Successful Treatment of a Patient with Synchronous Advanced Non-Small
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Transcatheter Arterial Chemoembolization Therapy for Hepatocellular Carcinoma Using Polylactic Acid Microspheres Containing Acla
[CANCER RESEARCH 49. 4357-4362, August 1. 1989] Transcatheter Arterial Chemoembolization Therapy for Hepatocellular Carcinoma Using Polylactic Acid Microspheres Containing Aclarubicin Hydrochloride 1omonimi Ichihara,1 Kiyoshi Sakamoto, Katsutaka Mori, and Masanobu Akagi Department of Surgery II, Kumamoto University Medical School, Kumamoto 860, Japan 4BSTRACT MATERIALS AND METHODS Transcatheter arterial Chemoembolization therapy using polylactic Preparation of PLA-ACRms acid microspheres containing aclarubicin hydrochloride (ACR) was per PLA-ACRms were prepared in the pharmacy of the Kumamoto formed in 62 patients with primary hepatocellular carcinoma. These microspheres were about 200 ¡anin diameter and contained 10% (w/w) University Hospital. Briefly, aclarubicin hydrochloride and isopropyl aclarubicin. A single dose of polylactic acid microspheres containing ACR myristate, a medium-chain fatty acid ester, were dissolved in 7.5% (50-100 mg of ACR) was administered 1 to 8 times with a mean of 2.2 polylactic acid-methylene chloride. The resultant solution was dispersed in 1% gelatin solution and sterilized in an autoclave for 20 min at doses (a total of 160 treatments) in 62 patients. Antitumor effects were 120°C;thismixture was then stirred with a magnetic stirrer at 500 rpm observed from the decrease in serum a-fetoprotein levels (82.1% of the patients) and in two dimensional size of tumor on computed tomography for 1 h. The resultant microspheres were collected by filtration through (93.6%). The cumulative survival rate was 54.3% at 1 year, 24.6% at 2 a membrane filter (3 //m pore diameter), rinsed 2 to 3 times (in 1 liter years, and 19.2% at 3 years, respectively, among 59 patients with of distilled water), and dried under reduced pressure for 5 days. -

Phenotype Microarrays Panels PM-M1 to PM-M14
Phenotype MicroArrays™ Panels PM-M1 to PM-M14 for Phenotypic Characterization of Mammalian Cells Assays: Energy Metabolism Pathways Ion and Hormone Effects on Cells Sensitivity to Anti-Cancer Agents and for Optimizing Culture Conditions for Mammalian Cells PRODUCT DESCRIPTIONS AND INSTRUCTIONS FOR USE PM-M1 Cat. #13101 PM-M2 Cat. #13102 PM-M3 Cat. #13103 PM-M4 Cat. #13104 PM-M5 Cat. #13105 PM-M6 Cat. #13106 PM-M7 Cat. #13107 PM-M8 Cat. #13108 PM-M11 Cat. #13111 PM-M12 Cat. #13112 PM-M13 Cat. #13113 PM-M14 Cat. #13114 © 2016 Biolog, Inc. All rights reserved Printed in the United States of America 00P 134 Rev F February 2020 - 1 - CONTENTS I. Introduction ...................................................................................................... 2 a. Overview ................................................................................................... 2 b. Background ............................................................................................... 2 c. Uses ........................................................................................................... 2 d. Advantages ................................................................................................ 3 II. Product Description, PM-M1 to M4 ................................................................ 3 III. Protocols, PM-M1 to M4 ................................................................................. 7 a. Materials Required .................................................................................... 7 b. Determination -

Towards the Reduction of Occupational Exposure To
TOWARDS THE REDUCTION OF OCCUPATIONAL EXPOSURE TO CYTOTOXIC DRUGS by Cristian Vasile Barzan B.Sc. Simon Fraser University, 2007 A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIRMENTS FOR THE DEGREE OF MASTER OF SCIENCE in The Faculty of Graduate Studies (Occupational and Environmental Hygiene) THE UNIVERSITY OF BRITISH COLUMBIA (Vancouver) October 2010 © Cristian Vasile Barzan, 2010 Abstract Background : One of the most powerful and widely used techniques in cancer treatment is the use of cytotoxic drugs in chemotherapy. These drugs are inherently hazardous with many of them causing carcinogenic, mutagenic or teratogenic health outcomes. Occupational exposure to cytotoxic drugs is of great concern due to their lack of selectivity between healthy and unhealthy cells. Widespread cytotoxic drug contamination has been reported in North America, Europe and Australia. Current cleaning protocols for hazardous antineoplastic drugs include the use of disinfectants and oxidizing agents, such as household bleach. Aim : The thesis project focused on two objectives: 1) hypothesize and confirm potential hazardous by- products arising from cleaning cyclophosphamide, a widely used cytotoxic drugs, with household bleach, a commonly used cleaning agent; 2) develop an effective and safe cleaning agent for cytotoxic drugs in order to prevent and eliminate exposure to these drugs. Methods : The gas chromatograph mass spectrum (GC/MS) was used to analyze the decomposition of cyclophosphamide by household bleach (5.25% hypochlorite). The reaction was conducted in a test-tube and the by-products extracted and derivatized prior to analysis. Multiple cleaning agent compositions were tested on 10x10cm stainless steel plates spiked with the two model cytotoxic drugs, cyclophosphamide and methotrexate. -

