Neuromuscular Junction Cases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dental Plexopathy Vesta Guzeviciene, Ricardas Kubilius, Gintautas Sabalys
SCIENTIFIC ARTICLES Stomatologija, Baltic Dental and Maxillofacial Journal, 5:44-47, 2003 Dental Plexopathy Vesta Guzeviciene, Ricardas Kubilius, Gintautas Sabalys SUMMARY Aim and purpose of the study were: 1) to study and compare unfavorable factors playing role in the development of upper teeth plexitis and upper teeth plexopathy; 2) to study peculiarities of clinical manifestation of upper teeth plexitis and upper teeth plexopathy, and to establish their diagnostic value; 3) to optimize the treatment. The results of examination and treatment of 79 patients with upper teeth plexitis (UTP-is) and 63 patients with upper teeth plexopathy (UTP-ty) are described in the article. Questions of the etiology, pathogenesis and differential diagnosis are discussed, methods of complex medicamental and surgical treatment are presented. Keywords: atypical facial neuralgia, atypical odontalgia, atypical facial pain, vascular toothache. PREFACE Besides the common clinical tests, in order to ana- lyze in detail the etiology and pathogenesis of the afore- Usually the injury of the trigeminal nerve is re- mentioned disease, its clinical manifestation and pecu- lated to the pathology of the teeth neural plexuses. liarities, we performed specific examinations such as According to the literature data, injury of the upper orthopantomography of the infraorbital canals, mea- teeth neural plexuses makes more than 7% of all sured the velocity of blood flow in the infraorbital blood neurostomatologic diseases. Many terms are used in vessels (doplerography), examined the pain threshold literature to characterize the clinical symptoms com- of facial skin and oral mucous membrane in acute pe- plex of the above-mentioned pathology. Some authors riod and remission, and evaluated the role that the state (1, 2, 3) named it dental plexalgia or dental plexitis. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies
Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies a, b Leo H. Wang, MD, PhD *, Michael D. Weiss, MD KEYWORDS Radial Posterior interosseous Neuropathy Electrodiagnostic study KEY POINTS The radial nerve subserves the extensor compartment of the arm. Radial nerve lesions are common because of the length and winding course of the nerve. The radial nerve is in direct contact with bone at the midpoint and distal third of the humerus, and therefore most vulnerable to compression or contusion from fractures. Electrodiagnostic studies are useful to localize and characterize the injury as axonal or demyelinating. Radial neuropathies at the midhumeral shaft tend to have good prognosis. INTRODUCTION The radial nerve is the principal nerve in the upper extremity that subserves the extensor compartments of the arm. It has a long and winding course rendering it vulnerable to injury. Radial neuropathies are commonly a consequence of acute trau- matic injury and only rarely caused by entrapment in the absence of such an injury. This article reviews the anatomy of the radial nerve, common sites of injury and their presentation, and the electrodiagnostic approach to localizing the lesion. ANATOMY OF THE RADIAL NERVE Course of the Radial Nerve The radial nerve subserves the extensors of the arms and fingers and the sensory nerves of the extensor surface of the arm.1–3 Because it serves the sensory and motor Disclosures: Dr Wang has no relevant disclosures. Dr Weiss is a consultant for CSL-Behring and a speaker for Grifols Inc. and Walgreens. He has research support from the Northeast ALS Consortium and ALS Therapy Alliance. -

Isolated Brachialis Muscle Atrophy
