Efficacy of Amrubicin for Non-Small Cell Lung Cancer After Failure of Two Or More Prior Chemotherapy Regimens
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Metabolic Carbonyl Reduction of Anthracyclines — Role in Cardiotoxicity and Cancer Resistance
Invest New Drugs DOI 10.1007/s10637-017-0443-2 REVIEW Metabolic carbonyl reduction of anthracyclines — role in cardiotoxicity and cancer resistance. Reducing enzymes as putative targets for novel cardioprotective and chemosensitizing agents Kamil Piska1 & Paulina Koczurkiewicz1 & Adam Bucki 2 & Katarzyna Wójcik-Pszczoła1 & Marcin Kołaczkowski2 & Elżbieta Pękala1 Received: 23 November 2016 /Accepted: 17 February 2017 # The Author(s) 2017. This article is published with open access at Springerlink.com Summary Anthracycline antibiotics (ANT), such as doxoru- monoHER, curcumin, (−)-epigallocatechin gallate, resvera- bicin or daunorubicin, are a class of anticancer drugs that are trol, berberine or pixantrone, and their modulating effect on widely used in oncology. Although highly effective in cancer the activity of ANT is characterized and discussed as potential therapy, their usefulness is greatly limited by their mechanism of action for novel therapeutics in cancer cardiotoxicity. Possible mechanisms of ANT cardiotoxicity treatment. include their conversion to secondary alcohol metabolites (i.e. doxorubicinol, daunorubicinol) catalyzed by carbonyl re- Keywords Anthracyclines . Cardiotoxicity . Resistance . ductases (CBR) and aldo-keto reductases (AKR). These me- Pharmacokinetics . Drug metabolism . Anticancer agents tabolites are suspected to be more cardiotoxic than their parent compounds. Moreover, overexpression of ANT-reducing en- zymes (CBR and AKR) are found in many ANT-resistant Introduction cancers. The secondary metabolites show decreased cytotoxic properties and are more susceptible to ABC-mediated efflux Anthracyclines (ANT) are a class of cell-cycle non-specific than their parent compounds; thus, metabolite formation is anticancer antibiotics that were first isolated from the considered one of the mechanisms of cancer resistance. Streptomyces genus in the early 1960s. -

Management of Lung Cancer-Associated Malignant Pericardial Effusion with Intrapericardial Administration of Carboplatin: a Retrospective Study
Management of Lung Cancer-Associated Malignant Pericardial Effusion With Intrapericardial Administration of Carboplatin: A Retrospective Study Hisao Imai ( [email protected] ) Gunma Prefectural Cancer Center Kyoichi Kaira Comprehensive Cancer Center, International Medical Center, Saitama Medical University Ken Masubuchi Gunma Prefectural Cancer Center Koichi Minato Gunma Prefectural Cancer Center Research Article Keywords: Acute pericarditis, Catheter drainage, Intrapericardial carboplatin, Lung cancer, Malignant pericardial effusion Posted Date: May 28th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-558833/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/8 Abstract Purpose: It has been reported that 5.1-7.0% of acute pericarditis is carcinomatous pericarditis. Malignant pericardial effusion (MPE) can progress to cardiac tamponade, which is a life-threatening condition. The effectiveness and feasibility of intrapericardial instillation of carboplatin (CBDCA; 150 mg/body) have never been evaluated in patients with lung cancer, which is the most common cause of MPE. Therefore, we evaluated the effectiveness and feasibility of intrapericardial administration of CBDCA following catheter drainage in patients with lung cancer-associated MPE. Methods: In this retrospective study, 21 patients with symptomatic lung cancer-associated MPE, who were administered intrapericardial CBDCA (150 mg/body) at Gunma Prefectural Cancer Center between January 2005 and March 2018, were included. The patients’ characteristics, response to treatment, and toxicity incidence were evaluated. Results: Thirty days after the intrapericardial administration of CBDCA, MPE was controlled in 66.7% of the cases. The median survival period from the day of administration until death or last follow-up was 71 days (range: 10–2435 days). -