Functional Similarity of Anticancer Drugs by MTT Bioassay
cer Scien an ce C & f o T l h a e Hiwasa et al., J Cancer Sci Ther 2011, 3.10 n r a Journal of r p u 1000099 y o J DOI: 10.4172/1948-5956. ISSN: 1948-5956 Cancer Science & Therapy Rapid Communication Open Access Functional Similarity of Anticancer Drugs by MTT Bioassay Takaki Hiwasa1*,Takanobu Utsumi1, Mari Yasuraoka1, Nana Hanamura1, Hideaki Shimada2, Hiroshi Nakajima3, Motoo Kitagawa4, Yasuo Iwadate4,5, Ken-ichiro Goto6, Atsushi Takeda7, Kenzo Ohtsuka8, Hiroyoshi Ariga9 and Masaki Takiguchi1 1Department of Biochemistry, and Genetics, Chiba University, Graduate School of Medicine, Chuo-ku, Chiba 260-8670, Japan 2Department of Surgery, School of Medicine, Toho University, Ota-ku, Tokyo 143-8541, Japan 3Department of Molecular Genetics, Chiba University, Graduate School of Medicine, Chuo-ku, Chiba 260-8670, Japan 4Department of Molecular and Tumor Pathology, Chiba University, Graduate School of Medicine, Chuo-ku, Chiba 260-8670, Japan 5Department of Neurological Surgery, Chiba University, Graduate School of Medicine, Chuo-ku, Chiba 260-8670, Japan 6Department of Orthopaedic Surgery, National Hospital Organization, Shimoshizu Hospital, Yotsukaido, Chiba 284-0003, Japan 7Laboratory of Biochemistry, Graduate School of Nutritional Sciences, Sagami Women’s University, Sagamihara, Kanagawa 252-0383, Japan 8Laboratory of Cell & Stress Biology, Department of Environmental Biology, Chubu University, Matsumoto-cho, Kasugai, Aichi 487-8501, Japan 9Graduate School of Pharmaceutical Sciences, Hokkaido University, Kita-ku, Sapporo 060-0812, Japan Abstract We prepared normal or Ha-ras-transformed NIH3T3 cells transfected stably or transiently with various tumor- related genes. The chemosensitivity of the transfected clones to 16 anticancer drugs was compared to the parental control cells using the MTT assay. -

Metabolic Carbonyl Reduction of Anthracyclines — Role in Cardiotoxicity and Cancer Resistance
Invest New Drugs DOI 10.1007/s10637-017-0443-2 REVIEW Metabolic carbonyl reduction of anthracyclines — role in cardiotoxicity and cancer resistance. Reducing enzymes as putative targets for novel cardioprotective and chemosensitizing agents Kamil Piska1 & Paulina Koczurkiewicz1 & Adam Bucki 2 & Katarzyna Wójcik-Pszczoła1 & Marcin Kołaczkowski2 & Elżbieta Pękala1 Received: 23 November 2016 /Accepted: 17 February 2017 # The Author(s) 2017. This article is published with open access at Springerlink.com Summary Anthracycline antibiotics (ANT), such as doxoru- monoHER, curcumin, (−)-epigallocatechin gallate, resvera- bicin or daunorubicin, are a class of anticancer drugs that are trol, berberine or pixantrone, and their modulating effect on widely used in oncology. Although highly effective in cancer the activity of ANT is characterized and discussed as potential therapy, their usefulness is greatly limited by their mechanism of action for novel therapeutics in cancer cardiotoxicity. Possible mechanisms of ANT cardiotoxicity treatment. include their conversion to secondary alcohol metabolites (i.e. doxorubicinol, daunorubicinol) catalyzed by carbonyl re- Keywords Anthracyclines . Cardiotoxicity . Resistance . ductases (CBR) and aldo-keto reductases (AKR). These me- Pharmacokinetics . Drug metabolism . Anticancer agents tabolites are suspected to be more cardiotoxic than their parent compounds. Moreover, overexpression of ANT-reducing en- zymes (CBR and AKR) are found in many ANT-resistant Introduction cancers. The secondary metabolites show decreased cytotoxic properties and are more susceptible to ABC-mediated efflux Anthracyclines (ANT) are a class of cell-cycle non-specific than their parent compounds; thus, metabolite formation is anticancer antibiotics that were first isolated from the considered one of the mechanisms of cancer resistance. Streptomyces genus in the early 1960s. -