A Case Report & Literature Review Isolated Brachialis Muscle Atrophy John W. Karl, MD, MPH, Michael T. Krosin, MD, and Robert J. Strauch, MD or sensory complaints. His medical history was otherwise Abstract unremarkable. Physical examination revealed obvious wast- Isolated brachialis muscle atrophy, a rare entity with ing of the right brachialis muscle, most notable on the lateral few reported cases in the literature, is explained by a aspect of the distal arm (Figures 1, 2A, 2B). His biceps muscle variety of etiologies. We present a case of unilateral, was functioning with full strength and had a normal bulk. He isolated brachialis muscle atrophy that likely resulted had a normal range of active and passive motion, including from neuralgic amyotrophy. full extension and flexion of both elbows, as well as complete Figure 1. Frontal view of both arms: note the brachialis atrophy solated brachialis muscle atrophy has been rarely reported. (solid arrow) on the right side, although the biceps contracts well. Among the few cases in the literature, 1 was attributed I to a presumed compartment syndrome,1 1 to a displaced clavicle fracture,2 and 3 to neuralgic amyotrophy.3,4 We pres- ent a case of isolated brachialis muscle atrophy of unknown etiology, the presentation of which is consistent with neuralgic amyotrophy, also known as Parsonage-Turner syndrome or brachial plexitis. The patient provided written informed consent for print and electronic publication of this case report. AJO Case Report A 37-year-old right-handed highway worker presented for eval- uation of right-arm muscle atrophy. One year earlier, while lift- ing heavy bags at work, he felt a painful strain in his right arm, although there was no bruising or swelling. -

New Insights in Lumbosacral Plexopathy
New Insights in Lumbosacral Plexopathy Kerry H. Levin, MD Gérard Said, MD, FRCP P. James B. Dyck, MD Suraj A. Muley, MD Kurt A. Jaeckle, MD 2006 COURSE C AANEM 53rd Annual Meeting Washington, DC Copyright © October 2006 American Association of Neuromuscular & Electrodiagnostic Medicine 2621 Superior Drive NW Rochester, MN 55901 PRINTED BY JOHNSON PRINTING COMPANY, INC. C-ii New Insights in Lumbosacral Plexopathy Faculty Kerry H. Levin, MD P. James. B. Dyck, MD Vice-Chairman Associate Professor Department of Neurology Department of Neurology Head Mayo Clinic Section of Neuromuscular Disease/Electromyography Rochester, Minnesota Cleveland Clinic Dr. Dyck received his medical degree from the University of Minnesota Cleveland, Ohio School of Medicine, performed an internship at Virginia Mason Hospital Dr. Levin received his bachelor of arts degree and his medical degree from in Seattle, Washington, and a residency at Barnes Hospital and Washington Johns Hopkins University in Baltimore, Maryland. He then performed University in Saint Louis, Missouri. He then performed fellowships at a residency in internal medicine at the University of Chicago Hospitals, the Mayo Clinic in peripheral nerve and electromyography. He is cur- where he later became the chief resident in neurology. He is currently Vice- rently Associate Professor of Neurology at the Mayo Clinic. Dr. Dyck is chairman of the Department of Neurology and Head of the Section of a member of several professional societies, including the AANEM, the Neuromuscular Disease/Electromyography at Cleveland Clinic. Dr. Levin American Academy of Neurology, the Peripheral Nerve Society, and the is also a professor of medicine at the Cleveland Clinic College of Medicine American Neurological Association. -

Whole Exome Sequencing Gene Package Intellectual Disability, Version 9.1, 31-1-2020
Whole Exome Sequencing Gene package Intellectual disability, version 9.1, 31-1-2020 Technical information DNA was enriched using Agilent SureSelect DNA + SureSelect OneSeq 300kb CNV Backbone + Human All Exon V7 capture and paired-end sequenced on the Illumina platform (outsourced). The aim is to obtain 10 Giga base pairs per exome with a mapped fraction of 0.99. The average coverage of the exome is ~50x. Duplicate and non-unique reads are excluded. Data are demultiplexed with bcl2fastq Conversion Software from Illumina. Reads are mapped to the genome using the BWA-MEM algorithm (reference: http://bio-bwa.sourceforge.net/). Variant detection is performed by the Genome Analysis Toolkit HaplotypeCaller (reference: http://www.broadinstitute.org/gatk/). The detected variants are filtered and annotated with Cartagenia software and classified with Alamut Visual. It is not excluded that pathogenic mutations are being missed using this technology. At this moment, there is not enough information about the sensitivity of this technique with respect to the detection of deletions and duplications of more than 5 nucleotides and of somatic mosaic mutations (all types of sequence changes). HGNC approved Phenotype description including OMIM phenotype ID(s) OMIM median depth % covered % covered % covered gene symbol gene ID >10x >20x >30x A2ML1 {Otitis media, susceptibility to}, 166760 610627 66 100 100 96 AARS1 Charcot-Marie-Tooth disease, axonal, type 2N, 613287 601065 63 100 97 90 Epileptic encephalopathy, early infantile, 29, 616339 AASS Hyperlysinemia, -

Psykisk Utviklingshemming Og Forsinket Utvikling
Psykisk utviklingshemming og forsinket utvikling Genpanel, versjon v03 Tabellen er sortert på gennavn (HGNC gensymbol) Navn på gen er iht. HGNC >x10 Andel av genet som har blitt lest med tilfredstillende kvalitet flere enn 10 ganger under sekvensering x10 er forventet dekning; faktisk dekning vil variere. Gen Gen (HGNC Transkript >10x Fenotype (symbol) ID) AAAS 13666 NM_015665.5 100% Achalasia-addisonianism-alacrimia syndrome OMIM AARS 20 NM_001605.2 100% Charcot-Marie-Tooth disease, axonal, type 2N OMIM Epileptic encephalopathy, early infantile, 29 OMIM AASS 17366 NM_005763.3 100% Hyperlysinemia OMIM Saccharopinuria OMIM ABCB11 42 NM_003742.2 100% Cholestasis, benign recurrent intrahepatic, 2 OMIM Cholestasis, progressive familial intrahepatic 2 OMIM ABCB7 48 NM_004299.5 100% Anemia, sideroblastic, with ataxia OMIM ABCC6 57 NM_001171.5 93% Arterial calcification, generalized, of infancy, 2 OMIM Pseudoxanthoma elasticum OMIM Pseudoxanthoma elasticum, forme fruste OMIM ABCC9 60 NM_005691.3 100% Hypertrichotic osteochondrodysplasia OMIM ABCD1 61 NM_000033.3 77% Adrenoleukodystrophy OMIM Adrenomyeloneuropathy, adult OMIM ABCD4 68 NM_005050.3 100% Methylmalonic aciduria and homocystinuria, cblJ type OMIM ABHD5 21396 NM_016006.4 100% Chanarin-Dorfman syndrome OMIM ACAD9 21497 NM_014049.4 99% Mitochondrial complex I deficiency due to ACAD9 deficiency OMIM ACADM 89 NM_000016.5 100% Acyl-CoA dehydrogenase, medium chain, deficiency of OMIM ACADS 90 NM_000017.3 100% Acyl-CoA dehydrogenase, short-chain, deficiency of OMIM ACADVL 92 NM_000018.3 100% VLCAD -
Bilateral Brachial Plexopathy As an Initial Presentation in a Newly-Diagnosed, Uncontrolled Case of Diabetes Mellitus Pica E C, Verma K K
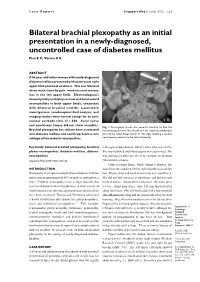
Case Report Singapore Med J 2008; 49(2) : e29 Bilateral brachial plexopathy as an initial presentation in a newly-diagnosed, uncontrolled case of diabetes mellitus Pica E C, Verma K K ABSTRACT A 55-year-old Indian woman with newly-diagnosed diabetes mellitus presented with acute onset right upper limb proximal weakness. This was followed three weeks later by pain, weakness and sensory loss in the left upper limb. Electrodiagnosis showed patchy multiple proximal and distal axonal neuropathies in both upper limbs, consistent with bilateral brachial neuritis. Laboratory investigations, cerebrospinal fluid analysis, and imaging studies were normal except for an anti- nuclear antibody titre of 1:640. Sural nerve and quadriceps biopsy did not show vasculitis. Fig. 1 Photograph shows the patient’s inability to flex the Brachial plexopathy has seldom been associated interphalangeal joint of the thumb and the distal interphalangeal with diabetes mellitus and could represent a rare joint of the index finger (pinch or OK sign) implying a median subtype of the diabetic neuropathies. nerve lesion proximal to the wrist bilaterally. Keywords: bilateral brachial plexopathy, brachial with signs of dehydration. HbA1c at the time was 14.2%. plexus neuropathies, diabetes mellitus, diabetic She was hydrated and blood sugars were optimised. She neuropathies was discharged after one week to continue medication Singapore Med J 2008; 49(2): e29-e32 (Metformin) at home. Upon reaching home, while taking a shower, she INTRODUCTION found that she could not lift her right shoulder to wash her Neuropathy is a frequent complication of diabetes mellitus hair. Elbow, wrist and hand movements were unaffected. -

