Health Department (2010-13)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

HEALTH Sep 31St, 2013 - Volume:1, Issue: 4
HEALTH Sep 31st, 2013 - Volume:1, Issue: 4 Epidemic control: Dengue counters set up at LGH IN THIS BULLETIN Seven more dengue patients confirmed in Mayo Hospital Lahore Punjab health department put on alert over Congo fever Health News 2-11 Dengue on the rise in Punjab Polio eradication: Provinces endorse three-year plan Healt deartments and Monitoring 12-13 Swat Declares Health Emergency Over Dengue bodies Publications WHO rings alarm over measles Anti –Measles drive delayed due to finance ministry stubbornness Balochistan EQ 2013 - Potentially 14 58m have no access to safe drinking water Affected Health Facilities Contamination risks: Think twice before you take a sip of your tap water Govt committed to making Pakistan polio-free: PM Health Response by Humanitarian 15-18 Precautionary measures: Health officials prepare to tackle Congo virus Post-natal screening: Sindh Assembly passes ‘newborn screening bill’ Partners in Awaran EQ - Balochistan PM lauds Bill Gates’ support on polio eradication in Pakistan LHC rebukes health DG in measles case District Health Profile Peshawar 19 Micro plan NID polio round from Sept Polio virus: BA voices fear Pakistanis might face travelling ban Urdu News 20-23 Meeting with PM: Donors share anguish over polio campaign First sexual health curriculum launched in Pakistan Health Maps 24-27 Balochistan Health department on high alert Pakistan lagging behind in child survival, maternal health development Health Directory 28-46 WHO polio chief in Pakistan honoured DRUG USE IN PAKISTAN 2013 KECH - POTENTIALLY -

Pakistan Supports KL Summit Aimed at Development: FM NAB
12 Operational test run of Metro LHC issues stay order on ghee train on 10th prices set by govt By Our Staff Correspondent The LAHORE: The Lahore High Court (LHC) on Tuesday LAHORE: Punjab government has announced to make has issued stay order on the imposition of ghee prices set orange line metro train operational on Dec 10 in the light by the federal government. The decision was taken during of implementation upon the Supreme Court (SC) orders. the hearing of a case pertaining to the prices of the ghee. According to media reports, Chief Minister (CM) Pun - The plaintiff said that the government had issued noti - jab Usman Buzdar along with caravan of 250 people in - fication without consulting with the owners of ghee mills. cluding ministers and journalists will make an official test We cannot sell our product on the prices provided by the run on Dec 10 upon 27 kilometer route of train. LBahore, Wuednesdays, Deciembner 04, 2e019 Rasbi-uss -Sani 06, 1441 government, he clarified. —Online Pak will succeed OICCI announces with regard to results of IPR GSP-Plus: Sarwar LAHORE: Punjab Governor survey 2019 Chaudhry Muhammad Sarwar held im - KARACHI: Overseas Investors Chamber of Commerce portant meetings with Secretary of State and Industry (OICCI) on Tuesday announced the key find - of Foreign Affairs and Cooperation ings of its latest intellectual property tights survey. Teresa Ribeiro and Vice President of The OICCI 2019 IPR survey highlighted that IPR protec - Parliamentary Committee for Foreign tion continues to be of high importance for the business com - Affairs and Portugese communities Pedro munity of Pakistan, whereas there is need for better Filipe Soares. -

List of Delegations to the Seventieth Session of the General Assembly
UNITED NATIONS ST /SG/SER.C/L.624 _____________________________________________________________________________ Secretariat Distr.: Limited 18 December 2015 PROTOCOL AND LIAISON SERVICE LIST OF DELEGATIONS TO THE SEVENTIETH SESSION OF THE GENERAL ASSEMBLY I. MEMBER STATES Page Page Afghanistan......................................................................... 5 Chile ................................................................................. 47 Albania ............................................................................... 6 China ................................................................................ 49 Algeria ................................................................................ 7 Colombia .......................................................................... 50 Andorra ............................................................................... 8 Comoros ........................................................................... 51 Angola ................................................................................ 9 Congo ............................................................................... 52 Antigua and Barbuda ........................................................ 11 Costa Rica ........................................................................ 53 Argentina .......................................................................... 12 Côte d’Ivoire .................................................................... 54 Armenia ........................................................................... -