Management of Lung Cancer-Associated Malignant Pericardial Effusion with Intrapericardial Administration of Carboplatin: a Retrospective Study
Management of Lung Cancer-Associated Malignant Pericardial Effusion With Intrapericardial Administration of Carboplatin: A Retrospective Study Hisao Imai ( [email protected] ) Gunma Prefectural Cancer Center Kyoichi Kaira Comprehensive Cancer Center, International Medical Center, Saitama Medical University Ken Masubuchi Gunma Prefectural Cancer Center Koichi Minato Gunma Prefectural Cancer Center Research Article Keywords: Acute pericarditis, Catheter drainage, Intrapericardial carboplatin, Lung cancer, Malignant pericardial effusion Posted Date: May 28th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-558833/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/8 Abstract Purpose: It has been reported that 5.1-7.0% of acute pericarditis is carcinomatous pericarditis. Malignant pericardial effusion (MPE) can progress to cardiac tamponade, which is a life-threatening condition. The effectiveness and feasibility of intrapericardial instillation of carboplatin (CBDCA; 150 mg/body) have never been evaluated in patients with lung cancer, which is the most common cause of MPE. Therefore, we evaluated the effectiveness and feasibility of intrapericardial administration of CBDCA following catheter drainage in patients with lung cancer-associated MPE. Methods: In this retrospective study, 21 patients with symptomatic lung cancer-associated MPE, who were administered intrapericardial CBDCA (150 mg/body) at Gunma Prefectural Cancer Center between January 2005 and March 2018, were included. The patients’ characteristics, response to treatment, and toxicity incidence were evaluated. Results: Thirty days after the intrapericardial administration of CBDCA, MPE was controlled in 66.7% of the cases. The median survival period from the day of administration until death or last follow-up was 71 days (range: 10–2435 days). -

Pharmaceutical Appendix to the Tariff Schedule 2
Harmonized Tariff Schedule of the United States (2006) – Supplement 1 (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2006) – Supplement 1 (Rev. 1) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABACAVIR 136470-78-5 ACEXAMIC ACID 57-08-9 ABAFUNGIN 129639-79-8 ACICLOVIR 59277-89-3 ABAMECTIN 65195-55-3 ACIFRAN 72420-38-3 ABANOQUIL 90402-40-7 ACIPIMOX 51037-30-0 ABARELIX 183552-38-7 ACITAZANOLAST 114607-46-4 ABCIXIMAB 143653-53-6 ACITEMATE 101197-99-3 ABECARNIL 111841-85-1 ACITRETIN 55079-83-9 ABIRATERONE 154229-19-3 ACIVICIN 42228-92-2 ABITESARTAN 137882-98-5 ACLANTATE 39633-62-0 ABLUKAST 96566-25-5 ACLARUBICIN 57576-44-0 ABUNIDAZOLE 91017-58-2 ACLATONIUM NAPADISILATE 55077-30-0 ACADESINE 2627-69-2 ACODAZOLE 79152-85-5 ACAMPROSATE 77337-76-9 ACONIAZIDE 13410-86-1 ACAPRAZINE 55485-20-6 ACOXATRINE 748-44-7 ACARBOSE 56180-94-0 ACREOZAST 123548-56-1 ACEBROCHOL 514-50-1 ACRIDOREX 47487-22-9 ACEBURIC -

