ISPUB.COM Politics Volume 7 Number 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

HEALTH Sep 31St, 2013 - Volume:1, Issue: 4
HEALTH Sep 31st, 2013 - Volume:1, Issue: 4 Epidemic control: Dengue counters set up at LGH IN THIS BULLETIN Seven more dengue patients confirmed in Mayo Hospital Lahore Punjab health department put on alert over Congo fever Health News 2-11 Dengue on the rise in Punjab Polio eradication: Provinces endorse three-year plan Healt deartments and Monitoring 12-13 Swat Declares Health Emergency Over Dengue bodies Publications WHO rings alarm over measles Anti –Measles drive delayed due to finance ministry stubbornness Balochistan EQ 2013 - Potentially 14 58m have no access to safe drinking water Affected Health Facilities Contamination risks: Think twice before you take a sip of your tap water Govt committed to making Pakistan polio-free: PM Health Response by Humanitarian 15-18 Precautionary measures: Health officials prepare to tackle Congo virus Post-natal screening: Sindh Assembly passes ‘newborn screening bill’ Partners in Awaran EQ - Balochistan PM lauds Bill Gates’ support on polio eradication in Pakistan LHC rebukes health DG in measles case District Health Profile Peshawar 19 Micro plan NID polio round from Sept Polio virus: BA voices fear Pakistanis might face travelling ban Urdu News 20-23 Meeting with PM: Donors share anguish over polio campaign First sexual health curriculum launched in Pakistan Health Maps 24-27 Balochistan Health department on high alert Pakistan lagging behind in child survival, maternal health development Health Directory 28-46 WHO polio chief in Pakistan honoured DRUG USE IN PAKISTAN 2013 KECH - POTENTIALLY -

Health Department (2010-13)
Version II DraftDraft for forDiscussion Discussion MEDIUM TERM BUDGETARY FRAMEWORK (MTBF) (2010-13) Volume - II Medium Term Budgetary Framework (MTBF) – Health Department (2010-13) Government of the Punjab Health Department 27th July 2010 i Draft for Discussion Table of Contents MESSAGE FROM SECRETARY HEALTH DEPARTMENT 1 ACRONYMS 2 SECTION I 4 1. Introduction and Background to the Department 4 1.1. Particulars of the Department 4 1.2. Vision Statement 4 1.3. Policy Objectives 4 1.4. Overview of Health Sector in Pakistan 5 1.5. Overview of Health Sector in Punjab 6 1.6. Organizational Structure and Functions of the Department 7 1.6.1. About the Department 7 1.6.2. Key Functions of the Department: 8 1.6.3. Planning & Budgeting Process in the Department 9 1.7. Share of Health Budget in Provincial Budget Outlay 11 2. Priorities in the medium term (2010-13) 12 3. Medium Term Budget Estimates (2010-13) 13 3.1 Summary of MTBF Estimates (2010-13) 13 3.2 MTBF Allocations by Policy Objectives 16 3.3 MTBF Allocations – by Object Classification 18 3.4 MTBF Allocations – by Functional Classification 21 3.5 MTBF Allocations – by Cross Classification 23 3.6 Key Inputs and Outputs – Current Budget 29 3.7 Selective Outputs for Large Development Schemes 36 3.8 Recurrent Impact of Development Projects 40 APPENDIX – B: EXPLANATORY NOTES TO MTBF ESTIMATES (2010-13) 42 APPENDIX – C: MTBF AT HEALTH DEPARTMENT 46 GLOSSARY OF TERMS 50 SECTION II 53 PART – A: DETAILS OF CURRENT BUDGET ESTIMATES 2010-13 53 i Draft for Discussion PART – B: DETAILS OF DEVELOPMENT BUDGET ESTIMATES 2010-13 221 ii Draft for Discussion MESSAGE FROM SECRETARY HEALTH DEPARTMENT This was second year of MTBF reforms in the Health Department. -