Meeting of the Technical Advisory Group on Poliomyelitis Eradication in Afghanistan and Pakistan
WHO-EM/POL/394/E Report on the Meeting of the Technical Advisory Group on Poliomyelitis Eradication in Afghanistan and Pakistan Islamabad, Pakistan 24–25 March 2011 © World Health Organization 2011 All rights reserved. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. Publications of the World Health Organization can be obtained from Distribution and Sales, World Health Organization, Regional Office for the Eastern Mediterranean, PO Box 7608, Nasr City, Cairo 11371, Egypt (tel: +202 2670 2535, fax: +202 2670 2492; email: [email protected]). -
Update on the Performance of Democratic Institutions
UPDATE ON THE PERFORMANCE OF DEMOCRATIC INSTITUTIONS MARCH 2021 2 UPDATE ON THE PERFORMANCE OF DEMOCRATIC INSTITUTIONS MARCH 2021 This update is meant to identify key developments during the month on Performance of Democratic Institutions in Pakistan with selected high- profile international developments included occasionally. IN THIS ISSUE 1 Senate Elections under Secret Ballot 2 Prime Minister Seeks Fresh Vote of Confidence 3 PM and PTI Ministers criticize the ECP 4 The Saga of Senate Chairman Election 5 PDM Alliance and Leader of the Opposition in the Senate 6 PTI, PPP Legislators clash in Sindh Assembly 7 Islamabad Security Dialogue: PM and COAS call for civilized relations with India 8 IHC orders removal of Lt General Asad Durrani’ s name from ECL 9 Senior Parliamentarians Council 10 NA-75 Bye Election and the Supreme Court 11 Peshawar High Court Adjourns Cases of Military Court Convicts 12 Supreme Court warns of uncontrolled Judicial overreach 13 Ministers threaten to attack Judge with Rockets if Sindh Assembly Membership suspended 14 Supreme Court allows DHA Quetta to develop schemes 15 Supreme Court Orders Restoration of Local Government in Punjab 16 Justice Qazi Faez Isa Case 17 Change in Federal Cabinet 18 Removal of HEC Chairman MARCH 2021 UPDATE ON THE PERFORMANCE OF DEMOCRATIC INSTITUTIONS 3 IN THIS ISSUE 19 Chairman, Deputy Chairman Senate call on PM and President 20 Fourth conference of Speakers of Parliaments ends in Turkey 21 COAS calls on PM 22 British High Commissioner calls on COAS 23 Qatari Land Forces Commander calls -

January 2017 NEWS COVERAGE PERIOD from JANUARY 23RD to JANUARY 29TH 2017 GROWING INEQUALITY THREATENS to PULL SOCIETIES APART the Express Tribune, January 23Rd, 2017
The Globalization Bulletin Poverty January 2017 NEWS COVERAGE PERIOD FROM JANUARY 23RD TO JANUARY 29TH 2017 GROWING INEQUALITY THREATENS TO PULL SOCIETIES APART The Express Tribune, January 23rd, 2017. Tehreem Husain Consider the following fact: Since 2015, the richest 1% has owned more wealth than the rest of the planet. A recent report “An economy for the 99 per cent” by Oxfam has put the gap between the rich and the poor to be far greater than what was feared before. It has claimed that just 8 men own the same wealth as 3.6 billion who make up the poorest half of the world. The report details how big businesses and the super-rich are fuelling inequality by evading taxes, driving down wages and using their power to influence politics. Winnie Byanyima, Executive Director of Oxfam International, has said that “it is obscene for so much wealth to be held in the hands of so few when 1 in 10 people survive on less than $2 a day. Inequality is trapping hundreds of millions in poverty; it is fracturing our societies and undermining democracy.” The report has laid emphasis on inequality as a major issue that is afflicting the world and has put forward some startling facts to prove how stark it is. Incomes of the poorest 10% of people increased by less than $3 a year between 1998 and 2011, while the incomes of the richest 1% increased 182 times. Growing inequality threatens to pull societies apart. It leads to increase in crime and insecurity and undermines the fight to end poverty. -

Compact for Impact Strategic Framework for Private Sector Engagement for the Sdgs
Compact for Impact Strategic Framework for Private Sector Engagement for the SDGs Farrukh Moriani ACRONYMS ADB Asian Development Bank ADPs Annual Development Plans APNS All Pakistan Newspapers Society BCtA Business Call to Action BISP Benazir Income Support Program CERB Centre of Excellence on Responsible Business CPEC China-Pakistan Economic Corridor CSO Civil Society Organization DFID Department for International Development EU European Union FBR Federal Board of Revenue FCCI Faisalabad Chambers of Commerce and Industries FPCCI Federation of Pakistan Chambers of Commerce and Industries FY Financial Year GC Global Compact GDP Gross Domestic Product GOP Government of Pakistan ICAP Institute of Chartered Accountants of Pakistan ICCI Islamabad Chambers of Commerce and Industry ICG Institute for Corporate Governance ITC International Trade Centre IICPSD Istanbul International Centre for Private Sector in Development KCCI Karachi Chambers of Commerce and Industries KP Khyber Pakhtunkhwa KPI Key Performance Indicators KPITB KP IT Board MOPDR Ministry of Planning, Development and Reforms MTBF Medium Term Budgetary Framework NGO Non-Governmental Organization OCCI Overseas Chamber of Commerce and Industries PITB Punjab Information Technolog Board PBC Pakistan Business Council PRGMEA Pakistan Readymade Garments Exporters Association PSX Pakistan Stock Exchange QCCI Quetta Chamber of Commerce and Industry QSTCCI Quetta Small Traders Chamber of Commerce and Industry SBP State Bank of Pakistan SECP Securities and Exchange Corporation of Pakistan -