Brachial Plexopathy Following High-Dose Melphalan and Autologous Peripheral Blood Stem Cell Transplantation
Bone Marrow Transplantation (2010) 45, 951–952 & 2010 Macmillan Publishers Limited All rights reserved 0268-3369/10 $32.00 www.nature.com/bmt LETTER TO THE EDITOR Brachial plexopathy following high-dose melphalan and autologous peripheral blood stem cell transplantation Bone Marrow Transplantation (2010) 45, 951–952; Tone and power were normal throughout, lower limb deep doi:10.1038/bmt.2009.243; published online 21 September 2009 tendon reflexes were absent and plantars were downgoing. Magnetic resonance imaging of the whole spine at this point revealed widespread myelomatous involvement of the Neuromuscular pathologies are a recognized complication bony spine but no cord compromise. Thalidomide was of SCT, often occurring as a result of infection or continued with no alteration in dosage. The patient haemorrhage, but also in association with GVHD follow- subsequently underwent a PBSCT with high-dose melpha- ing allogeneic SCT.1 The published literature on post- lan as the conditioning regime. transplant peripheral nervous system pathologies includes Within 14 days of stem-cell infusion the patient devel- descriptions of myasthenia gravis, Guillain-Barre´ oped progressive proximal weakness affecting predomi- syndrome, polymyositis and peripheral neuropathy.2–5 nantly the upper limbs. There was no neck pain or Ocular toxicity, radiculopathy and plexopathy have also involvement of bladder or bowel. Examination revealed rarely been reported. We report three cases of brachial bilateral wrist-drop with grade 3–4 weakness of the small plexopathy occurring after autologous peripheral blood muscles of the hand, elbow flexors and extensors and stem cell transplantation (PBSCT). shoulder abduction. Upper limb reflexes were absent. The neurological findings in the lower limbs were unchanged. -

Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies
Electrodiagnosis of Brachial Plexopathies and Proximal Upper Extremity Neuropathies Zachary Simmons, MD* KEYWORDS Brachial plexus Brachial plexopathy Axillary nerve Musculocutaneous nerve Suprascapular nerve Nerve conduction studies Electromyography KEY POINTS The brachial plexus provides all motor and sensory innervation of the upper extremity. The plexus is usually derived from the C5 through T1 anterior primary rami, which divide in various ways to form the upper, middle, and lower trunks; the lateral, posterior, and medial cords; and multiple terminal branches. Traction is the most common cause of brachial plexopathy, although compression, lacer- ations, ischemia, neoplasms, radiation, thoracic outlet syndrome, and neuralgic amyotro- phy may all produce brachial plexus lesions. Upper extremity mononeuropathies affecting the musculocutaneous, axillary, and supra- scapular motor nerves and the medial and lateral antebrachial cutaneous sensory nerves often occur in the context of more widespread brachial plexus damage, often from trauma or neuralgic amyotrophy but may occur in isolation. Extensive electrodiagnostic testing often is needed to properly localize lesions of the brachial plexus, frequently requiring testing of sensory nerves, which are not commonly used in the assessment of other types of lesions. INTRODUCTION Few anatomic structures are as daunting to medical students, residents, and prac- ticing physicians as the brachial plexus. Yet, detailed understanding of brachial plexus anatomy is central to electrodiagnosis because of the plexus’ role in supplying all motor and sensory innervation of the upper extremity and shoulder girdle. There also are several proximal upper extremity nerves, derived from the brachial plexus, Conflicts of Interest: None. Neuromuscular Program and ALS Center, Penn State Hershey Medical Center, Penn State College of Medicine, PA, USA * Department of Neurology, Penn State Hershey Medical Center, EC 037 30 Hope Drive, PO Box 859, Hershey, PA 17033. -

