may be within Currently, 16,863 hectares are under various reach. The team attributes progress to the forms of restoration through agroforestry and following approaches: Farmer-Managed Natural Regeneration approaches, with 7,495 households adopting. 1. Direct intervention with communities in However, the team needs to create awareness of three districts these approaches to have as many stakeholders This approach comprises of training farmers and and communities on board. -
Report of the Auditor General on the Accounts of District Assemblies For
Our Vision Our Vision is to become a world-class Supreme Audit I n s t i t u t i o n d e l i v e r i n g professional, excellent and cost-effective services. REPUBLIC OF GHANA REPORT OF THE AUDITOR GENERAL ON THE ACCOUNTS OF DISTRICT ASSEMBLIES FOR THE FINANCIAL YEAR ENDED 31 DECEMBER 2019 This report has been prepared under Section 11 of the Audit Service Act, 2000 for presentation to Parliament in accordance with Section 20 of the Act. Johnson Akuamoah Asiedu Acting Auditor General Ghana Audit Service 21 October 2020 This report can be found on the Ghana Audit Service website: www.ghaudit.org For further information about the Ghana Audit Service, please contact: The Director, Communication Unit Ghana Audit Service Headquarters Post Office Box MB 96, Accra. Tel: 0302 664928/29/20 Fax: 0302 662493/675496 E-mail: [email protected] Location: Ministries Block 'O' © Ghana Audit Service 2020 TRANSMITTAL LETTER Ref. No.: AG//01/109/Vol.2/144 Office of the Auditor General P.O. Box MB 96 Accra GA/110/8787 21 October 2020 Tel: (0302) 662493 Fax: (0302) 675496 Dear Rt. Honourable Speaker, REPORT OF THE AUDITOR GENERAL ON THE ACCOUNTS OF DISTRICT ASSEMBLIES FOR THE FINANCIAL YEAR ENDED 31 DECEMBER 2019 I have the honour, in accordance with Article 187(5) of the Constitution to present my Report on the audit of the accounts of District Assemblies for the financial year ended 31 December 2019, to be laid before Parliament. 2. The Report is a consolidation of the significant findings and recommendations made during our routine audits, which have been formally communicated in management letters and annual audit reports to the Assemblies. -

Ghana FY20 Act West Work Plan Narrative Clean Web.Pdf
FY20 ACT TO END NTDs |WEST GHANA WORK PLAN Ghana FY 2020 Act to End Neglected Tropical Diseases | West Annual Work Plan October 1, 2019 – September 30, 2020 1 FY20 ACT TO END NTDs |WEST GHANA WORK PLAN II. TABLE OF CONTENTS I. COVER PAGE………………………………………………………………………………………………………….………………… 1 II. TABLE OF CONTENTS…………………………………………………………………………….……………..……….…………. 2 III. ACRONYM LIST………………………………………………………………………………………….………..….……………….. 3 NARRATIVE……………………………………………………………………………………………..……….………….………….. 5 1. National NTD PROGRAM OVERVIEW…………………………………………….…………………………….. 5 2. IR1 PLANNED ACTIVITIES: LF, TRA, OV……………………………………………………….…………….….. 6 3. SUSTAINABILITY STRATEGY ACTIVITIES (IR2 and IR3) …………………………………….…………... 13 i. DATA SECURITY AND MANAGEMENT……………………………………………….……………. 13 ii. DRUG MANAGEMENT………………………………………………………………………………….… 14 iii. MAINSTREAMING AND HSS ACTIVITIES (IR2) ………………………………………………... 15 iv. PLANNED ACTIVITIES: SCH, STH, POST VALIDATION/VERIFICATION SURVEILLANCE (IR3) ……………………………………………………………………………………... 16 2 FY20 ACT TO END NTDs |WEST GHANA WORK PLAN III. ACRONYM LIST AE-f-MDA Adverse Events following MDA ALB Albendazole APOC African Program for Oncho Control BCC Behaviour Change Communication CDC The United States Centers for Disease Prevention and Control CDD Community Drug Distributor CDTI Community directed treatment with ivermectin CMS Central Medical Stores CNTD Centre for Neglected Tropical Diseases DHMT District Health Management Team DSA Disease Specific Assessment FAA Fixed Agreement Award GES Ghana Education Service GHS Ghana Health -