ISPUB.COM Politics Volume 7 Number 1
The Internet Journal of World Health and Societal ISPUB.COM Politics Volume 7 Number 1 Governance and health sector development: a case study of Pakistan G Pappas, A Ghaffar, T Masud, A Hyder, S Siddiqi Citation G Pappas, A Ghaffar, T Masud, A Hyder, S Siddiqi. Governance and health sector development: a case study of Pakistan. The Internet Journal of World Health and Societal Politics. 2008 Volume 7 Number 1. Abstract BackgroundThe volatile political history of Pakistan has led to problems with governance overall and in the health sector. MethodsGovernance is defined by six domains of concern: voice and accountability; political stability and absence of violence; government effectiveness; regulatory quality; rule of law; and control of corruption. A review of the literature concerning health sector in Pakistan is interpreted using this conceptual framework. Results and DiscussionThe domains of governance are illustrated with examples from Pakistan's health sector. Two case studies, the President's Primary Health Care Initiative and the Tawana Pakistan Program are used to help understand how poor governance undermines important and positive political initiatives. Globalization effects governance through an evolving relationship between donors, multilateral agencies, and client states.ConclusionsGovernance issues are major barriers to improving health in Pakistan. This study contributes to our understanding of governance and the role of donors and multilateral agencies. BACKGROUND (Table 1) Failing states and the failure of aid have been associated Figure 1 with stagnation or deteriorations of health status in Table 1 Health Expenditure in Pakistan (Rs. Million) populations ( , ). Problems with governance, the poor performance of governments, have been used as part of the explanation of continued poor health in less developed countries ( ). -
Health Bulletin Volume 2 Issue 6.Pdf
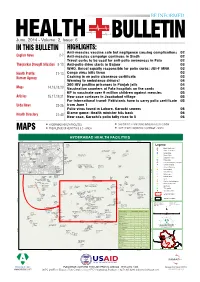
June, 2014 - Volume: 2, Issue: 6 IN THIS BULLETIN HIGHLIGHTS: Anti-measles vaccine safe but negligence causing complications 02 English News 2-7 Anti-measles campaign continues in Sindh 02 Travel curbs to be used for anti-polio awareness in Fata 02 Tharparkar Drought Situation 8-10 Anti-polio drive starts in Bajaur 03 WHO, Unicef equally responsible for polio curbs: JUI-F MNA 03 Health Profile: 11-13 Congo virus kills three 03 Kurram Agency Cashing in on polio clearance certificate 03 Warning to ambulance drivers! 04 300 HIV positive prisoners in Punjab jails 04 Maps 14,16,18,20 Vaccination counters at Fata hospitals on the cards 04 KP to vaccinate over 9 million children against measles 05 Articles 15,17,19,21 New case surfaces in Jacobabad village 05 For international travel: Pakistanis have to carry polio certificate 05 Urdu News 22-26 from June 1 Polio virus found in Lahore, Karachi sewers 06 Blame game: Health minister hits back 06 Health Directory 27-40 New case, Karachi's polio tally rises to 5 06 HYDERABAD HEALTH FACILITIES CHILDREN 12-23 MONTHS IMMUNIZATION - SINDH MAPS PREVALENCE OF HEPATITIS B & C - SINDH LADY HEALTH WORKERS COVERAGE - SINDH HYDERABAD HEALTH FACILITIES 68°21'30"E 68°22'0"E 68°22'30"E 68°23'0"E 68°23'30"E Hira Ultrasound Clinic Civil Sindh Awami Hospital Sindh Hospital Medical Aiwan E Clinic Store Quresh Legend Memon Clinic Seeja Rhc Taluka Hospital "' Basic Health Unit Clinic Hospital Muslim Khutri Soni Rohan Clinic And Charitable Clinic Irum Ulfat ÷Ó Children Hospital Meena Hospital Maternity Home Clinic Clinic -