Painful Brachial Plexopathy: an Unusual Presentation of Polyarteritis Nodosa S
Postgrad Med J: first published as 10.1136/pgmj.58.679.311 on 1 May 1982. Downloaded from Postgraduate Medical Journal (May 1982) 58, 311-313 Painful brachial plexopathy: an unusual presentation of polyarteritis nodosa S. G. ALLAN* H. M. A. TOWLA* M.R.C.P. B. Med. Biol., M.B. C. C. SMITH* A. W. DOWNIE* F.R.C.P. F.R.C.P. J. C. CLARKt M.B., Ch.B. *Department ofMedicine, The Royal Infirmary, Foresterhill, Aberdeen tDepartment ofPathology, University ofAberdeen, Foresterhill Summary intact save for evidence of a right recurrent laryn- An elderly man was admitted to hospital with an geal nerve palsy on indirect laryngoscopy. There unusual painful bilateral brachial neuropathy, which was a flicker of left biceps contraction and grade 2/5 progressed in spite ofhigh dose corticosteroid therapy. power in the deltoids and adductors of the shoulders, Polyarteritis nodosa, characterized by widespread but otherwise total paralysis of the upper limbs. arteriolar involvement, was shown at post-mortem. Marked tenderness was noted over each brachial copyright. plexus, but there was neither muscle tenderness nor fasciculation. 'Glove' loss of all sensory modalities Introduction was present up to the elbows bilaterally, with hypo- The clinical presentations of polyarteritis nodosa tonicity and areflexia. There was minimal hip flexor are classically diverse, reflecting variable vascular weakness and absent left knee and both ankle involvement of many organs and tissues. Mono- reflexes without sensory abnormality or calf tender- neuritis multiplex is the most common neurological ness. Bladder and bowel functions were unaffected sequel (Ford and Siekert, 1965), but asymmetrical and examination otherwise unremarkable. -

Massive Indoor Cycling-Induced Rhabdomyolysis in a Patient With
CASE CoMMUNICATIONS IMAJ • VOL 14 • noveMber 2012 Massive Indoor Cycling-Induced Rhabdomyolysis in a Patient with Hereditary Neuropathy with Liability to Pressure Palsy Marganit Benish PhD1, Inna Zeitlin MD2, Dana Deshet MD2 and Yitzhak Beigel MD1,2 1Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv, Israel 2Department of Medicine D, Wolfson Medical Center, Holon, Israel profoundly decreased. Severe pain exercise-induced rhabdomyolysis, KEY WORDS: PATIENT DESCRIPTION and stiffness were observed when she hereditary neuropathy with liability A 21 year old female was hospitalized stretched both legs. She did not suffer to pressure palsy (HNPP), creatine kinase, indoor cycling, “spinning,” in December 2011 because of pain from any other medical condition and myoglobin and profound weakness in her thighs had no history of recent exposure to IMAJ 2012; 14: 712-714 rendering her unable to walk, and tea- medications, vaccines, alcohol drinking, colored urine. The muscular symptoms or any signs and symptoms of a viral had begun 5 days prior to her admis- infection. Laboratory results showed a sion, starting immediately after she had CK level of 132,170 U/L (range < 10–145 participated, for the first time in her U/L) and increased transaminase levels habdomyolysis is a condition charac- life, in an indoor-cycling class (“spin- (alanine transaminase 280 U/L (< 3–31 R terized by extended myolysis, marked ning”) lasting 45 minutes. The color U/L), aspartate transaminase 1256 U/L elevation of serum creatine kinase and of her urine changed and prompted (< 3–32 U/L) [Table], serum sodium myoglobinuria. Weakness, myalgia, and her to immediately seek medical care.