A Phase I/II Trial of Belinostat in Combination with Cisplatin, Doxorubicin, and Cyclophosphamide in Thymic Epithelial Tumors: a Clinical and Translational Study
Published OnlineFirst September 4, 2014; DOI: 10.1158/1078-0432.CCR-14-0968 Clinical Cancer Cancer Therapy: Clinical Research A Phase I/II Trial of Belinostat in Combination with Cisplatin, Doxorubicin, and Cyclophosphamide in Thymic Epithelial Tumors: A Clinical and Translational Study Anish Thomas1, Arun Rajan1, Eva Szabo2, Yusuke Tomita1, Corey A. Carter3, Barbara Scepura1, Ariel Lopez-Chavez1, Min-Jung Lee1, Christophe E. Redon4, Ari Frosch1, Cody J. Peer1, Yuanbin Chen1, Richard Piekarz5, Seth M. Steinberg6, Jane B. Trepel1, William D. Figg1, David S. Schrump7, and Giuseppe Giaccone1 Abstract Purpose: This phase I/II study sought to determine the safety and maximum tolerated dose (MTD) of a novel schedule of belinostat, a histone deacetylase inhibitor (HDAC) administered before and in combi- nation with cisplatin (P), doxorubicin (A), and cyclophosphamide (C) in thymic epithelial tumors (TET). Antitumor activity, pharmacokinetics, and biomarkers of response were also assessed. Experimental Design: Patients with advanced, unresectable TET received increasing doses of belinostat as a continuous intravenous infusion over 48 hours with chemotherapy in 3-week cycles. In phase II, belinostat at the MTD was used. Results: Twenty-six patients were enrolled (thymoma, 12; thymic carcinoma, 14). Dose-limiting toxicities at 2,000 mg/m2 belinostat were grade 3 nausea and diarrhea and grade 4 neutropenia and thrombocytopenia, respectively, in two patients. Twenty-four patients were treated at the MTD of 1,000 mg/m2 with chemo- therapy (P, 50 mg/m2 on day 2; A, 25 mg/m2 on days 2 and 3; C, 500 mg/m2 on day 3). Objective response rates in thymoma and thymic carcinoma were 64% (95% confidence interval, 30.8%-89.1%) and 21% (4.7%–50.8%), respectively. -

In Vitro Synergistic Effects of Anthracycline Antitumor Agents And
evelo f D pin l o g a D Matsumoto et al., J Develop Drugs 2014, 3:2 n r r u u g o s J Journal of Developing Drugs DOI: 10.4172/2329-6631.1000125 ISSN: 2329-6631 Research Article Open Access In vitro Synergistic Effects of Anthracycline Antitumor Agents and Fluconazole Against Azole-Resistant Candida albicans Clinical Isolates Matsumoto S, Kurakado S, Shiokama T, Ando Y, Aoki N, Cho O and Sugita T* Department of Microbiology, Meiji Pharmaceutical University, Kiyose, Tokyo Japan Abstract The number of azole-resistant Candida albicans clinical isolates is increasing. This study searched for compounds that are functionally synergistic with fluconazole against azole-resistant C. albicans strains. Synergistic effects were evaluated using the checkerboard method in a time-kill study using anthracycline antitumor agents and azole-resistant C. albicans strains. Of the five anthracycline agents examined, aclarubicin by itself had antifungal effects, whereas daunorubicin, doxorubicin, epirubicin, and idarubicin did not show antifungal effects alone, but did exert dose- and time- dependent synergistic effects with fluconazole against the C. albicans strains. No antitumor agent other than anthracycline exhibited an anti-Candida effect. Anthracycline compounds may therefore be useful as seeds for development of new antifungal agents. Keywords: Anthracycline; antitumor agent; azole-resistant Candida Materials and Methods albicans; synergy Strains used Introduction Twelve azole-resistant Candida albicans strains obtained from Candida albicans is the most frequently observed opportunistic patients’ blood were examined in this study. All strains were cultured fungal pathogen and causes deep-seated fungal infection, mainly on Sabouraud dextrose agar (SDA) plates at 37°C. -

Comparative Transcriptome Analysis Reveals Key Epigenetic Targets in SARS-Cov-2 Infection
www.nature.com/npjsba ARTICLE OPEN Comparative transcriptome analysis reveals key epigenetic targets in SARS-CoV-2 infection Marisol Salgado-Albarrán 1,2,7, Erick I. Navarro-Delgado 3,7, Aylin Del Moral-Morales 1,7, Nicolas Alcaraz 4, Jan Baumbach 5,6, ✉ ✉ Rodrigo González-Barrios3 and Ernesto Soto-Reyes 1 COVID-19 is an infection caused by SARS-CoV-2 (Severe Acute Respiratory Syndrome coronavirus 2), which has caused a global outbreak. Current research efforts are focused on the understanding of the molecular mechanisms involved in SARS-CoV-2 infection in order to propose drug-based therapeutic options. Transcriptional changes due to epigenetic regulation are key host cell responses to viral infection and have been studied in SARS-CoV and MERS-CoV; however, such changes are not fully described for SARS-CoV-2. In this study, we analyzed multiple transcriptomes obtained from cell lines infected with MERS-CoV, SARS-CoV, and SARS-CoV-2, and from COVID-19 patient-derived samples. Using integrative analyses of gene co-expression networks and de-novo pathway enrichment, we characterize different gene modules and protein pathways enriched with Transcription Factors or Epifactors relevant for SARS-CoV-2 infection. We identified EP300, MOV10, RELA, and TRIM25 as top candidates, and more than 60 additional proteins involved in the epigenetic response during viral infection that has therapeutic potential. Our results show that targeting the epigenetic machinery could be a feasible alternative to treat COVID-19. npj Systems Biology and Applications (2021) 7:21 ; https://doi.org/10.1038/s41540-021-00181-x 1234567890():,; INTRODUCTION hallmark of active chromatin)10, histone acetylation in H3 and The coronavirus family (CoV) are non-segmented, positive-sense, H4 histones, and increased levels of H4K20me2 and unmodified 11 and enveloped RNA viruses that have been identified as the cause H3K36 and H4K79 have been reported . -