Compact for Impact Strategic Framework for Private Sector Engagement for the Sdgs
Compact for Impact Strategic Framework for Private Sector Engagement for the SDGs Farrukh Moriani ACRONYMS ADB Asian Development Bank ADPs Annual Development Plans APNS All Pakistan Newspapers Society BCtA Business Call to Action BISP Benazir Income Support Program CERB Centre of Excellence on Responsible Business CPEC China-Pakistan Economic Corridor CSO Civil Society Organization DFID Department for International Development EU European Union FBR Federal Board of Revenue FCCI Faisalabad Chambers of Commerce and Industries FPCCI Federation of Pakistan Chambers of Commerce and Industries FY Financial Year GC Global Compact GDP Gross Domestic Product GOP Government of Pakistan ICAP Institute of Chartered Accountants of Pakistan ICCI Islamabad Chambers of Commerce and Industry ICG Institute for Corporate Governance ITC International Trade Centre IICPSD Istanbul International Centre for Private Sector in Development KCCI Karachi Chambers of Commerce and Industries KP Khyber Pakhtunkhwa KPI Key Performance Indicators KPITB KP IT Board MOPDR Ministry of Planning, Development and Reforms MTBF Medium Term Budgetary Framework NGO Non-Governmental Organization OCCI Overseas Chamber of Commerce and Industries PITB Punjab Information Technolog Board PBC Pakistan Business Council PRGMEA Pakistan Readymade Garments Exporters Association PSX Pakistan Stock Exchange QCCI Quetta Chamber of Commerce and Industry QSTCCI Quetta Small Traders Chamber of Commerce and Industry SBP State Bank of Pakistan SECP Securities and Exchange Corporation of Pakistan -
Health Bulletin Volume 2 Issue 6.Pdf
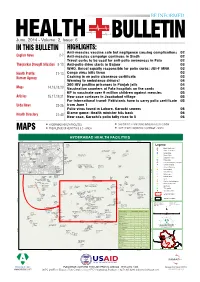
June, 2014 - Volume: 2, Issue: 6 IN THIS BULLETIN HIGHLIGHTS: Anti-measles vaccine safe but negligence causing complications 02 English News 2-7 Anti-measles campaign continues in Sindh 02 Travel curbs to be used for anti-polio awareness in Fata 02 Tharparkar Drought Situation 8-10 Anti-polio drive starts in Bajaur 03 WHO, Unicef equally responsible for polio curbs: JUI-F MNA 03 Health Profile: 11-13 Congo virus kills three 03 Kurram Agency Cashing in on polio clearance certificate 03 Warning to ambulance drivers! 04 300 HIV positive prisoners in Punjab jails 04 Maps 14,16,18,20 Vaccination counters at Fata hospitals on the cards 04 KP to vaccinate over 9 million children against measles 05 Articles 15,17,19,21 New case surfaces in Jacobabad village 05 For international travel: Pakistanis have to carry polio certificate 05 Urdu News 22-26 from June 1 Polio virus found in Lahore, Karachi sewers 06 Blame game: Health minister hits back 06 Health Directory 27-40 New case, Karachi's polio tally rises to 5 06 HYDERABAD HEALTH FACILITIES CHILDREN 12-23 MONTHS IMMUNIZATION - SINDH MAPS PREVALENCE OF HEPATITIS B & C - SINDH LADY HEALTH WORKERS COVERAGE - SINDH HYDERABAD HEALTH FACILITIES 68°21'30"E 68°22'0"E 68°22'30"E 68°23'0"E 68°23'30"E Hira Ultrasound Clinic Civil Sindh Awami Hospital Sindh Hospital Medical Aiwan E Clinic Store Quresh Legend Memon Clinic Seeja Rhc Taluka Hospital "' Basic Health Unit Clinic Hospital Muslim Khutri Soni Rohan Clinic And Charitable Clinic Irum Ulfat ÷Ó Children Hospital Meena Hospital Maternity Home Clinic Clinic -

General 4 February 2016
United Nations E/C.12/PAK/1 Economic and Social Council Distr.: General 4 February 2016 Original: English English, French and Spanish only Committee on Economic, Social and Cultural Rights Consideration of reports submitted by States parties under articles 16 and 17 of the International Covenant on Economic, Social and Cultural Rights Initial reports of States parties due in 2010 Pakistan* [Date received: 16 October 2015] * The present document is being issued without formal editing. GE.16-00186(E) *1600186* E/C.12/PAK/1 Introduction 1. The Government of Pakistan (GoP) signed the International Covenant on Economic, Social and Cultural Rights (ICESCR) on 3rd November, 2004 and ratified it on 17th April, 2008. In accordance with Articles 16 and 17 of the Covenant, which stipulate that a State Party must submit its implementation report in accordance with its treaty obligations, the Government of Pakistan is pleased to present its initial report to the Committee on Economic, Social and Cultural Rights (CESCR). 2. This report mainly contains information and developments from 2008 to 2014 which have been obtained from various stakeholders through detailed consultative meetings and through information made available by the Government. Furthermore, this report has been prepared in coordination with the Ministry of Law, Justice and Human Rights along with the contributions of various Ministries and Departments both at the Federal and the Provincial levels. The guidelines adopted by the CESCR on 18th November, 2008 have been followed for the preparation of this report. 3. Although Pakistan ratified the ICESCR in 2008, yet prior to this date the Government of Pakistan has been making efforts through a number of legislative and administrative measures for realization of economic, social and cultural rights of the people of Pakistan. -