CCI Annual Report 2017-18
Annual Report 2017-18 3Annual Report of CCI 2017-18 TABLE OF CONTENTS iii PREFACE v EXECUTIVE SUMMARY nd th Chapter-1 32 MEETING OF CCI HELD ON 25 AUGUST, 2017 1 2017-18 rd th Chapter-2 33 MEETING OF CCI HELD ON 13 NOVEMBER, 2017 9 2017-18 th th Chapter-3 34 MEETING OF CCI HELD ON 24 NOVEMBER, 2017 13 th th Chapter-4 35 MEETING OF CCI HELD ON 26 FEBRUARY, 2018 25 2017-18 th th Chapter-5 36 MEETING OF CCI HELD ON 27 MARCH, 2018 37 2017-18 th th Chapter-6 37 MEETING OF CCI HELD ON 24 APRIL, 2018 43 th th Chapter-7 38 MEETING OF CCI HELD ON 27 MAY, 2018 49 2017-18 53 Chapter-8 CONSTITUTIONAL PROVISIONS REGARDING CCI 2017-18 59 Chapter-9 INSTITUTIONAL HISTORY 2017-18 65 Chapter-10 RULES OF PROCEDURE OF CCI, 2010 75 Chapter-11 LANDMARK ACHIEVEMENTS OF CCI 2017-18 79 Chapter-12 COMPOSITION OF CCI 2017-18 ABBREVAITIONS 82 i Annual Report of CCI 2017-18 ii Annual Report of CCI 2017-18 PREFACE I consider it my privilege to prepare the eighth report of the Council of Common Interests for presentation to both the houses of the Parliament under Article 153 (4) of the Constitution of Islamic Republic of Pakistan. 2. The 18th Constitutional amendment was the outcome of a consensus with far-reaching impact on the subjects enumerated in Federal Legislative List (Part- II). In CCI, the Federation and Federating Units deliberate upon the issues of national importance and resolve the same amicably with the decision of majority. -

General 4 February 2016
United Nations E/C.12/PAK/1 Economic and Social Council Distr.: General 4 February 2016 Original: English English, French and Spanish only Committee on Economic, Social and Cultural Rights Consideration of reports submitted by States parties under articles 16 and 17 of the International Covenant on Economic, Social and Cultural Rights Initial reports of States parties due in 2010 Pakistan* [Date received: 16 October 2015] * The present document is being issued without formal editing. GE.16-00186(E) *1600186* E/C.12/PAK/1 Introduction 1. The Government of Pakistan (GoP) signed the International Covenant on Economic, Social and Cultural Rights (ICESCR) on 3rd November, 2004 and ratified it on 17th April, 2008. In accordance with Articles 16 and 17 of the Covenant, which stipulate that a State Party must submit its implementation report in accordance with its treaty obligations, the Government of Pakistan is pleased to present its initial report to the Committee on Economic, Social and Cultural Rights (CESCR). 2. This report mainly contains information and developments from 2008 to 2014 which have been obtained from various stakeholders through detailed consultative meetings and through information made available by the Government. Furthermore, this report has been prepared in coordination with the Ministry of Law, Justice and Human Rights along with the contributions of various Ministries and Departments both at the Federal and the Provincial levels. The guidelines adopted by the CESCR on 18th November, 2008 have been followed for the preparation of this report. 3. Although Pakistan ratified the ICESCR in 2008, yet prior to this date the Government of Pakistan has been making efforts through a number of legislative and administrative measures for realization of economic, social and cultural rights of the people of Pakistan. -

Examining Multi-Level and Inter-Organizational Collaborative Response to Disasters: the Case of Pakistan Floods in 2010
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2013 Examining Multi-level And Inter-organizational Collaborative Response To Disasters: The Case Of Pakistan Floods In 2010 Sana Khosa University of Central Florida Part of the Public Administration Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Khosa, Sana, "Examining Multi-level And Inter-organizational Collaborative Response To Disasters: The Case Of Pakistan Floods In 2010" (2013). Electronic Theses and Dissertations, 2004-2019. 2890. https://stars.library.ucf.edu/etd/2890 EXAMINING MULTI-LEVEL AND INTER-ORGANIZATIONAL COLLABORATIVE RESPONSE TO DISASTERS: THE CASE OF PAKISTAN FLOODS IN 2010 by SANA KHOSA B.Sc. (Hons.) Lahore University of Management Sciences, Pakistan, 2005 M.P.A. University of Central Florida, 2010 A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the College of Health and Public Affairs at the University of Central Florida Orlando, Florida Fall Term 2013 Major Professor: Naim Kapucu © 2013 Sana Khosa ii ABSTRACT Catastrophic disasters are different than routine disasters and managing them requires the mobilization of inter-organizational, inter-governmental, cross-sectoral and international humanitarian support. The role of the international community through International Non- governmental Organizations (INGOs), and multi-lateral organizations such as the United Nations (UN) becomes imperative when the scale of the disaster is unprecedented and difficult for a country to manage on its own.