Review Article
REVIEW ARTICLE Chemotherapy advances in small-cell lung cancer Bryan A. Chan1,2, Jermaine I. G. Coward1,2,3 1Mater Adult Hospital, Department of Medical Oncology, Raymond Terrace, Brisbane, QLD 4101, Australia; 2School of Medicine, University of Queensland, St Lucia, Brisbane, QLD 4072, Australia; 3Inflammation & Cancer Therapeutics Group, Mater Research, Level 4, Translational Research Institute, Woolloongabba, Brisbane, QLD 4102, Australia ABSTRACT Although chemotherapeutic advances have recently been heralded in lung adenocarcinomas, such success with small-cell lung cancer (SCLC) has been ominously absent. Indeed, the dismal outlook of this disease is exemplified by the failure of any significant advances in first line therapy since the introduction of the current standard platinum-etoposide doublet over 30 years ago. Moreover, such sluggish progress is compounded by the dearth of FDA-approved agents for patients with relapsed disease. However, over the past decade, novel formulations of drug classes commonly used in SCLC (e.g. topoisomerase inhibitors, anthracyclines, alkylating and platinum agents) are emerging as potential alternatives that could effectively add to the armamentarium of agents currently at our disposal. This review is introduced with an overview on the historical development of chemotherapeutic regimens used in this disease and followed by the recent encouraging advances witnessed in clinical trials with drugs such as amrubicin and belotecan which are forging new horizons for future treatment algorithms. KEY WORDS Small cell lung cancer (SCLC); amrubicin; belotecan; picoplatin; relapsed SCLC J Thorac Dis 2013;5(S5):S565-S578. doi: 10.3978/j.issn.2072-1439.2013.07.43 Introduction cigarette smoking 20 years prior, but is now slowly decreasing due to changing smoking patterns (2). -
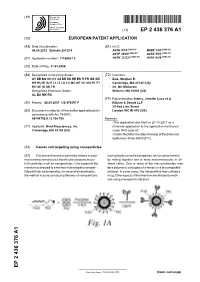
Cancer Cell Targeting Using Nanoparticles
(19) & (11) EP 2 436 376 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 04.04.2012 Bulletin 2012/14 A61K 9/14 (2006.01) B82B 1/00 (2006.01) A61P 35/00 (2006.01) A61K 9/51 (2006.01) (2006.01) (2006.01) (21) Application number: 11186037.5 A61K 31/337 A61K 9/48 (22) Date of filing: 31.03.2008 (84) Designated Contracting States: (72) Inventors: AT BE BG CH CY CZ DE DK EE ES FI FR GB GR • Zale, Stephen E. HR HU IE IS IT LI LT LU LV MC MT NL NO PL PT Cambridge, MA 02142 (US) RO SE SI SK TR • Ali, Mir Mikkaram Designated Extension States: Woburn, MA 01801 (US) AL BA MK RS (74) Representative: Harris, Jennifer Lucy et al (30) Priority: 28.09.2007 US 976197 P Kilburn & Strode LLP 20 Red Lion Street (62) Document number(s) of the earlier application(s) in London WC1R 4PJ (GB) accordance with Art. 76 EPC: 08744752.0 / 2 136 788 Remarks: •This application was filed on 20-10-2011 as a (71) Applicant: Bind Biosciences, Inc. divisional application to the application mentioned Cambridge, MA 02139 (US) under INID code 62. •Claims filed after the date of receipt of the divisional application (Rule 68(4) EPC). (54) Cancer cell targeting using nanoparticles (57) The present invention generally relates to poly- having highly controlled properties, which can be formed mersand macromolecules, inparticular, to polymersuse- by mixing together two or more macromolecules in dif- ful in particles such as nanoparticles.