PROMISE Baseline Survey
PROMISE Baseline Survey Garu-Tempane and East Mamprusi Districts 1 J. Bruce, R. Annan and M. Kumah PROMISE BASE LINE SURVEY J. Bruce1, R. Annan2 and M. Kumah3 . ACKNOWLEDGEMENTS We would first like to thank the management of CARE Ghana for the opportunity to undertake this study. We would also like to thank the managers and staff of PAS-Garu and PARED for their assistance with data collection especially when notice given was so short. We would also like to thank the translators who accompanied us in this process to the end. Thanks are due the District Directors of Agriculture as well as the District Nutrition Officers of the Garu=Tempane and East Mamprusi Districts for all time spent and information given during the data collection period. Finally, we would like to thank the community members who endured the long hours of interviewing without complaint. 1 P.O. Box KS 7025, Kumasi 2 Department of Biochemistry and Biotechnology, KNUST, Kumasi 3 The DORCAS Foundation, Tamale 2 TABLE OF CONTENTS PAGE 1.0 BACKGROUND TO THE STUDY 5 1.1 Methodology 5 1.2 The Report 7 2.0 FINDINGS OF THE STUDY 9 2.1 Project Intermediate Outcome 1 9 2.2 Project Intermediate Outcome 2 26 2.3 Project Intermediate Outcome 3 35 3.0 CHALLENGES AND RECOMMENDATION 40 APPENDICES 42 3 4 Acronyms AC Area Council CAPS Community Action Plans CBEA Community Based Extension Systems CIDA Canadian International Development Agency CSIR Council for Scientific and Industrial Research DA District Assembly DMTDP District Medium Term Development Plan FBO Farmer Based Organization GHS -
GARU DISTRICT ASSEMBLY SUB-PROGRAMME: SP 1.2: Finance and Revenue Mobilization
Table of Contents PART A: INTRODUCTION ............................................................................................................................. 4 1. ESTABLISHMENT OF THE DISTRICT ........................................................................................ 4 2. POPULATION STRUCTURE ........................................................................................................... 4 3. DISTRICT ECONOMY ..................................................................................................................... 5 a. AGRICULTURE ............................................................................................................................. 5 b. MARKET CENTRE ....................................................................................................................... 6 c. ROAD NETWORK ......................................................................................................................... 6 d. EDUCATION ................................................................................................................................... 6 e. HEALTH .......................................................................................................................................... 7 f. WATER AND SANITATION ........................................................................................................ 8 g. BUILT ENVIRONMENT ............................................................................................................... 9 REPUBLIC -

Upper East Region
UPPER EAST REGION AGRICULTURAL CLASS NO NAME CURRENT GRADE RCC/MMDA QUALIFICATION INSTITUTION REMARKS ATTENDED Animal Production Bawku West District Upgrading 1 Mahama Bukari Officer Assembly BSc. Agriculture University of Energy Nabdam District University of Energy Upgrading 2 Zenaze Issah Chief Technical Officer Assembly BSc. Agriculture and Natural Resources Senior Production Bongo District Upgrading 3 Aforuk Dominic Officer Assembly B.Ed. Agriculture Science UDS Senior Technician Pusiga District University of Energy Conversion 4 Yaw Jeyija Joshua Engineer Assembly BSc. Agriculture and Natural Resources Bongo District University of Cape Upgrading 5 Tipien-Kaarayir Anane Senior Technical Officer Assembly BSc. Agriculture Extension Coast ENGINEERING CLASS NO NAME CURRENT GRADE RCC/MMDA QUALIFICATION INSTITUTION REMARKS ATTENDED Garu District Sunyani Techni. Conversion 1 Issaka Karim Ayabugri Revenue Inspector Assembly Btech. Building Technology University Botchway Kwame Principal Technician Binduri District Sunyani Technical Upgrading 2 Emmanuel Engineer Assembly Btech. Building Technology University Principal Technician Bawku West Distant Sunyani Technical Upgrading 3 Dominic Kwasi Alandu Engineer Assembly Btech. Building Technology University Akologo Azoogo Senior Technician Tempane District Sunyani Technical Upgrading 4 Abednego Engineer Assembly Btech Building Technology University Principal Technician Bawku West District Sunyani Technical Upgrading 5 Dominic Kwasi Engineer Assembly Btech. Building Technology University Akologo Azoogo