Pharmaceutical Appendix to the Tariff Schedule 2
Harmonized Tariff Schedule of the United States (2006) – Supplement 1 (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2006) – Supplement 1 (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABACAVIR 136470-78-5 ACEXAMIC ACID 57-08-9 ABAFUNGIN 129639-79-8 ACICLOVIR 59277-89-3 ABAMECTIN 65195-55-3 ACIFRAN 72420-38-3 ABANOQUIL 90402-40-7 ACIPIMOX 51037-30-0 ABARELIX 183552-38-7 ACITAZANOLAST 114607-46-4 ABCIXIMAB 143653-53-6 ACITEMATE 101197-99-3 ABECARNIL 111841-85-1 ACITRETIN 55079-83-9 ABIRATERONE 154229-19-3 ACIVICIN 42228-92-2 ABITESARTAN 137882-98-5 ACLANTATE 39633-62-0 ABLUKAST 96566-25-5 ACLARUBICIN 57576-44-0 ABUNIDAZOLE 91017-58-2 ACLATONIUM NAPADISILATE 55077-30-0 ACADESINE 2627-69-2 ACODAZOLE 79152-85-5 ACAMPROSATE 77337-76-9 ACONIAZIDE 13410-86-1 ACAPRAZINE 55485-20-6 ACOXATRINE 748-44-7 ACARBOSE 56180-94-0 ACREOZAST 123548-56-1 ACEBROCHOL 514-50-1 ACRIDOREX 47487-22-9 ACEBURIC -

A Phase I/II Trial of Belinostat in Combination with Cisplatin, Doxorubicin, and Cyclophosphamide in Thymic Epithelial Tumors: a Clinical and Translational Study
Published OnlineFirst September 4, 2014; DOI: 10.1158/1078-0432.CCR-14-0968 Clinical Cancer Cancer Therapy: Clinical Research A Phase I/II Trial of Belinostat in Combination with Cisplatin, Doxorubicin, and Cyclophosphamide in Thymic Epithelial Tumors: A Clinical and Translational Study Anish Thomas1, Arun Rajan1, Eva Szabo2, Yusuke Tomita1, Corey A. Carter3, Barbara Scepura1, Ariel Lopez-Chavez1, Min-Jung Lee1, Christophe E. Redon4, Ari Frosch1, Cody J. Peer1, Yuanbin Chen1, Richard Piekarz5, Seth M. Steinberg6, Jane B. Trepel1, William D. Figg1, David S. Schrump7, and Giuseppe Giaccone1 Abstract Purpose: This phase I/II study sought to determine the safety and maximum tolerated dose (MTD) of a novel schedule of belinostat, a histone deacetylase inhibitor (HDAC) administered before and in combi- nation with cisplatin (P), doxorubicin (A), and cyclophosphamide (C) in thymic epithelial tumors (TET). Antitumor activity, pharmacokinetics, and biomarkers of response were also assessed. Experimental Design: Patients with advanced, unresectable TET received increasing doses of belinostat as a continuous intravenous infusion over 48 hours with chemotherapy in 3-week cycles. In phase II, belinostat at the MTD was used. Results: Twenty-six patients were enrolled (thymoma, 12; thymic carcinoma, 14). Dose-limiting toxicities at 2,000 mg/m2 belinostat were grade 3 nausea and diarrhea and grade 4 neutropenia and thrombocytopenia, respectively, in two patients. Twenty-four patients were treated at the MTD of 1,000 mg/m2 with chemo- therapy (P, 50 mg/m2 on day 2; A, 25 mg/m2 on days 2 and 3; C, 500 mg/m2 on day 3). Objective response rates in thymoma and thymic carcinoma were 64% (95% confidence interval, 30.8%-89.1%) and 21% (4.7%–50.8%), respectively. -