Examining Multi-Level and Inter-Organizational Collaborative Response to Disasters: the Case of Pakistan Floods in 2010
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2013 Examining Multi-level And Inter-organizational Collaborative Response To Disasters: The Case Of Pakistan Floods In 2010 Sana Khosa University of Central Florida Part of the Public Administration Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Khosa, Sana, "Examining Multi-level And Inter-organizational Collaborative Response To Disasters: The Case Of Pakistan Floods In 2010" (2013). Electronic Theses and Dissertations, 2004-2019. 2890. https://stars.library.ucf.edu/etd/2890 EXAMINING MULTI-LEVEL AND INTER-ORGANIZATIONAL COLLABORATIVE RESPONSE TO DISASTERS: THE CASE OF PAKISTAN FLOODS IN 2010 by SANA KHOSA B.Sc. (Hons.) Lahore University of Management Sciences, Pakistan, 2005 M.P.A. University of Central Florida, 2010 A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the College of Health and Public Affairs at the University of Central Florida Orlando, Florida Fall Term 2013 Major Professor: Naim Kapucu © 2013 Sana Khosa ii ABSTRACT Catastrophic disasters are different than routine disasters and managing them requires the mobilization of inter-organizational, inter-governmental, cross-sectoral and international humanitarian support. The role of the international community through International Non- governmental Organizations (INGOs), and multi-lateral organizations such as the United Nations (UN) becomes imperative when the scale of the disaster is unprecedented and difficult for a country to manage on its own. -