Comparative Transcriptome Analysis Reveals Key Epigenetic Targets in SARS-Cov-2 Infection
www.nature.com/npjsba ARTICLE OPEN Comparative transcriptome analysis reveals key epigenetic targets in SARS-CoV-2 infection Marisol Salgado-Albarrán 1,2,7, Erick I. Navarro-Delgado 3,7, Aylin Del Moral-Morales 1,7, Nicolas Alcaraz 4, Jan Baumbach 5,6, ✉ ✉ Rodrigo González-Barrios3 and Ernesto Soto-Reyes 1 COVID-19 is an infection caused by SARS-CoV-2 (Severe Acute Respiratory Syndrome coronavirus 2), which has caused a global outbreak. Current research efforts are focused on the understanding of the molecular mechanisms involved in SARS-CoV-2 infection in order to propose drug-based therapeutic options. Transcriptional changes due to epigenetic regulation are key host cell responses to viral infection and have been studied in SARS-CoV and MERS-CoV; however, such changes are not fully described for SARS-CoV-2. In this study, we analyzed multiple transcriptomes obtained from cell lines infected with MERS-CoV, SARS-CoV, and SARS-CoV-2, and from COVID-19 patient-derived samples. Using integrative analyses of gene co-expression networks and de-novo pathway enrichment, we characterize different gene modules and protein pathways enriched with Transcription Factors or Epifactors relevant for SARS-CoV-2 infection. We identified EP300, MOV10, RELA, and TRIM25 as top candidates, and more than 60 additional proteins involved in the epigenetic response during viral infection that has therapeutic potential. Our results show that targeting the epigenetic machinery could be a feasible alternative to treat COVID-19. npj Systems Biology and Applications (2021) 7:21 ; https://doi.org/10.1038/s41540-021-00181-x 1234567890():,; INTRODUCTION hallmark of active chromatin)10, histone acetylation in H3 and The coronavirus family (CoV) are non-segmented, positive-sense, H4 histones, and increased levels of H4K20me2 and unmodified 11 and enveloped RNA viruses that have been identified as the cause H3K36 and H4K79 have been reported . -

Review Article
REVIEW ARTICLE Chemotherapy advances in small-cell lung cancer Bryan A. Chan1,2, Jermaine I. G. Coward1,2,3 1Mater Adult Hospital, Department of Medical Oncology, Raymond Terrace, Brisbane, QLD 4101, Australia; 2School of Medicine, University of Queensland, St Lucia, Brisbane, QLD 4072, Australia; 3Inflammation & Cancer Therapeutics Group, Mater Research, Level 4, Translational Research Institute, Woolloongabba, Brisbane, QLD 4102, Australia ABSTRACT Although chemotherapeutic advances have recently been heralded in lung adenocarcinomas, such success with small-cell lung cancer (SCLC) has been ominously absent. Indeed, the dismal outlook of this disease is exemplified by the failure of any significant advances in first line therapy since the introduction of the current standard platinum-etoposide doublet over 30 years ago. Moreover, such sluggish progress is compounded by the dearth of FDA-approved agents for patients with relapsed disease. However, over the past decade, novel formulations of drug classes commonly used in SCLC (e.g. topoisomerase inhibitors, anthracyclines, alkylating and platinum agents) are emerging as potential alternatives that could effectively add to the armamentarium of agents currently at our disposal. This review is introduced with an overview on the historical development of chemotherapeutic regimens used in this disease and followed by the recent encouraging advances witnessed in clinical trials with drugs such as amrubicin and belotecan which are forging new horizons for future treatment algorithms. KEY WORDS Small cell lung cancer (SCLC); amrubicin; belotecan; picoplatin; relapsed SCLC J Thorac Dis 2013;5(S5):S565-S578. doi: 10.3978/j.issn.2072-1439.2013.07.43 Introduction cigarette smoking 20 years prior, but is now slowly decreasing due to changing smoking patterns (2). -
Cancer Cell Targeting Using Nanoparticles
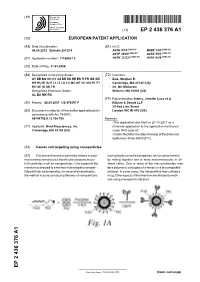
(19) & (11) EP 2 436 376 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 04.04.2012 Bulletin 2012/14 A61K 9/14 (2006.01) B82B 1/00 (2006.01) A61P 35/00 (2006.01) A61K 9/51 (2006.01) (2006.01) (2006.01) (21) Application number: 11186037.5 A61K 31/337 A61K 9/48 (22) Date of filing: 31.03.2008 (84) Designated Contracting States: (72) Inventors: AT BE BG CH CY CZ DE DK EE ES FI FR GB GR • Zale, Stephen E. HR HU IE IS IT LI LT LU LV MC MT NL NO PL PT Cambridge, MA 02142 (US) RO SE SI SK TR • Ali, Mir Mikkaram Designated Extension States: Woburn, MA 01801 (US) AL BA MK RS (74) Representative: Harris, Jennifer Lucy et al (30) Priority: 28.09.2007 US 976197 P Kilburn & Strode LLP 20 Red Lion Street (62) Document number(s) of the earlier application(s) in London WC1R 4PJ (GB) accordance with Art. 76 EPC: 08744752.0 / 2 136 788 Remarks: •This application was filed on 20-10-2011 as a (71) Applicant: Bind Biosciences, Inc. divisional application to the application mentioned Cambridge, MA 02139 (US) under INID code 62. •Claims filed after the date of receipt of the divisional application (Rule 68(4) EPC). (54) Cancer cell targeting using nanoparticles (57) The present invention generally relates to poly- having highly controlled properties, which can be formed mersand macromolecules, inparticular, to polymersuse- by mixing together two or more macromolecules in dif- ful in particles such as nanoparticles. -

Successful Treatment of a Patient with Synchronous Advanced Non-Small
ANTICANCER RESEARCH 25: 2579-2582 (2005) Successful Treatment of a Patient with Synchronous Advanced Non-small Cell Lung Cancer and Acute Myeloid Leukemia by a Combination of Gefitinib, Low-dose Cytarabine and Aclarubicin NAGIO TAKIGAWA1, MAKOTO TAKEUCHI2, TAKUO SHIBAYAMA1, ISAO YOSHIDA2, NORIKO KAWATA1, ATSUHIKO TADA1, HIROSHI UEOKA4 and KIYOSHI TAKAHASHI3 1Department of Pulmonary Medicine, 2Department of Hematology and 3Department of Internal Medicine, National Hospital Organization, Minami-Okayama Medical Center, 4066 Hayashima, Okayama 701-0304; 4Department of Hematology, Oncology and Respiratory Medicine, Okayama University Graduate School of Medicine and Dentistry, 2-5-1 Shikata, Okayama 700-8558, Japan Abstract. There are few reports describing simultaneous not yet been established. Gefitinib, the tyrosine kinase occurrence of acute leukemia and lung cancer. We describe inhibitor of epidermal growth factor receptor, has anti- here an 83-year-old woman who simultaneously developed tumor activity in advanced NSCLC (5, 6), and was effective advanced adenocarcinoma of the lung and acute myeloid even in elderly patients with poor PS (7, 8). On the other leukemia. She could not receive intensive chemotherapy due to hand, for elderly patients with acute myeloid leukemia poor performance status. This patient was treated with a (AML), conventional combinations of anthracycline combination of gefitinib, low-dose cytarabine and aclarubicin. (daunorubicin or idarubicin) and cytarabine have frequently This combination could be safely administered in the elderly been used (9), however, the standard treatment for patients patient with poor performance status and was effective for both aged 75 years or older has not been established (10). In lung cancer and acute myeloid leukemia. Japan, a combination of low-dose cytarabine and aclarubicin was reported to be useful in previously untreated elderly (65 The incidence of lung cancer is increasing worldwide and - 82 years old) patients with AML (11). -

Imatinib Mesylate
217-222.qxd 17/11/2009 08:35 Ì Page 217 ONCOLOGY REPORTS 23: 217-222, 2010 217 Imatinib mesylate (STI571) enhances amrubicin-induced cytotoxic activity through inhibition of the phosphatidylinositol 3-kinase/Akt pathway in small cell lung cancer cells HISASHI SUYAMA, TADASHI IGISHI, YASUTO UEDA, YASUSHI SHIGEOKA, MASAHIRO KODANI, MASATO MORITA, KENICHI TAKEDA, TAKASHI SUMIKAWA, HIROFUMI NAKAZAKI, KEIJI MATSUNAMI, SHINGO MATSUMOTO and EIJI SHIMIZU Division of Medical Oncology and Molecular Respirology, Faculty of Medicine, Tottori University, Yonago 683-8504, Japan Received July 30, 2009; Accepted September 17, 2009 DOI: 10.3892/or_00000626 Abstract. Small cell lung cancer (SCLC) is characterized by Introduction autocrine mechanisms. Stem cell factor (SCF) and its receptor c-kit can activate Akt and extracellular signal-regulated kinase Small cell lung cancer (SCLC) is a highly aggressive neoplasm (Erk) pathways. Imatinib mesylate (STI571) can inhibit c-kit characterized by a high growth fraction, short doubling time tyrosine kinase activity, but clinical trials have resulted in and high rate of metastasis (1), but is sensitive to chemotherapy failure. We investigated the possibility of SCF/c-kit-targeted (2). Systemic chemotherapy prolongs the survival of SCLC therapy against SCLC. Using c-kit-positive SCLC cells patients (3), and cisplatin (CDDP), etoposide (VP-16), topoiso- (H209 and H69 cells) and SCF as a model of the autocrine merase I inhibitors [irinotecan (CPT-11) and topotecan] (4,5) mechanisms, the effects of SCF, LY294002, PD98059 or and amrubicin (AMR) (6) (a totally synthetic 9-amino- STI571 on Akt and Erk were assessed by Western blot anthracycline) are used in regular clinical practice in Japan. -