Downloads/PIM-BRT.Pdf 95
- !"# $$%& ' ()(* +, $$%& !" # "$%&''('))& $%&''(*'&(+ &0 1 -/ 2 -/ # "$%&'&''**)+ " $ , -' ."$///' -' All rights reserved No part of this publication may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying and recording or by any information storage and retrieval system, without the permission of the publisher. © 2015 ALHASAN SYSTEMS PRIVATE LIMITED A Hi-Tech Knowledge Management, Business Psychology Modeling, and Publishing Company 205-C, 2nd Floor, Evacuee Trust Complex, Sector F-5/1, Islamabad, Pakistan 44000 Landline:+92.51.282.0449, +92.51.835.9288 Fax:+92.51.835.9287 195-1st floor, Deans Trade Center, Peshawar Cantt, Peshawar, Pakistan Landline:+92.91.525.3347 Email: [email protected] Website: www.alhasan.com Facebook: www.facebook.com/alhasan.com Twitter: @alhasansystems w3w address: *Alhasan 220 p.; 10x13 ISSN: 2312-3575 ISBN: 978-969-638-003-0 (Paper Book) 978-969-638-004-7 (Digital/ E-book) DISCLAIMER ! "!#!$#%#&'# ( ( ) ) ) ( * + ( ( ( , ) ( - ! "!#!$ #%#&'# ( . / 0 ) / 0 ! ( 1 2 ) ) ) 3 $ ( ( ( ( () () ( - ( ( , ! "!#!$#%#&'# ) ( - ( ( ) * . - ! "!#!$#%#&'# ( (4 ( 3 ) ! "!#!$#%#&'# -
HEALTH Nov 30Th, 2013 - Volume:1, Issue: 6
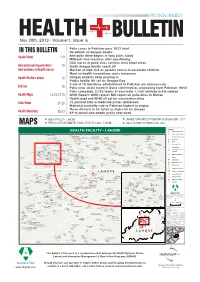
HEALTH Nov 30th, 2013 - Volume:1, Issue: 6 Polio cases in Pakistan pass 2012 total IN THIS BULLETIN No debate on dengue deaths Health News 1-9 Anti-polio drive begins in twin cities today’ Militants free teachers after questioning DCO warns of polio virus carriers from tribal areas Humanitarian Organizations’ 10 Sindh dengue deaths reach 30 Interventions in Health Sector Mardan at high-risk as parents refuse to vaccinate children Moot on health innovations starts tomorrow Health Profile Lahore 12 Dengue patients keep pouring in Public health: All set for Dengue Day 9 out of 10 injections administered in Pakistan are unnecessary Articles 16 Polio virus strain found in Syria confirmed as originating from Pakistan: WHO Polio campaign: 2,755 teams to vaccinate 1.18m children in Faisalabad Health Maps 13,15,17,19 WHO-Report: WHO rejects NIH report on polio virus in Multan Health dept and WHO all set for vaccination drive Urdu News 21-23 15 percent hike in medicine prices withdrawn Maternal mortality rate in Pakistan highest in region Three districts to be listed as high-risk for dengue Health Directory 25-37 KP to unveil new health policy next week HEALTH FACILITY - LAHORE LAHORE TOWN WISE DISTRIBUTION OF DRUG USERS - 2011 MAPS PERSONS WITH DISABILITIES (PWDS) STATISTICS 2012 - PUNJAB ACUTE RESPIRATORY INFECTION - 2012 Legend HEALTH FACILITY - LAHORE "' Basic Health Unit "' Sub Health Centre Mian Munshi Hospital Railway Hospital Arooj Hospital Maqssoda Family Government Nawaz Shalamar Hospital Iqra Surraya "' Shah Abdul Latif Health Lady Sharif Hospital Murad Clinic Rural Health Centre Azeem Family Faree Clinic Center Aitcheson Hospital Hospital Pathi Ground Mayo Hospital Clinic Ali Hospital "' Muhammad Physician Hospital Janki Devi Hospital Tanveer Cairns Railway Maham Clinic "' Eisha Hospital MCH Filter Clinic British Clinic Hospital Rabia Clinic Pasban Waqar Clinic Ultrasound Zanib Clinic "&F Puff Clinic Agakhan Health Center Aftab Clinic Society Homeopathic Hyder Umar Hospital Clinic Laboratory Neelam Dr. -

Chapter 6.1: Health
PUNJAB ECONOMIC | REPORT Health 6.1.0 Introduction Although Punjab’s overall health indicators are comparable to or slightly better than the national average, the province continues to face typical health problems and service challenges of the most densely populated and rural areas of the developing world. Across the globe, the healthcare sector expanding with rising economic prosperity, a changing disease prole, a growing global population and changing demographics that are resulting in a higher demand for healthcare services. A sound public health sector is critical for low-income segments of the population that already face a constrained access to adequate facilities at an aordable cost. e very same drivers for growth globally are also shaping the development of the healthcare sector in Pakistan. is sector has been expanding and is expected to continue its expansion as changing population ratios, higher incidences of chronic disease and wider health insurance coverage create upsurges in healthcare spending. Comprising more than half of Pakistan’s population, Punjab plays a key role in attainment of national health goals1. e province has shown better progress in comparison to other provinces, but lags behind countries like India, Bangladesh, Nepal and Sri Lanka that share similar socio-economic conditions as Punjab. One of the key reasons slowing down progress is the high rate of population growth. It is adversely impacting service delivery and widening regional inequities. For many in Punjab, cost of healthcare, in addition to cultural and social barri- ers, is a major obstacle preventing access to eective health services. e province also faces equity concerns in terms of access to health outcomes and services, much worse in the southern districts. -

Compact for Impact Strategic Framework for Private Sector Engagement for the Sdgs
Annexure K Compact for Impact Strategic Framework for Private Sector Engagement for the SDGs Farrukh Moriani ACRONYMS ADB Asian Development Bank ADPs Annual Development Plans APNS All Pakistan Newspapers Society BCtA Business Call to Action BISP Benazir Income Support Program CERB Centre of Excellence on Responsible Business CPEC China-Pakistan Economic Corridor CSO Civil Society Organization DFID Department for International Development EU European Union FBR Federal Board of Revenue FCCI Faisalabad Chambers of Commerce and Industries FPCCI Federation of Pakistan Chambers of Commerce and Industries FY Financial Year GC Global Compact GDP Gross Domestic Product GOP Government of Pakistan ICAP Institute of Chartered Accountants of Pakistan ICCI Islamabad Chambers of Commerce and Industry ICG Institute for Corporate Governance ITC International Trade Centre IICPSD Istanbul International Centre for Private Sector in Development KCCI Karachi Chambers of Commerce and Industries KP Khyber Pakhtunkhwa KPI Key Performance Indicators KPITB KP IT Board MOPDR Ministry of Planning, Development and Reforms MTBF Medium Term Budgetary Framework NGO Non-Governmental Organization OCCI Overseas Chamber of Commerce and Industries PITB Punjab Information Technolog Board PBC Pakistan Business Council PRGMEA Pakistan Readymade Garments Exporters Association PSX Pakistan Stock Exchange QCCI Quetta Chamber of Commerce and Industry QSTCCI Quetta Small Traders Chamber of Commerce and Industry SBP State Bank of Pakistan SECP Securities and Exchange Corporation of -

HRH Profile for Punjab 2012.Pdf
2012 Human Resources for Health Profile Punjab, Pakistan World Health Organization Human Resource for Health Profile – Punjab, Pakistan i ACKNOWLEDGEMENT The Human Resource for Health Profile for Punjab was undertaken after due approval of the Department of Health, Punjab. PHSRP, on behalf of the Department of Health, Government of Punjab provided full facilitation towards the HRH data collection. Their support was very valuable in accessing the Human Resource for Health Data that existed at varied sources in Punjab. The cooperation of all the focal persons nominated by the Punjab Health Sector Reform Programme (PHSRP) in facilitating the data collection was immense and needs a special acknowledgement. We greatly appreciate their valuable inputs, thoughts and the time and energy they devoted towards this assignment. We are particularly thankful to the Global Health Workforce Alliance (GHWA) for providing catalytic funding support and valuable inputs by sharing of resource materials that provided excellent guidance to the team working on the project. The devoted technical support to the study provided by Dr Muhammad Mahmood Afzal, Head of Country Coordination & Facilitation Team, GHWA is specially acknowledged. We would also like to take the opportunity to acknowledge with thanks the following partners of the Alliance, whose funding contribution to the Alliance has made this piece of work possible: . Bill and Melinda Gates Foundation . Canadian International Development Agency (CIDA) . French Development Agency/Agence Francaise de developpemenet (AFD) . Deutsche Gesellschaft fur International Zusammenarbeit (GIZ) Gmbh . Irish aid, department of Foreign Affairs . Norwegian Agency for Development Cooperation (NORAD) . UK Development for International Development (DFID) . United States Agency for International Development (USAID) The technical support, facilitation and guidance provided by the World Health Organization Country Office in Islamabad and the WHO office in Lahore remained extremely useful and valuable. -

Shaping 21St Century Public Health in Pakistan: an Actionable Agenda for Achieving Universal Health Coverage
Shaping 21st Century Public Health in Pakistan: An Actionable Agenda for Achieving Universal Health Coverage Dr. Muhammad Ali Chaudhry Ammara Khan Bismillah irr Rahman irr Rahim Shaping 21st Century Public Health in Pakistan: An Actionable Agenda for Achieving Universal Health Coverage Dr. Muhammad Ali Chaudhry Ammara Khan Tabadlab Working Paper 05 ISBN 978-969-7911-04-2 © Tabadlab Private Limited 2020 This work is licensed under the Creative Commons Attribution 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by/3.0 Available from: Tabadlab Mezzanine Floor, Beverly Centre, Blue Area, Islamabad, Pakistan, 44000. Tabadlab Private Limited is a for-profit think tank based out of Pakistan. Tel: +92 51 2726668 [email protected] The authors did not receive any financial support from any firm or person for this article or from any firm or person with a financial or political interest in this article. They are currently not an officer, director, or board member of any organization with an interest in this article. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of Tabadlab Private Limited. Shaping 21st Century Public Health in Pakistan: An Actionable Agenda for Achieving Universal Health Coverage Dr. Muhammad Ali Chaudhry, Ammara Khan Abstract Pakistan’s health system has struggled to effectively and efficiently serve the needs of an ever- growing population. Chronic challenges include prioritization, regulation, institutional alignment and governance. They have combined to produce major gaps in service delivery. Structural shifts in Pakistan’s demographic and disease profile are indicative of the urgent need to reform and reorient healthcare in the country.