Systematic Analysis of the Transcriptome Profiles and Co-Expression Networks of Tumour Endothelial Cells Identifies Several Tumo
cancers Article Systematic Analysis of the Transcriptome Profiles and Co-Expression Networks of Tumour Endothelial Cells Identifies Several Tumour-Associated Modules and Potential Therapeutic Targets in Hepatocellular Carcinoma Thomas Mohr 1,2 , Sonja Katz 1 , Verena Paulitschke 3 , Nadim Aizarani 4 and Alexander Tolios 5,6,7,∗ 1 ScienceConsult—DI Thomas Mohr KG, Enzianweg 10a, A-2353 Guntramsdorf, Austria; [email protected] or [email protected] (T.M.); [email protected] (S.K.) 2 Institute of Cancer Research, Department of Medicine I, Medical University of Vienna and Comprehensive Cancer Center, A-1090 Vienna, Austria 3 Department of Dermatology, Medical University of Vienna, A-1090 Vienna, Austria; [email protected] 4 Max-Planck-Institute of Immunobiology and Epigenetics, D-79108 Freiburg, Germany; [email protected] 5 Department of Blood Group Serology and Transfusion Medicine, Medical University of Vienna, A-1090 Vienna, Austria 6 Center of Physiology and Pharmacology, Institute of Vascular Biology and Thrombosis Research, Medical University of Vienna, A-1090 Vienna, Austria 7 Section of Artificial Intelligence and Decision Support, Center for Medical Statistics, Informatics and Citation: Mohr, T.; Katz, S.; Intelligent Systems, Medical University of Vienna, A-1090 Vienna, Austria Paulitschke, V.; Aizarani, N.; Tolios, * Correspondence: [email protected] A. Systematic Analysis of the Transcriptome Profiles and Simple Summary: Endothelial cells, the innermost layer of blood vessels, play an essential role in the Co-Expression Networks of Tumour progression of cancer, particularly liver cancer. To develop cancer therapies targeting those cells, the Endothelial Cells Identifies Several investigation of gene co-expression networks is of great importance. -

Systemic Therapy for Limited Stage Small Cell Lung Carcinoma
6290 Review Article on Small Cell Lung Cancer Systemic therapy for limited stage small cell lung carcinoma Vanita Noronha, Anbarasan Sekhar, Vijay Maruti Patil, Nandini Menon, Amit Joshi, Akhil Kapoor, Kumar Prabhash Department of Medical Oncology, Tata Memorial Hospital, Parel, Mumbai; Homi Bhabha National Institute, Mumbai, India Contributions: (I) Conception and design: V Noronha, A Sekhar; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: V Noronha, A Sekhar; (V) Data analysis and interpretation: V Noronha, A Sekhar; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Kumar Prabhash. Professor, Department of Medical Oncology, Tata Memorial Hospital, Parel, Mumbai, India; Homi Bhabha National Institute, Mumbai, India. Email: [email protected]. Abstract: Systemic treatment in small cell lung carcinoma has been a challenge for oncologists for decades. The high propensity for recurrence is usually due to distant metastasis, which makes systemic treatment an essential component of treatment in small cell lung carcinoma. The regimen of cisplatin and etoposide (established in the mid-1980’s) concurrently with thoracic radiotherapy followed by prophylactic cranial irradiation (PCI) remains the standard of care in limited stage disease. Despite numerous trials, this regimen has not been improved upon. The standard combination regimen of cisplatin and etoposide has been compared to alternative platinum-containing regimens with drugs like epirubicin, irinotecan, paclitaxel, topotecan, pemetrexed, amrubicin and belotecan. Non-platinum containing regimens like ifosfamide and etoposide have also been tested. Attempts to intensify therapy have included the addition of a third drug like paclitaxel, ifosfamide, tirapazamine, tamoxifen, and thalidomide. -

Pharmaceuticals Appendix
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE